
Abstract
Background
The rise of telemedicine has brought significant changes to patient care, especially regarding the experience of empathy and connection during consultations. Understanding how telemedicine compares to in-person visits in terms of patient–physician interactions and the perception of empathy is crucial for optimizing telehealth services.
Objectives
This study aims to compare patient–physician interaction ratings between telemedicine and in-person visits across the 10 items of the Consultation and Relational Empathy (CARE) measure. Additionally, it seeks to identify any significant differences in interaction ratings between male and female patients within these contexts.
Methods
A cross-sectional study was conducted involving 320 participants who had either telemedicine or in-person consultations. Participants were assigned to the telehealth or in-person group based on the type of consultation they experienced. The CARE measure was utilized to capture patient's perspective of the quality of the interaction. Statistical analyses were performed to compare the ratings between the two groups.
Results
The study found no significant differences in overall CARE measure ratings between telemedicine and in-person visits. However, male patients reported higher satisfaction with telemedicine on several items compared to in-person visits, whereas female patients showed no significant differences in their ratings.
Conclusions
Telemedicine is as effective as in-person visits in maintaining high-quality patient–physician interactions. The findings also suggest gender-specific preferences that could inform the optimization of telemedicine practices. Further research is recommended to explore these differences in more diverse populations.
Introduction and background
Telemedicine has experienced rapid growth in recent years, particularly in response to the COVID-19 pandemic.1–3 This growth highlights the importance of telemedicine in modern healthcare and its potential to transform patient care delivery in diverse cultural contexts. The adoption of telemedicine offers numerous benefits, including increased access to healthcare services, convenience, and potential cost savings. However, ensuring the quality of patient care remains a critical concern, particularly regarding the quality of patient–physician interactions, which are crucial for healthcare outcomes and patient satisfaction.4,5
Patient–physician interactions play a fundamental role in the delivery of healthcare services, influencing patient satisfaction, adherence to medical advice, and overall health outcomes.6,7 Evaluating these interactions in both telemedicine and in-person settings is essential to ensure that the shift toward telemedicine does not compromise the quality of care. Previous research has demonstrated that positive patient–physician interactions are associated with better adherence to medical advice, higher satisfaction, and improved health outcomes. 7
Technological advancements have significantly reduced barriers to telehealth, making it more accessible, reliable, and user-friendly. 8 These advancements suggest that technology is less likely to be a barrier to effective telehealth delivery, allowing healthcare providers to concentrate more on the quality of interactions and patient care. Utilizing these technological innovations, the Saudi Virtual Hospital (known as SEHA Virtual Hospital) showcases the successful incorporation of contemporary telehealth solutions into a national healthcare strategy. Launched in February 2022 under Saudi Vision 2030, SEHA integrates over 130 hospitals and offers 34 subspecialties, providing telehealth services such as emergency consultations, virtual clinics, and home care. Patients can access these services via their phones for consultations with government Ministry of Health (MOH) hospitals at no cost. During the COVID-19 pandemic, SEHA ensured uninterrupted medical care by providing virtual access to patients. 9
However, there is limited research comparing patient–physician interactions in telemedicine and traditional in-person visits, particularly in the context of Middle Eastern nations. 10 The adoption and implementation of telemedicine in these countries face numerous challenges, such as cultural barriers and issues related to communication and empathy. 10 Studies have shown that cultural and social barriers, including resistance to change and traditional beliefs, significantly impact the acceptance and utilization of telemedicine in some countries in the Middle East and surrounding countries. 10
To assess the quality of patient–physician interactions, it is crucial to employ robust and validated measures. The CARE (Consultation and Relational Empathy) measure is particularly well-suited for this purpose, as it focuses on the empathetic and relational aspects of clinical consultations. 11 The CARE measure evaluates various aspects of patient interaction, focusing on creating a comfortable environment for patients, actively listening and showing genuine interest in their overall well-being, understanding and addressing their concerns with empathy, empowering patients, and collaboratively developing a plan of action. 11
Very few studies have applied the CARE measure specifically in the context of telehealth. For example, Cheshire et al. (2021) utilized the CARE measure to assess physician empathy specifically in the context of telehealth, focusing on stroke telemedicine. 12 They found that there was no significant difference in how patients perceived physician empathy during acute stroke treatment when comparing telemedicine to in-person consultations. 12 This indicates that telemedicine can effectively convey empathy through voice, facial expressions, and attentiveness, even without physical touch or closeness.
Some research has also shown that gender differences exist in healthcare experiences and communications. 13 Male and female patients may have different preferences and expectations regarding patient–physician interactions. 13 Understanding these differences is essential for providing personalized care and ensuring that telemedicine services meet the needs of all patients.
Despite the growing body of research on telemedicine, there are significant gaps in understanding how telemedicine affects patient–physician interactions compared to in-person visits. Addressing these gaps is crucial for optimizing telemedicine practices and ensuring high-quality care for all patients. Understanding the differences in patient–physician interaction ratings between telemedicine and in-person visits, and exploring gender-specific experiences, will help in the design, development, and delivery of telehealth services. Such insights can guide the communication strategies and enhance empathy and understanding in virtual settings, as well as specialized training for healthcare providers to address patients’ needs. Furthermore, these findings can contribute to the development of guidelines that ensure high-quality patient–physician interactions in telemedicine, ultimately enhancing patient satisfaction and health outcomes.
The primary objective of this study is to determine whether there are statistical differences in patient–physician interaction ratings between telemedicine and in-person visits across the 10 items of the CARE measure. A secondary objective is to explore whether significant differences exist in the ratings of patient–physician interactions between male and female patients when comparing telemedicine to in-person visits across these 10 CARE measure items.
Methods
We conducted a quantitative study to assess patient–physician communication during telehealth and in-person visits. Ethical approval was obtained from the Ethics Approval Committee at Jazan University (approval number REC-45/07/962). Data were collected via an online self-administered survey. The survey instrument used in our study was the Arabic version of the CARE Measure, for which we obtained the necessary permission. This validated 10-item tool, utilizing a 5-point Likert scale from “poor” to “excellent,” assesses patient–physician communication and empathy during sessions.11,14,15 The CARE Measure has been extensively tested and shown to reliably capture key aspects of patient experience and relational empathy in healthcare settings. Demographic variables, including age, marital status, and education level, were collected and categorized as detailed in (Appendix 1).
Participants were primarily recruited from a university setting. This recruitment strategy was chosen to ensure participants had the adequate proficiency with technology, allowing us to focus on measuring empathy in telehealth communication without the results being influenced by technological barriers. Participants were included if they had visited a physician, either via telemedicine or in person, within the past year. Exclusion criteria involved individuals without recent healthcare visits, as well as participants who did not provide informed consent or failed to complete the survey. Recruitment took place between December 2023 and March 2024. Participants were provided with an informed consent, and detailed information about the study design along with the survey. Participation was voluntary, and participants had the option to withdraw or skip questions at any time. Data were collected using convenience sampling.
Participants were categorized into two groups based on recent healthcare visits in the past year. Those who have used telemedicine were assigned to the telemedicine group, and were asked about their telehealth experience, while those who visited their physician in-person were asked about their most recent in-person visit. The CARE measure was tailored to reflect the type of visit they had experienced, ensuring relevance to either telehealth or in-person interactions.
The survey was distributed online via the Research Electronic Data Capture (REDCap), which is designed for secure data collection and complies with research requirements. 16 REDCap is a secure, web-based application for building and managing online surveys and databases. 16
The sample size for our study was determined using G*Power 3.1.9.7. 17 To detect a medium effect size (d = 0.5) with a significance level (α) of 0.05 and a power (1 - β) of 0.80, the required sample size was 134 participants, with 67 participants per group. This calculation was based on the Wilcoxon–Mann–Whitney test for two independent groups, assuming a two-tailed test.
Data analysis was performed using SPSS software v23. 18 Descriptive statistics, including means and percentages, were calculated to summarize the data. The Mann–Whitney test was conducted to compare the significance of differences between groups, with p-values indicating statistical significance. The primary outcome measures were derived from the CARE measure, which evaluated patient experiences with communication during telemedicine or in-person visits. Participants were categorized based on their prior use of telemedicine, and experiences were compared between male and female participants.
Results
In this study, demographic data were collected from 392 participants, with a total of 320 providing valid responses about their telehealth or in-person visit. Of these, 120 (37.5%) used telehealth, 200 (62.5%) attended in-person visits, and the remaining participants either were unsure or did not remember (Table 1). Out of the 320 participants, gender distribution was 38.1% male and 61.6% female, with 0.3% opting not to disclose. Marital status data showed that a majority (79.7%) were single, while 17.2% were married, and 2.5% were divorced. The age distribution of participants indicated that the majority (79.4%) were between 18 and 24 years old. The remaining participants were distributed as follows: 10% were aged 25–34, 4.4% were in the 35–44 age range, 4.4% were in the 45–54 age range, and 1.9% were 55 years or older. In terms of education, 74.4% held a Bachelor's degree, followed by 20.9% with a high school or lower, and the remainder with an Associate's, Master's, or PhD degrees.
Participant demographics, marital status, age distribution, education levels, and telehealth usage.

The CARE measure assessed various aspects of patient–physician interaction for telemedicine and in-person visit groups. For the telemedicine group, the mean scores ranged from 3.89 to 4.21, indicating generally positive experiences across all items. For in-person visit group, the mean scores was lower ranging from 3.71 to 3.98 (Table 2) (Figure 1).

Comparison of telemedicine with in-person visits. Mean scores for telemedicine and in-person visits across 10 patient experience items.
Participants rating for each item of the care measure.

*The p-values in this table were calculated using the Mann–Whitney U test, a non-parametric test for comparing two independent groups.
Overall, the telemedicine group rated their experiences slightly more positively across all items compared to the in-person visits group (Table 2). Our results show that Item 3 “Really listening” showed a statistically significant difference, with the telemedicine group rating it higher (Mean = 4.15, Median = 5, IQR = 2) than the in-person group (Mean = 3.87, Median = 4, IQR = 2), as indicated by the Mann–Whitney test (p = 0.049). This suggests that telemedicine group felt more listened to by their physicians. Although other items did not show statistically significant differences, they were consistently rated slightly higher by telemedicine group (Table 2). For example, Item 1, “Making you feel at ease,” and Item 2, “Letting you tell your story,” received higher ratings from Telemedicine users, with only Item 3, “Really listening,” showing a statistically significant difference.
The analysis of gender differences revealed clear patterns in patient–physician interactions when comparing telemedicine to in-person visits for each gender separately. Among female participants, there were no significant differences in ratings between those who used telemedicine and those who had in-person visits (Table 3). A total of 197 females participated in the study. Of these, 71 (36.0%) reported using telehealth, while 126 (64.0%) reported attending in-person visits. The mean scores for females in the telemedicine group ranged from (Mean = 3.76, Median = 4, IQR = 2) to (Mean = 4.12, Median = 5, IQR = 2), while for those in the in-person group, scores ranged from (Mean = 3.83, Median = 4, IQR = 2) to (Mean = 4.07, Median = 5, IQR = 2). All p-values exceeded the significance threshold, indicating that the mode of interaction did not significantly affect their experience.
Comparison of CARE measures items for female participants who used and did not use telemedicine.
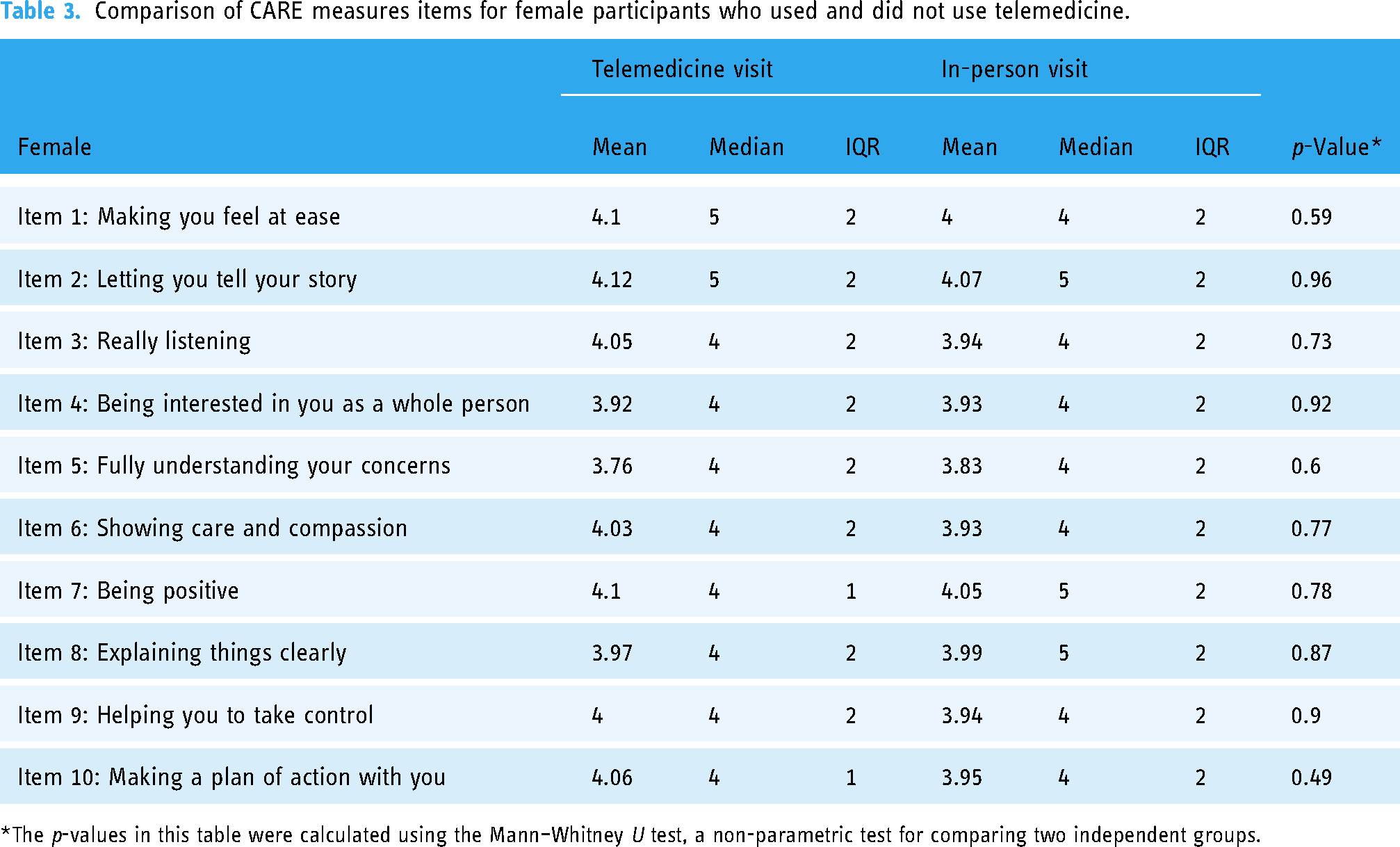
*The p-values in this table were calculated using the Mann–Whitney U test, a non-parametric test for comparing two independent groups.
A total of 122 males participated in the study of these, 48 (39.3%) reported using telehealth, while 74 (60.7%) reported attending in-person visits. Given the underpowered statistical tests for the male group, these findings should be interpreted with caution. Among male participants, those who used telemedicine reported significantly different experiences (Table 4). For items such as Item 2 “Letting you tell your story,” Item 3 “Really listening,” Item 4 “Being interested in you as a whole person,” Item 5 “Fully understanding your concerns,” Item 6 “Showing care and compassion,” Item 7 “Being positive,” and Item 8 “Explaining things clearly,” males in the telemedicine group reported significantly higher ratings compared to in-person visits group. For instance, the mean score for Item 2 “Letting you tell your story” was (Mean = 4.43, Median = 5, IQR = 1) for males in the telemedicine group, compared to (Mean = 3.82, Median = 4, IQR = 2) for in-person visits group, with a p-value of 0.00. Similarly, for Item 3 “Really listening,” the mean scores were (Mean = 4.37, Median = 5, IQR = 1) for telemedicine group and (Mean = 3.73, Median = 4, IQR = 2) for in-person visits group, also with a p-value of 0.00. These findings suggest that telemedicine may significantly enhance the patient–physician interaction experience for male participants across several key dimensions of care. These findings suggest that telemedicine may significantly enhance the patient–physician interaction experience for male participants across several key dimensions of care. However, the sample size for males using telehealth (n = 48) falls short of the required 67 participants to achieve adequate power for detecting a medium effect size (d = 0.5) with 80% power. Therefore, the results for the male telehealth subgroup may be underpowered and should be interpreted with caution.
Comparison of CARE measures items for male participants who used and did not use telemedicine.

*The p-values in this table were calculated using the Mann–Whitney U test, a non-parametric test for comparing two independent groups.
Discussion
This study aimed to evaluate patient communication and empathy with telehealth compared to in-person visits, focusing on the quality of patient–physician interactions. Telemedicine users rated their experiences more positively across all items compared to non-users. Of the 10 CARE measures items compared, the item “Really listening” showed a statistically significant difference, with telemedicine users feeling more heard by their physicians.
Prior work that compared telehealth with in person visits using different tools reported mixed experienced. A study using Press Ganey scores to compare the telehealth and in-person patient encounters found no significant difference in the odds of respondents giving a top box score to rate their satisfaction with their care provider between telehealth and in-person encounters.19,20 Consistent with our finding, studies that employed questionnaires that investigate the details of the visits, communication, and patient experience reported higher rating for telehealth.21,22 Conversely, Itamura et al. reported lower satisfaction scores for telehealth compared to in-person visits, particularly in areas of provider listening, conveyance of information, and overall provider ratings. 23 Itamura et al. also noted technical issues such as video quality and wait times, which could have contributed to the lower satisfaction scores for virtual visits during the early pandemic period.
A study by Cheshire et al. employed the CARE measure to evaluate patient perceptions of physician empathy in stroke telemedicine. 12 The study enrolled 71 patients and found no significant difference in empathy scores between telemedicine and in-person consultations, with high satisfaction levels reported for telemedicine. It is worth noting that our study population was considerably younger than those in previous studies. Despite these demographic differences, similar results were observed. 12
The finding of our study suggests that telemedicine can enhance certain aspects of patient–physician interactions, particularly for younger, tech-savvy populations. Most of our participants were young (aged 18–24) and likely familiar with technology, which may have contributed to their positive experiences with telemedicine. Additionally, the study was conducted recently, during a period when telehealth had gained more acceptance and integration into healthcare systems following the COVID-19 pandemic. This broader acceptance and familiarity with telehealth may have positively influenced patient perceptions and satisfaction.
Our study has few limitations that should be considered. Our sample predominantly comprised young, single individuals, which may limit the generalizability of the findings to older populations. The studies also relied on self-reported measures, which can be subject to recall and response biases. Additionally, our study did not investigate the reason for the visit or the clinic specialty visited, which could influence participants’ perceptions of empathy. Different medical conditions or reasons for consultations may lead to varying expectations and experiences in patient–physician interactions. For example, patients seeking care for chronic conditions might place a higher value on long-term relationship-building and empathetic communication, whereas those with acute or urgent concerns may prioritize efficiency and clear instructions. Similarly, the nature of the clinic or specialty, such as mental health versus primary care, could also affect how empathy is perceived. Without accounting for these factors, our results may not fully capture the variability in empathy experiences across different healthcare contexts. Future research should consider including visit reasons and clinic specialties for deeper understanding of the perceived patients’ empathy.
For future research, we recommend including a wider demographic to ensure findings are applicable to diverse patient populations. We also recommend the consistency in using standardized tools such as the CARE measures across different specialties to allow for better comparison and optimization of the areas of the CARE measure. The current use of varying measures in studies limits the comparability and reliability of meta-analysis reviews. Moreover, investigating the reasons behind gender-specific differences in telehealth experiences can provide deeper insights into optimizing telehealth for different patient groups. Additionally, research must consider cultural contexts and the variability in telehealth adoption across different regions and populations to provide a comprehensive understanding of telehealth's effectiveness and areas for improvement.
Conclusion
In conclusion, our study demonstrates that telehealth can provide quality patient–physician interactions, with significant positive perceptions among younger, tech-savvy users. These findings highlight the potential of telehealth to meet patient needs effectively, especially when technological and communication challenges are addressed. Continued efforts to enhance virtual communication and patient engagement are essential to maximize the effectiveness and satisfaction of telehealth in the long term.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076241305284 - Supplemental material for A comparative study of patient–physician empathy in telehealth and traditional in-person visits
Supplemental material, sj-docx-1-dhj-10.1177_20552076241305284 for A comparative study of patient–physician empathy in telehealth and traditional in-person visits by Abdulrahman M Jabour in DIGITAL HEALTH
Footnotes
Acknowledgements
The author would like to thank all participants who participated in this survey. The author also gratefully acknowledges the funding of the Deanship of Graduate Studies and Scientific Research, Jazan University, Saudi Arabia, through Project Number: GSSRD-24.
Contributorship
The primary author AMJ has designed, conceptualized and conducted the study, including the analysis and writing.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The Research Ethics Review Committee at Jazan University approved the study (Approval: REC-45/07/962). Participants received written information detailing the study, including the consent information and the questionnaire, during the invitation. This information was designed to be clear and concise, explaining the study's purpose, the questionnaire design, and the intended use of the collected data.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Guarantor
Abdulrahman Jabour, PhD.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.