
Abstract
Maintaining therapeutic levels of anticoagulation is essential to avoid health complications in people who take vitamin K antagonists. This study aimed to analyze the influence of people’s characteristics and the presence of changes in their lives in the control of therapeutic levels of anticoagulation. A longitudinal multicenter study with a 1-year follow-up of a cohort of 199 people receiving anticoagulant therapy was performed. The effect of biological, clinical, social, lifestyle, and changes in life on the international normalized ratio (INR) was analyzed. During the follow-up, 46.7% of participants presented good INR control. At baseline, a diagnosis of atrial fibrillation (P = .00), the lack of comorbidities (P = .03), absence of depression (P = .04), and not following a pharmacological treatment with hypoglycemia drugs (P = .01) were associated with good INR control. During the follow-up, the variable of making changes to the usual diet was associated with poor INR control (P = .05). In the binary multiple regression model, factors associated with poor control were taking hypoglycemia drugs (P = .02) and the presence of depression (P = .04), and only the diagnosis of atrial fibrillation was associated with good control (P = .03). People with a diagnosis of atrial fibrillation had good INR control. Having comorbidities, suffering depression, taking hypoglycemia drugs, and making changes to the diet have a negative effect on INR control.
Keywords
Background
Cardiovascular diseases are one of the main causes of death worldwide and 23.6 million such deaths are forecast in 2030. 1 Atrial fibrillation is the most common sustained cardiovascular disease in adults worldwide with a prevalence between 2% and 4%. 2 A 2.3-fold rise is expected owing to extended longevity and intensified searching for undiagnosed atrial fibrillation.3,4
Atrial fibrillation is associated with a five-fold increase in the risk of stroke, given that between 20% and 30% of people with ischemic stroke are diagnosed with this disease before, during or after the event. Therefore, atrial fibrillation poses a significant burden to patients, physicians, and healthcare systems globally. 5
Both preventative and curative treatment of these diseases is through anticoagulation. The decision to anticoagulate patients with atrial fibrillation depends on the stroke risk. 6 In general, oral anticoagulation is indicated in the prevention of cardiac thromboembolism with a CHA2DS2-VASc score ≤2. There are 2 main types of oral anticoagulant therapies: vitamin K antagonists and direct oral anticoagulants. The European Society of Cardiology recommends the use of direct oral anticoagulants instead of vitamin K antagonists when oral coagulation is initiated in patients with atrial fibrillation. 5 However, vitamin K antagonists have shown their efficacy in the prevention of thromboembolic events, especially in older people, 7 and are currently the treatment of choice for atrial fibrillation. 8 The use of these antagonists is conditioned by the narrow therapeutic window, which requires monitoring through the international normalized ratio (INR) and frequent dose adjustments. 9
The general recommendation is to maintain the INR between 2 and 3, although this can vary depending on the reason for the anticoagulant therapy. 9 When INR values are below the recommended range, the risk of stroke is doubled, whereas if INR values are above this range the risk of cerebral hemorrhage increases. 6 Therefore, the maintenance of therapeutic levels of anticoagulation is essential to avoid complications. 10 This treatment is often monitored in primary care settings and professionals from this area are essential both in the diagnosis and in determining the most suitable approach. 11
People on oral anticoagulant therapy often present out-of-range INR values. 12 Age, comorbidities, poor drug adherence, tobacco and alcohol use, changes in prescribed treatments, dietary changes, and the consumption of herb-based supplements have all been associated with poor INR control.5,9,12-14
Knowledge of the characteristics of the population receiving oral anticoagulant treatment and the factors influencing its control provides the basis for establishing care strategies. Although there are studies about treatment with vitamin K antagonists, 15 few are focused on the characteristics we consider in the present study and few published studies report longitudinal controls of this treatment in primary care settings. The present study aimed to analyze the control of therapeutic levels of anticoagulation and to relate this control to people’s characteristics and the presence of changes in their lives during the study period.
Methods
Design
A multicenter prospective cohort study with a 1-year follow-up of patients receiving anticoagulant therapy.
Sample
The study population consisted of people treated with vitamin K antagonists and who had INR controls in 1 of the 4 participating primary health care centers located in the Girona Health Region (n = 274). Exclusion criteria were having initiated the treatment less than 6 months earlier, being institutionalized or included in the home care program, and being unable to respond to the questionnaires for cognitive reasons.
Instruments
Two ad hoc questionnaires were prepared, one for the first visit and one for successive visits. The first questionnaire consisted of 4 sections: (a) sociodemographic data: age, sex, cohabitation status, educational level, occupation, and primary care center; (b) clinical data: diagnosis, obesity, comorbidities (Charlson Comorbidity Index 16 ), cognitive state (Pfeiffer Short Portable Mental Status Questionnaire 17 ), depression (The Geriatric Depression Scale 18 ), and pharmacological treatment; (c) lifestyle: physical activity and addictions: (tobacco and alcohol) and (d) data related to the treatment with vitamin K antagonists: initiation, preparation of the drug, discomfort with the INR control, discomfort with the vitamin K antagonist therapy, controls with the primary care nurse, and attendance at therapy groups. In the second questionnaire, data was gathered during the INR controls about the following changes and events: pharmacological treatment, changes in diet, intercurrent health problems (such as, eg, viral processes or surgical interventions), and failures to take the dose of the anticoagulation drug. INR control was considered to be good in those patients who had at least 60% of INR controls within the range during the year of follow-up (in accordance with the individually established INR ranges based on the pathology).
In order to increase the validity of the results, both clinical experts (2 experienced case management nurses in cardiac pathology and 1 in hematology) and methodological experts participated in the preparation of the questionnaires. These were administered during the consultation visits with the different primary care nurses who had received specific training for the study.
Before the start of the study, a pilot questionnaire was given to 15 people who were being treated with vitamin K antagonists and who were under INR control at one of the participating primary health care centers, which resulted in minor modifications being made.
Data Collection
Patients were recruited through the primary care nurses. Once included in the study, the baseline visit was set at which the data from the first questionnaire was gathered. Afterward, and over a period of 12 months, a nurse administered the second questionnaire at each of the monthly INR control visits.
Before starting the full study, a pilot test was conducted with 15 patients. No modifications were required as all participants understood all the questions asked.
Ethical Considerations
The study was carried out in accordance with the Declaration of Helsinki and the European Medicine Agency Guidelines for Good Clinical Practice. The study was approved by the territorial research ethics committee. Informed consent for study participation was required.
Data Analysis
The data obtained from the questionnaires was analyzed using IBM SPSS Statistics for Windows (version 21.0; IBM Corp. Released, 2012).
Continuous variables were described as the mean and measures of dispersion (standard deviation, median, and interquartile range). Categorical variables were described in terms of absolute and relative frequencies. The normality of data distribution was analyzed using the Kolmogorov-Smirnov test. Bivariate analyses using the Chi-square test and the independent samples with the Mann-Whitney U test and a binary logistic regression model were used to study the variables associated with INR levels. The level of significance for all analyses was set at P < .05.
Results
The final sample included 199 patients (72.9% of the people who were taking anticoagulant therapy during the study period). Of these, 56% (n = 112) were men. The average age of the participants was 75.9 (SD: 9.5), median 78 (IQR 70-83) years. 72.9% lived with other people, 27.1% had intermediate studies, and 43.2% did or had done unqualified work.
About 82.4% of the participants took vitamin K antagonists due to a diagnosis of atrial fibrillation. The mean body mass index of the participants was 28.5 (SD: 4.8) (overweight). 13.6% had a comorbidity index of over 4 points, the mean of the Pfeiffer test was 1.46 (SD: 2.4) points (normal cognitive state), and 18.1% of participants suffered cognitive deterioration. 77.4% of the participants did not present depression. Clinical characteristics of the sample, as well as prescribed treatments, apart from the vitamin K antagonist, are presented in Table 1.
Clinical Characteristics of the Sample and Their Relation to INR Control (n 199).

The categorical variables are described with the absolute frequency and their percentage.
Chi-square test P < .05.
The participants did an average of 4.37 (SD: 4.7) hours of physical exercise per week. With regards to addictions, 62.8% of the participants were nonsmokers and 54.8% consumed alcohol with low risk (Table 2).
Variables Related to Lifestyle and AVK Treatment and Their Relation to INR Control (n 199).

The categorical variables are described with absolute frequencies and their percentage.
These results should be considered with caution as the application criteria are not met.
Chi-square test P < .05.
The mean time since the initiation of vitamin K antagonist therapy was 76.6 (SD: 80.2) months, and most prepared the drug for themselves (85.9%). 74.4% of the participants did not refer to any discomfort related to the INR control and 75.9% did not refer to any discomfort with regards to the vitamin K antagonist treatment. 85.4% of the participants followed controls with their primary care nurse for motives unrelated to INR control and 10.6% had participated in therapy groups of people in treatment with vitamin K antagonists (Table 2).
Results Associated With International Normalized Ratio Control
The results of the study show that 46.7% of patients had good INR control and that there were no significant differences based on age (P = .59), sex, whether one lives alone or not, education, occupation, and primary care center.
Good INR control was associated with the following clinical variables: a diagnosis of atrial fibrillation, the lack of comorbidities, absence of depression, and not following a pharmacological treatment with hypoglycemia drugs. Specifically, 51.2% of people with a diagnosis of atrial fibrillation had good INR control (P < .01). Poor INR control was associated with a comorbidity index of more than 4 points (70.4%; P = .03). Furthermore, 66.7% of people with a diagnosis of depression had poor INR control (P = .04) as did 68.8% of the participants who took hypoglycemia drugs (P = .01).
The number of drugs taken by the participants, obesity and cognitive state were not found to be associated with INR control (Table 1).
Physical activity, tobacco, alcohol consumption, the length of treatment with AVK, who prepared the medication, the perception of discomfort associated with the control of the INR or the medication, and following controls with the primary care nurse or participating in peer therapy groups were not found to be associated with control of the INR (Table 2).
In general, people who had intercurrent health problems, especially fever and gastrointestinal problems and those that omitted taking some of the doses of AVK showed worse control of the INR, although this was not a significant association. On the other hand, making changes to the diet that is usually consumed was associated with worse control of the INR (1.07 [1.3] vs 1.64 [1.7]; P < .05).
The logistic regression model shows that taking hypoglycemia drugs (OR = 0.44, 95% CI 0.216-0.912, P = .02) and depression (OR = 0.72, 95% CI 0.522-0.988, P = .04) were strongly associated with poor INR control. Only the diagnosis of atrial fibrillation (OR = 2.55, 95% CI 1.085-6.038, P = .04) was associated with good control (P = .03) (Table 3).
Binary Logistic Regression Model for Variable Associated with INR Control (n 199).

Abbreviations: B, coefficient B; β, standardized beta coefficient; 95% CI, confidence interval of 95%; corrected R2, adjusted R-square (adjusted coefficient of determination); R2, R-square, the coefficient of determination; SE, standard error.
Discussion
This study analyzed the control of therapeutic levels of anticoagulation in relation to people’s characteristics and the presence of changes in their lives over a period of 1 year. The results show that just over half of the participants had good control of the INR and that no differences were found in terms of sex and age. Our findings are partially in line with earlier studies. In this respect, people treated with AVK often present out of range INR values,19,20 especially in women.5,21
Most participants took vitamin K antagonists for a diagnosis of atrial fibrillation given the efficacy of this drug in the prevention of thromboembolic events in these patients. 8
The results of the study associate the presence of comorbidities and depression with a worse control of the INR. Similar results have been found in earlier studies.5,9,14 Furthermore, Cosanu et al 22 have shown the benefit of changing vitamin K antagonists to direct anticoagulants in people with depression. There is also evidence for this same change being made in people with cognitive deterioration. 23 However, the results of the present study do not find an association between cognitive state and INR control.
In studying the interaction of the vitamin K antagonist with other drugs, it was observed that taking hypoglycemia drugs was associated with worse control of the INR. The effect of some drugs on vitamin K treatments has been previously reported5,14 and studies that have analyzed the specific effect of hypoglycemia drugs have suggested opting for a treatment that does not require a periodic adjustment of the dose. 24
The binary multiple regression model revealed that the presence of a diagnosis of atrial fibrillation is associated with good control of the INR of the participants, on the other hand, a high comorbidity index, depression, and taking hypoglycemia drugs is associated with poor control of the INR.
In terms of lifestyle, despite sedentary participants having more INR controls outside of normal ranges, the study does not show a significant relationship between physical activity and INR control. Previous studies have found that patients that perform physical activity present therapeutic INR ranges that are more correct. 14
Addiction to tobacco and alcohol have not been associated with INR control in the present study. In contrast, previous studies have found a negative effect of tobacco and alcohol use with INR control.5,14,15 These differences between our results and those of other studies might be explained by the fact that we had a small sample of people who were smokers and consumed alcohol with lower mean ages and comorbidity indexes.
With regards to the changes that were produced during the phase of follow-up of participants, the results of the study show that people who made changes to their usual diet had worse INR control, as was also found by Violi et al. 25 Other authors have highlighted the effect of various herbs, food, and dietary supplements that are rich in vitamin K on INR control.26-28 Additionally, many patients on warfarin remain unaware of which foods contain large amounts of vitamin K. Practitioners should advise patients to consume a steady amount of vitamin K in their diet and make sure that they are familiar with which foods contain this vitamin. 29
We did not find therapeutic adherence, changes in the habitual treatment and intercurrent health problems to be associated with INR control. However, previous studies have associated low therapeutic adherence, making changes in habitual treatments and the presence of intercurrent problems5,14 with poor therapeutic control of the INR.
Figure 1 shows the relationship of INR control with clinical characteristics, social support, lifestyle, and changes and events affecting the participants.
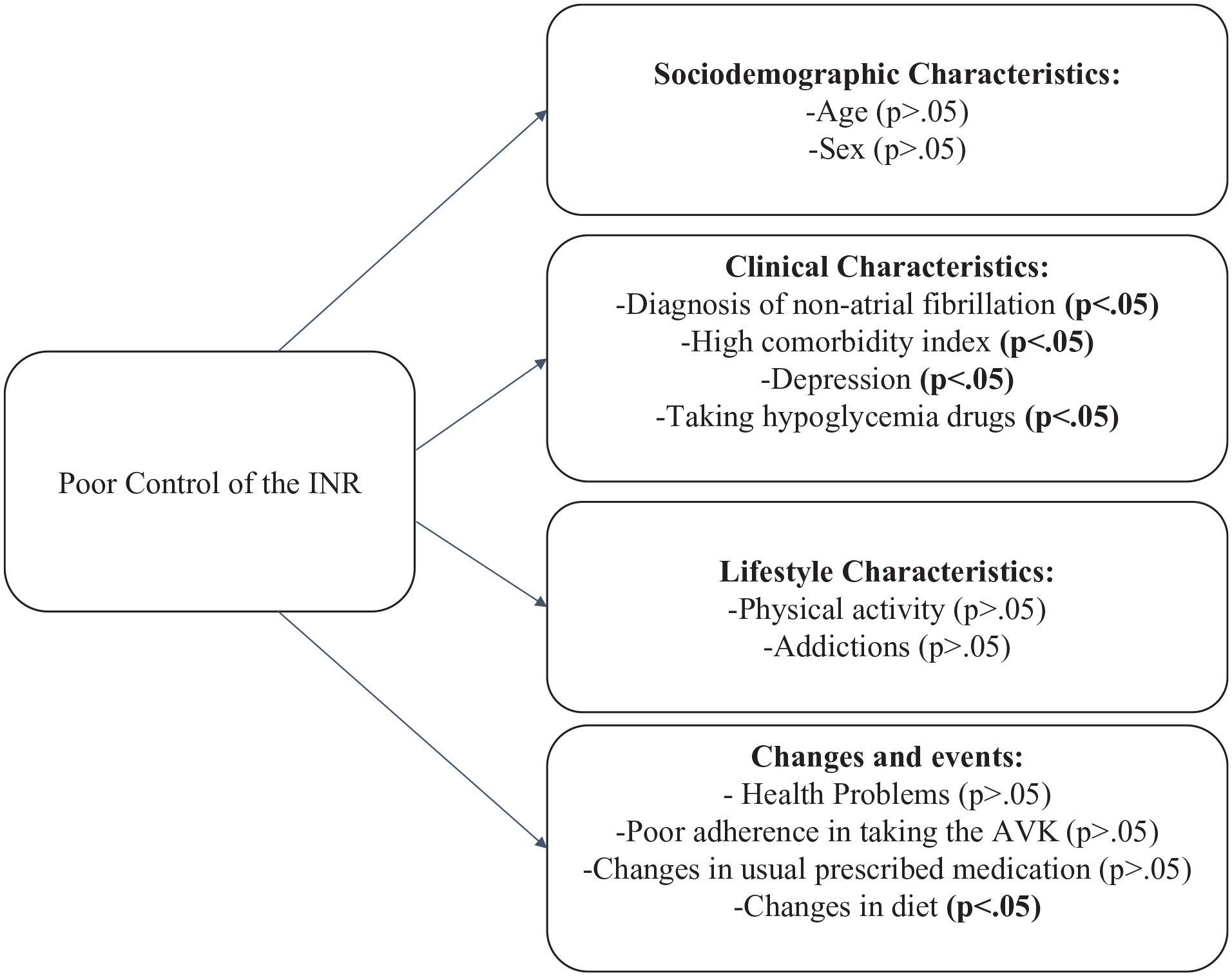
Relationship of INR control with clinical characteristics, social support, lifestyle, and changes and events.
This study has some strengths and weaknesses. First, given the variability in INR values, which has been widely described and has many causes, only the best-known influencing factors have been taken into consideration in our study. Second, the variance in the dependent variable explained by the regression model is low. One possible explanation could be that some of the factors studied are present in only a smaller number of people, preventing them from reaching statistical power. Despite these limitations, it should be noted that although there are studies on treatment with vitamin K antagonists, there is no previous research focused on the follow-up of these patients with similar variables in the area of primary care.
Conclusions
Almost half of the people who were controlled for vitamin K antagonist therapy in a primary care setting were found to have good INR control. The diagnosis of non-atrial fibrillation, having comorbidities, depression, and taking hypoglycemia drugs were associated with worse control of the INR. Making changes to one’s usual diet was also associated to more INR controls being outside the normal range.
Despite the proven efficacy of vitamin K antagonists in the treatment of cardiovascular diseases, particularly atrial fibrillation, there are still many people who have poor INR control. The present study highlights the characteristics that favor within range INR values for people controlled for vitamin K antagonist therapy in primary care settings. These characteristics can guide us in developing care strategies that optimize the management of this therapy in the most efficient and cost-effective manner.
Footnotes
Acknowledgements
The authors thank the patients for their participation in this study.
Author Contributions
Conceptualization, G.R.G., R.S.S., D.C.L., and R.J.Q.; Methodology, G.R.G., R.S.S., and J.G.O.; Software, G.R.R., R.S.S., and D.C.L.; Validation, G.R.G., D.J.C., and R.S.S.; Formal Analysis, G.R.G., R.S.S., and J.G.O.; Investigation, G.R.G., R.J.Q., J.F.V., J.V.V., D.C.L., and S.M.J.; Data Curation, G.R.G., R.S.S., and D.J.C; Writing—Original Draft Preparation, G.R.G., R.S.S., and D.C.L.; Writing—Review & Editing, G.R.G., R.S.S., D.C.L., D.J.C., and S.M.J.; Visualization, G.R.G., D.C.L.; Supervision, R.S.S.; Project Administration, G.R.G., R.S.S.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Institutional Review Board
This study was approved by the territorial research ethics committee (Dr. Josep Trueta Hospital, CEIM: 2021.064).