
Abstract
Introduction:
The COVID-19 pandemic has disproportionally affected historically marginalized populations and their access to resources and healthcare. In times of crisis, authentic community engagement is more important than ever. This study was Phase 1 of a larger 3-phase study to conduct timely community-engaged research with community members to understand the disproportionate impact of COVID-19 on historically underserved communities. The objective of this work was to conduct key informant (KI) interviews (1) to understand community organizations perspectives about the role that large academic health centers play as they interface with community organizations to support their work, (2) to leverage KI’s expertise to identify needs and assets within the community, and (3) to inform both Phase 2 (focus group qualitative research) and Phase 3 (survey) of the broader study.
Methods:
A total of 24 key informants were identified through purposeful sampling and one-on-one semi-structured interviews were conducted across 4 states using video conferencing.
Results:
Barriers to access and lack of transparency were highlighted as major issues requiring reform—in particular, aggressive billing practices and insurance barriers exacerbated local distrust of medical institutions. KIs recognized the health institution’s support for testing and vaccination during the COVID-19 pandemic, but noted other significant gaps in care, especially regarding mental health support. Although communication with the health institution was consistent for some KIs, others experienced unsustained communication efforts that hindered cooperation and relationship building.
Conclusions:
Leaders in the community as key stakeholders can provide unique insights into the challenges and potential solutions required to promote health equity, and foster understanding between local communities and healthcare institutions.
Introduction
The COVID-19 pandemic has disproportionally affected historically marginalized populations and their access to healthcare and other resources. Black and Hispanic communities experience higher rates of coronavirus infections, hospitalizations, and mortality compared to White communities.1,2 These findings highlight the need for healthcare reform and attention to health disparities.3,4
In many of these communities, medical anchor institutions have begun taking initiatives to address the needs of under-resourced populations. 5 These institutions serve a vital role in communities, mobilizing economic resources to support local community-based organizations and to promote health.6-8 There is increasing emphasis on the role of large academic health systems in supporting local communities and as potential “anchor institutions.”5-8
Community engaged research (CEnR) is defined by the Centers for Disease Control and Prevention as “the process of working collaboratively with and through groups of people affiliated by geographic proximity, special interest, or similar situations to address issues affecting the wellbeing of those people.” 9 By understanding stakeholder and community needs, CEnR approaches can influence public health initiatives and address health disparities.7,8,10,11
In times of crisis such as the global COVID-19 pandemic, authentic community engagement is more important than ever to build trust in healthcare and public health organizations and highlight issues of food insecurity, education, and economic opportunities.7,8,10,11 Community engagement aids researchers in formulating culturally sensitive interventions to support the needs of underserved populations. 12 This approach helps community organizations improve the effectiveness of their programs, which can in turn improve their ability to empower community interests. 13
Consulting key informants (KIs), community experts that hold formal positions and have special or relevant knowledge, is crucial to formulating a comprehensive view of a community’s health needs. 14 Conducting KI interviews helps glean insight into the intricate networks of these communities, including the experiences and needs of people from disenfranchised and underserved groups. 15
This study was part of a larger 3-phase research program developed to conduct timely community-engaged research with community members in order to understand the disproportionate impact of COVID-19 on historically underserved communities. The objective of this phase of the study was to conduct KI interviews (1) to understand community organizations’ perspectives about the role that large academic health centers can play as they interface with community organizations to support their work, (2) to leverage KI’s expertise to identify needs and assets within the community, and (3) to inform Phase 2 (focus group) and Phase 3 (survey) of the research program.
Methods
Study Setting and Design
The Phase 1 of our work described in detail in this paper was part of a mixed methods study. In Phase 1, we used purposive sampling to identify key informants from multiple stakeholder groups and conducted semi-structured interviews. In Phase 2, we held focus groups with community members from historically marginalized demographics. In Phase 3, we developed a survey using validated scales and distributed it to diverse communities residing in the geographic areas of our healthcare system across 4 states. Phase 1 of the study were approved as minimal risk by the Mayo Clinic IRB (21-001802). We conducted Phase 1 between March and July of 2021 across the Mayo Clinic Health System (MCHS) which includes the catchment areas of the 3 academic medical centers and the health system. Mayo Clinic is a health care organization with a wide geographic reach, with hospitals in Scottsdale, Arizona; Jacksonville, Florida; Rochester, Minnesota; and a Health System spread throughout Minnesota and Wisconsin.
Phase 1: Key Informant (KI) Interviews
Participants and recruitment
Our study team used purposive sampling to identify key informants (KI) from multiple community stakeholder groups that included county public health officials, safety net medical providers, community leaders, non-profit organization executives and staff, and health system leadership. We connected with stakeholders via email or phone to outline the nature of the study and participation requirements. All consent forms were automatically emailed to those who agreed to participate and completed via DocuSign (DocuSign, San Francisco, CA) prior to the interview.
The broader study team developed the interview guide which contained questions that explored the mission of the organization within which the KI was working, communities the organization served, health challenges facing those communities, current efforts to address the needs and assets, and research needed to amplify current work (Appendix 1). Other included questions asked about the specific effect of COVID-19 in those communities, how services were modified to meet needs, and suggestions for efforts and research to support and prepare communities for future similar events, as well as the organization’s relationship with MCHS and current collaborative initiatives.
Data collection
We scheduled online video conferencing interviews for up to 60 min. Study team members (AB, KC) conducted one-on-one, semi-structured interviews. We did not offer remuneration.
Qualitative Analysis
We recorded all KI interviews, and the audio recordings were transcribed verbatim and de-identified prior to analysis. Interview data were organized and analyzed using the Framework analytic approach. 16 Trained coders (AB, KC, TC) collaborated on each phase of analysis, from indexing to exemplar (quote) retrieval; (KC, LH, AB). Coding was guided deductively by the interview guide and left open to inductive findings as they arose during the coding process.
Results
KI Interviews
We conducted 24 KI interviews. Demographic, geographic, and organizational sector characteristics are outlined in Table 1.
Demographics.

MCHS’s COVID-19 pandemic response was met with both negative and positive feedback. Common themes are provided in Table 2.
Themes.
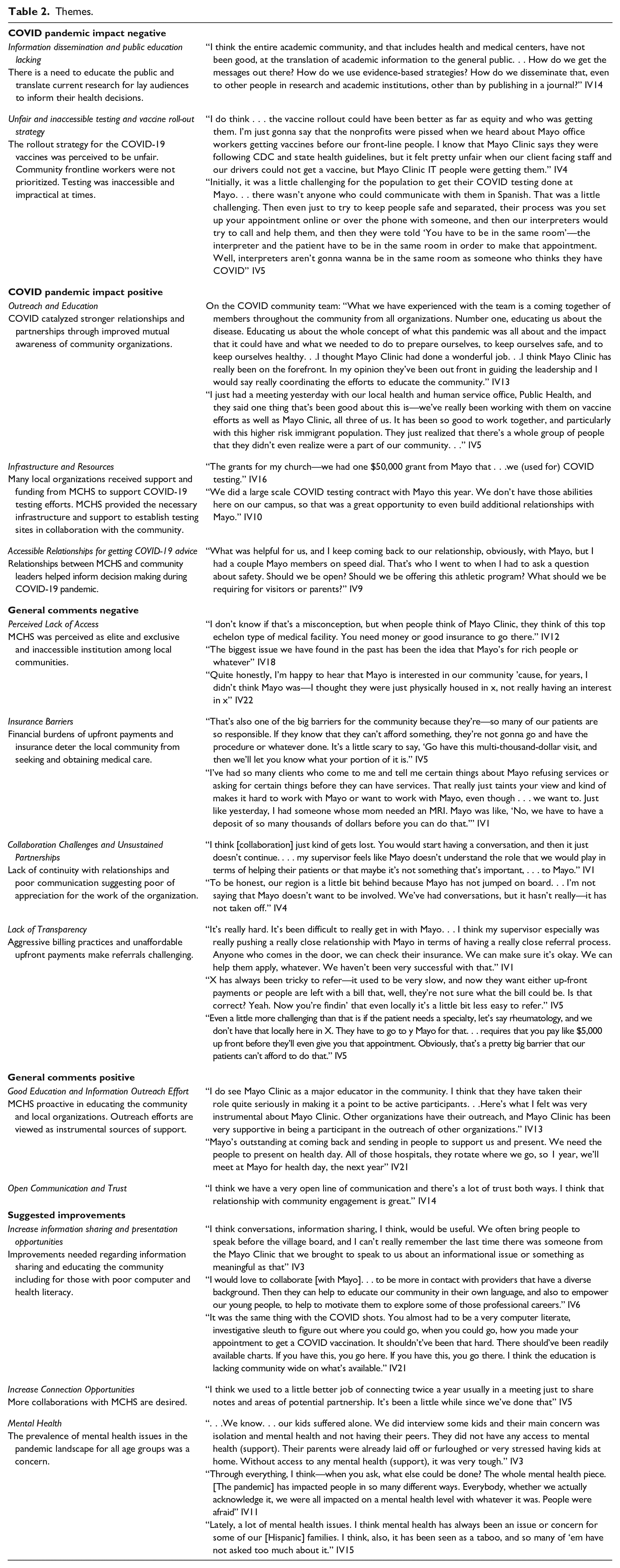
Negative Perceptions of MCHS Pandemic Response
Information dissemination and lack of public education
Under-resourced communities struggled to stay informed about COVID-19 prevention methods. KIs wished that COVID-19 research was better communicated to the public. They emphasized relaying published scientific findings to lay audiences to promote public education.
Unfair and inaccessible testing and vaccine roll-out strategy
Some KIs noted unfair vaccine rollout decisions by MCHS. They felt that rollout priorities were inequitable and frontline non-profit community organization workers were neglected in this process.
Positive Perceptions of MCHS Pandemic Response
Outreach and education
Other KIs found MCHS’s presence to be a “unifying force” and “community focused,” addressing the community’s needs and providing education in times of uncertainty.
Funding and infrastructure
Many also reported that MCHS was instrumental in supporting and setting up testing and vaccination efforts in local underserved areas. MCHS provided infrastructure and funding necessary to establish COVID-19 related resources for prevention of infection.
Accessible relationships for getting COVID-19 advice
Many KIs felt that they had a strong, accessible relationship with MCHS throughout the pandemic and in some cases the collaborative work conducted during the pandemic had strengthened ties with MCHS and increased awareness of available resources and organizations. Some KIs cited the ability to directly reach MCHS experts as essential during decision making about safe programming in their organizations.
Overall Negative Perceptions of MCHS
Perceived lack of access
Key informants emphasized community distrust and intimidation about seeking care at MCHS. Organizations as well as individuals were skeptical of collaborating or receiving care at MCHS due to the perception that MCHS was too exclusive. KIs illustrate that many community members “have an image of Mayo that it’s just not for everybody.”
Insurance barriers
Underserved communities did not perceive MCHS as a viable resource due to financial barriers and insurance.
Collaboration challenges
KIs reported difficulties navigating and sustaining communication and relationships with MCHS. Many KIs believed that MCHS as an institution demonstrated a lack of willingness to meaningfully work with local organizations and this could only be achieved with individuals working beyond the scope of their role.
Lack of transparency
KIs, especially those from safety net sites, discussed the challenges their patients faced when being referred. There is a perceived lack of transparency around billing and referrals for those who need specialized care. These financial barriers to pursing care at MCHS deterred underserved communities from prioritizing their health.
Overall Positive Perceptions of MCHS
Good education and information outreach efforts
In local underserved communities, KIs identified MCHS as a major educational resource and support structure. They illustrated how MCHS plays an active role in the community by bringing speakers to present on various health topics.
Open communication
KIs emphasize that partnerships with MCHS involve bidirectional open communication and trust.
Suggested Improvements
Increase information sharing and education opportunities
Multiple KIs suggested improvements in education of both the community and youth.
Increase connection opportunities
KIs want to increase regular connection opportunities and collaboration efforts with MCHS.
Mental health
Many informants also expressed that access to mental health resources is neglected in underserved populations.
Discussion
This paper describes KI interviews which were conducted as part of a 3-phase mixed methods study assessing the impact of COVID-19 on community health and wellbeing. KIs are local experts and community leaders that play a vital role in addressing the needs of their constituents.14,15 They are uniquely positioned to understand local challenges, evaluate how anchor institutions interface at the organizational level, and assess the impact of anchor institutional activities on local health outcomes.14,15 As such, KI feedback provides a robust basis for specific, tailored improvements to MCHS’s impact in underserved communities that strengthen MCHS’s function as an anchor institution.
KIs praised MCHS’s role in educating the community, recommending that MCHS offer additional educational opportunities and deepen information sharing with local communities. KIs also recognized MCHS’s support for testing and vaccination, but noted significant gaps in care, especially regarding mental health. KIs highlighted barriers to access and lack of transparency as major issues requiring reform—in particular, aggressive billing practices and insurance barriers exacerbated local distrust of medical institutions. KIs also identified challenges they faced in collaborating with MCHS—while some enjoyed consistent communication, others experienced poor communication that hindered consistent and ongoing cooperative efforts.
Our study builds on the small but growing literature on the role large medical institutions play in serving local communities during the COVID-19 syndemic—a disastrous confluence of deadly disease, systematic racism, adverse political-economic forces, and institutional violence. 17 We affirm and extend the findings of Leese et al 18 that sustained relationship building, hearing diverse perspectives, and understanding change and uncertainty are crucial to developing a stronger pandemic response. In particular, it is imperative that MCHS and other large health care organizations pursue deeper relationships with local communities to foster trust in medical interventions.10,19 They should also deepen their understanding of social determinants of health (SDOH), pre-existing health conditions, and access to care in underserved communities, as these factors lead to worse health outcomes and higher susceptibility to COVID-19 and other diseases.20,21 MCHS and other organizations can draw inspiration from the 5-part action plan proposed by Maulik Joshi, of Meritus Health, which aims to combat health inequity and racism by addressing unconscious biases, disparities in care, lack of racial and ethnic diversity in leadership, and adverse SDOH.21,22
Strengths of this study include diverse perspectives from local leaders from organizations within the MCHS community and catchment areas. The insights garnered from KI expertise allow us to implement changes specific to the needs of the community and strengthen MCHS role as an anchor institution.23,24 The KI interviews informed the phase 2 and 3 of our study. Our findings will be triangulated by other work in our mixed methods study.
Limitations of the study include the following. While our methodological approach can be replicated in other healthcare systems that wish to conduct robust community engaged research, the positive and negative impressions cited by our KIs may not be the same challenges that community organizations working with other large healthcare systems experience. However, despite issues of generalizability we expect there are likely shared concerns. Furthermore, we acknowledge that some KIs would have had important insights, but due to scheduling difficulties exacerbated by the pandemic, we were unable to interview them.
Overall, our findings highlight the need for large academic health centers to act as anchor institutions, especially in turbulent times where COVID-19 has exacerbated vulnerabilities among underserved groups by amplifying problems such as financial instability and lack of access to healthcare.12,18,25 Our findings serve as a guide for other large academic centers, informing their outreach efforts and community engagement programs. Based on our findings, future directions include and providing care through additional community engagement and outreach efforts. Further investigation in information dissemination regarding emerging health topics and available health services is needed.
Conclusion
Leaders in the community as key stakeholders can foster understanding and provide insights to inform large academic health centers about approaches to address health and healthcare inequities in the community. Our results highlight the need for community engagement research and the importance of medical anchor institutions in underserved communities during times of crisis. Facilitating partnerships and the exchange of accessible information will help foster trust in the healthcare system.
Footnotes
Appendix 1. Interview Guide
Thank you for joining us. Before we begin can you confirm that you had a chance to review the consent form we sent over and that you are willing to proceed with the interview?
Thank you. With your permission, I will be audio recording our conversation to ensure accuracy. Do I have your permission to turn on the recorder?
Thank you. To start, can you state your role and what you do on a day to day basis?
How would you frame the mission of [organization]?
What communities does [organization] seek to serve?
What are the greatest health challenges facing those communities?
What efforts are currently underway to address those challenges?
What additional resources or assets would amplify those efforts?
What research would help with moving those efforts forward?
Does your organization have any relationship with Mayo Clinic?
Can you tell me why or why not and what you think would facilitate stronger relationships?
I’m going to talk a little about the current COVID pandemic now and how it has affected your community.
How has COVID impacted your organization and the communities it serves?
In addressing the impact of COVID has your organization shifted to any remote services such as phone visits or socially distanced deliveries?
Has your organization received any local, state, or Federal support to help with those impacts?
If yes, in what form and how effective was it?
If no, did you apply for or seek any such assistance and why did you not receive it?
How do you think we could better support communities during mass health events such as COVID?
What do you think needs to be done to better prepare our communities for future events?
In the wake of COVID, what research do you think would be helpful in understanding how better to combat these events?
Mayo Clinic is launching a new initiative to drive research in addressing community health needs and disparities. Is that something you think you and/or your organization would be interested in joining?
Acknowledgements
We would like to thank the Mayo Clinic Center for Health Equity and Community Engaged Research (CHCR) which provided funding for this initiative.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.