
Abstract
Introduction/Objective:
The prevalence of Type 2 Diabetes Mellitus is increasing in the older American population, especially Mexican Americans. Sleep disorders are common in older adults with T2DM. This study examined the relationship between T2DM-related complications and sleep complaints in older Mexican Americans over 9 years of follow-up.
Methods:
Study included 310 participants aged 77 years or older with self-reported diabetes from the Hispanic Established Population for the Epidemiological Study of the Elderly (2007/08-2016).
Results:
Of the 310 participants, the mean age was 82.04 years. The cohort had significantly more females (69.03%) than males (30.97%). A substantial number of participants had trouble falling asleep (16.13%), waking up several times (36.45%), trouble staying asleep (15.16%), and feeling tired and worn out after waking up (12.90%). The percent of diabetes complications were 70.2% for circulation problems, 58.2% for eye disorders, 15.9% for kidney disease, and 4.4% for amputation. Participants who experienced sleep complaints for 15 or more days in a month were more likely to experience diabetic complications.
Discussion:
This study demonstrated a significant relationship between T2DM macro- and micro-vascular complications and increased risk of sleep disorders in older Mexican Americans.
Keywords
Introduction
Type 2 Diabetes Mellitus (T2DM) is a serious global health issue with a significant impact on the health of people and use of health resources. 1 According to the Centers for Disease Control and Prevention (CDC), approximately 23.4 million people in the United States suffer from T2DM, and the prevalence of diabetes has increased from 0.93% in 1958 to 7.4% in 2015. 2 According to the CDC, 25% or more of the U.S. population aged ≥65 years have diabetes. 3 Diabetes in older adults is linked to higher mortality, reduced functional status, and increased risk of institutionalization. 4 The prevalence of these adverse outcomes is particularly high among the growing number of older Hispanics, a population with high rates of diabetes.4,5
The Hispanic population is one of the fastest growing ethnic communities. As of 2016, an estimated 58 million Hispanics were living in the U.S., 64% of whom were Mexican Americans. 6 T2DM is a major health concern in the Hispanic population. An estimated 2.5 million Hispanic Americans above the age of 20 suffer from T2DM. 7 Among the older adult population, T2DM is associated with disabling complications (eg, coronary heart, cerebrovascular and peripheral vascular disease, retinopathy, and neuropathy)4,5,8 and with geriatric syndromes (eg, falls, dementia, and sleep disorders).5,9
Sleep disorders, in particular, have been understudied in the context of the growing number of older Hispanics with diabetes. About 70 million Americans suffer from sleep disorders including insomnia, obstructive sleep apnea, and chronic partial sleep deprivation. 10 Persons experiencing sleep insufficiency are more likely to suffer from chronic diseases such as hypertension, diabetes mellitus, depression, obesity, and cancer; have increased mortality; and have reduced quality of life and productivity. 11 Mounting evidence links sleep deprivation, obesity, and sleep-related breathing to diabetes. 12 However, the data on the association between T2DM and sleep have largely derived from white and young-old populations, 13 with little data on the growing number of old-old (≥80 years) and non-White older adults. In the 2017 Standards of Care for diabetes patients, the American Diabetes Association (ADA) strongly recommended “the assessment of sleep pattern and duration as part of the comprehensive medical evaluation based on emerging evidence suggesting a relationship between sleep quality and glycemic control.” 14 Sleep disturbance is a significant geriatric syndrome among older adults, yet little is known about the sleep-diabetes association in old-old diabetic patients, especially the older Mexican Americans (the majority of US Hispanics) who have a high prevalence of T2DM and sleep problems. A study analyzing data from 1085 Mexican Americans aged 75 years and older revealed a significant prevalence of sleep problems ranging from 9% to 30%. 15
While the relationship between T2DM and sleep disorders has been studied previously, most of these studies have been conducted among non-Hispanic groups. Little is also known about the extent to which different diabetic complications (macro- and micro-vascular complications) associate with new-onset of sleep disorders. Since older Mexican Americans suffer from high rates of T2DM, further research with rigorous analysis of both sleep disorders and DM among the Mexican American elderly is warranted. This study examined the relationship between DM-related complications and sleep complaints in older Mexican Americans with T2DM over 9 years of follow-up.
Methods
Sample and Procedures
Data used came from the Hispanic Established Populations for the Epidemiological Study of the Elderly (EPESE). The Hispanic EPESE is an ongoing longitudinal study based on interviews conducted with noninstitutionalized Mexican Americans aged 65 years and older, residing in 5 southwestern states (Texas, California, Arizona, Colorado, and New Mexico). The sampling plan and cohort characteristics have been described previously by Markides et al. 16 Information and data for the Hispanic EPESE is available at the National Archive of Computerized Data on Aging (NACDA). The original Hispanic EPESE sample consisted of 3050 participants interviewed in 1993/94 at baseline and followed up every 2 or 3 years. Nine waves of data have been completed as of 2016. In 2004 to 2005 (Wave 5), 1167 participants from the original cohort aged 75 years and older were re-interviewed. A new sample of 902 respondents aged 75 years and older was added, using sampling procedures similar to those used in 1993/94. Both cohorts received identical evaluations at baseline and follow up. In-home interviews were conducted in Spanish or English based on the respondent’s preference.
The present analysis used data from Waves 6 (hereafter referred as baseline) through 9. Wave 6 was selected as the baseline because questions on sleep complaints were first collected in Wave 6. Of the 1542 participants aged 77 years and older who were interviewed at Wave 6 (2007/08), 1006 completed at least 1 follow up, either at Wave 7 (2010/11), Wave 8 (2012/13), or Wave 9 (2016). Among these 1006 participants, 1003 had complete information on diabetes and diabetes-related complications at baseline. The final sample for this study was the 310 participants who reported having diabetes and had complete information on sleep complaints.
Sleep Measures
To assess sleep complaints, participants were asked how often in the past month they experienced the following: “have trouble falling asleep,” “waking up several times per night,” “difficulty staying asleep,” and “waking up after the usual amount of sleep feeling tired and worn out.” The frequency of sleep complaints in a month was reported as “Not at all,” “1-3 days,” “4-7 days,” “8-14 days,” or “more than 15 days.” Frequency of sleep complaints were the main outcome variables analyzed as <15 and ≥15 days. We classified symptoms for ≥15 days as severe. According to the International Classification of Sleep Disorders (AASD, 2014) sleep disorder symptoms (such as insomnia) are considered severe if they occur at least 3 times per week.
Diabetes Measures
Participants were asked if a doctor had ever said that they have diabetes, sugar in their urine, or high blood sugar. Participants who reported a diabetes diagnosis were asked about disease duration (categorized as ≤10 and >10 years) and treatment received (categorized as insulin and non-insulin). Participants were asked if as a result of diabetes, they had problems with their kidneys, eyes, circulation (arms or legs), or if they have had any part of their body amputated.
Covariates
Baseline sociodemographic variables included age, gender, marital status, and years of formal education. A series of questions were asked to assess the presence of various medical conditions by asking participants if a doctor had ever told them that they had arthritis, hypertension, heart attack, heart failure, stroke, cancer, or hip fracture. These medical conditions were summed to obtain a total comorbidity score. BMI was computed as weight in kilograms divided by height in meters squared. Cognitive functioning was assessed using the Mini Mental Status Examination (MMSE). 17 The English and Spanish versions of the MMSE were adopted from the Diagnostic Interview Scale and have been used in prior community surveys.18-20 Depressive symptoms were measured using the Center for Epidemiologic Studies Depression (CES-D) scale. 21
Statistical Analysis
Chi-square and analysis of variance (ANOVA) tests were used to examine the distribution of covariates for participants by sleep complaint status at baseline. A generalized linear mixed model (GLMM) using the GLIMMIX procedure in SAS 22 with the logit link function to estimate the odds ratio and 95% Confidence Interval for each of the 4 sleep complaints for 15 or more days as a function of T2DM complications over 10-year of follow up. T2DM complications and sleep complaints were assessed at each wave and analyzed as time dependent variable. The partial effect of diabetes complications was estimated after controlling for baseline socio-demographics, number of comorbidities, BMI, depressive symptoms (CES-D score), cognitive function, and any sleep complaints at baseline. Those participants who died, refused to be interviewed later, or were lost to follow-up were included in the study until their last follow-up. Additional analyses using logistic regression model to examine the factors associated with sleep complaints at Wave 6 (baseline). All tests of significance were 2-sided with a P-value <.05. Analyses were performed using the SAS 9.4 (SAS Institute, Inc., Cary, NC).
Results
Table 1 shows the baseline characteristics of the final sample. Of the 310 participants, the mean age was 82.04 years (SD = 3.62 years). The cohort had significantly more females (69.03%) than males (30.97%). The mean MMSE score was 22.24 (SD = 6.76); mean CES-D score was 9.86 (SD = 9.10); and mean comorbidity score was 1.92 (SD = 0.98). A substantial number of the 310 subjects reported trouble falling asleep (16.13%), waking up several times (36.45%), trouble staying asleep (15.16%), and waking up after their usual amount of sleep feeling tired and worn out (12.90%). Approximately 40% of the 310 participants reported having any of the above sleeping problems for 15 or more days in a month.
Baseline Descriptive Characteristics of the Final Sample (N = 310).

Abbreviations: CES-D, Center for Epidemiological Studies Depression Scale; MMSE, mini mental state examination; SD, standard deviation.
Comorbidities were computed as a summed disease burden of self-reported physician diagnosed hypertension, arthritis, heart attack, heart failure, stroke, cancer, and hip fracture.
Approximately 22% of the 310 participants reported using insulin injections. Half (50.97%) had experienced any kind of diabetic complications. Among the 158 participants who reported having experienced diabetic complications, the majority of the complications were in the eye (58.23%) and circulation (70.25%). Diabetic complications in the kidney were less common (15.19%) and few participants reported having an amputation (4.43%). Lastly, 37.34% of complications were a combination of both macro and micro, 32.91% were solely macro, and 29.75% were solely micro.
Figure 1 presents the distribution of participants who reported sleep complaints for 15 or more days across the 4 observation waves. The bar graphs indicate that the most frequent sleep complaint was “waking up several times per night” and the second most frequent was “have trouble falling asleep.”
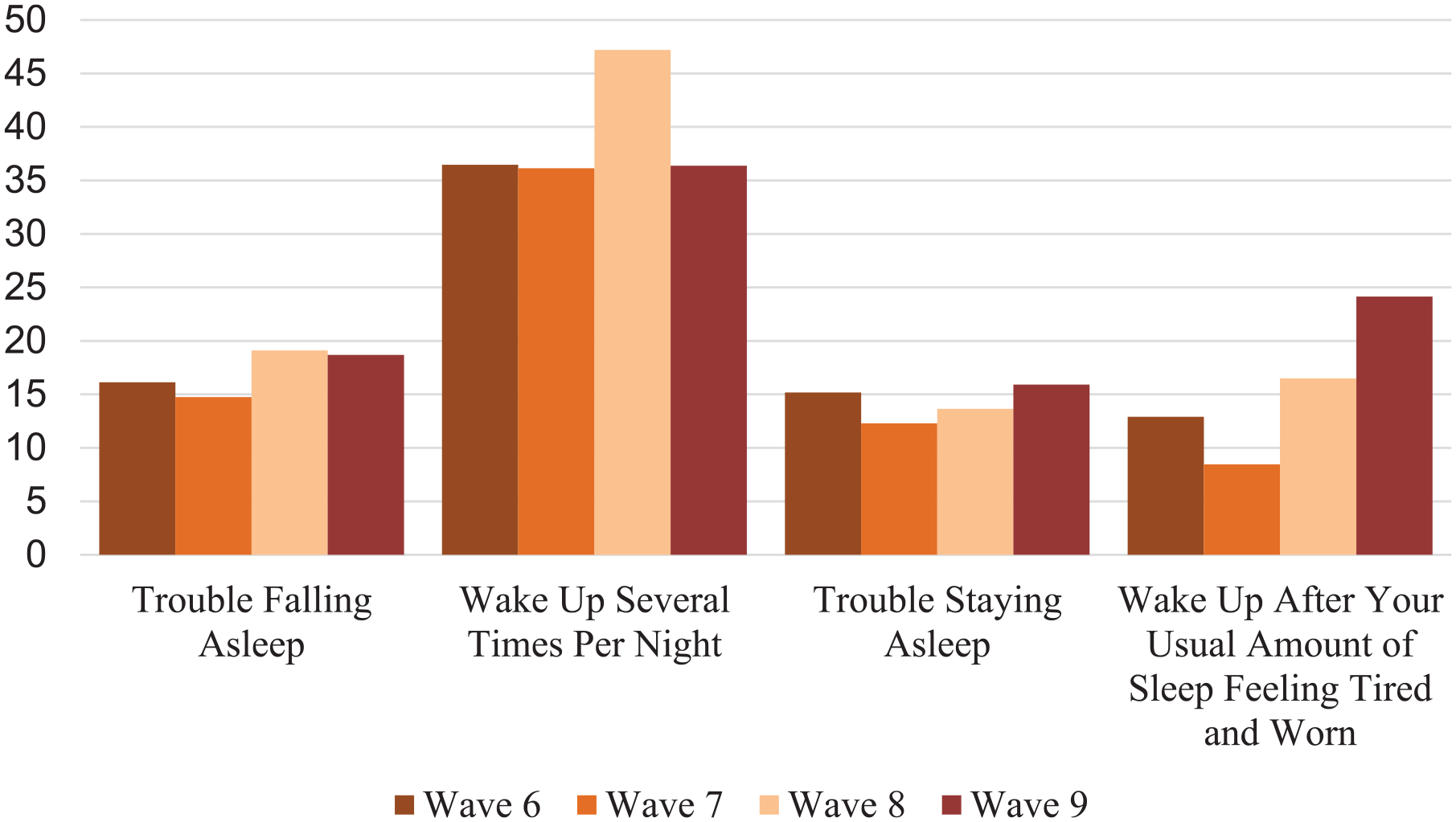
Percent of sleep complications at each wave of interview (N = 310).
Table 2 shows the descriptive characteristics of participants according to sleep complaints. Results showed that participants who experienced “have trouble falling asleep” for 15 or more days (72%) had significantly greater percentages of experiencing diabetic complications than those who experienced this sleep complaint for less than 15 days (46.92%). Participants who experienced “waking up several times per night” for 15 or more days had significantly greater percentages of experiencing diabetic complications (59.29%) than those who experienced this sleep complaint for less than 15 days (46.19%). Participants who had “difficulty staying asleep” for 15 or more days had significantly greater percentages of experiencing diabetic complications (70.21%) than those who experienced this sleep complaint for less than 15 days (47.53%). Participants who experienced “waking up after the usual amount of sleep feeling tired and worn out” for 15 or more days had significantly greater percentages of experiencing diabetic complications (75%) than those who experienced this sleep complaint for less than 15 days (47.41%).
Baseline Descriptive Characteristics of the Final Sample by Sleep Complains of Older Mexican Americans With Type 2 Diabetes Mellitus (N = 310).

Abbreviations: CES-D, Center for Epidemiological Studies Depression Scale; MMSE, mini mental state examination; SD, standard deviation.
Comorbidities were computed as a summed disease burden of self-reported physician diagnosed hypertension, arthritis, heart attack, heart failure, stroke, cancer, and hip fracture.
P-value < .05.
Table 3 presents the results from 4 GLMM analyses to assess the OR of sleep complaints for 15 or more days over a 10-year period as a function of diabetes-related complications. Having any sleep complaints at baseline (OR = 2.49; 95% CI = 1.22-5.05) was associated with “trouble falling asleep” in the past month. Having macro-diabetic complications (OR = 3.51; 95% CI = 1.81-6.81), micro-complications (OR = 3.30; 95% CI = 1.66-6.56), both macro- and micro-diabetic complications (OR = 3.35; 95% CI = 1.84-6.12), and any sleep complaints at baseline (OR = 1.78, and 95% CI = 1.09-2.90% CI) were associated with “waking up several times per night.” Any sleep complaints at baseline (OR = 2.62; 95% CI = 1.10-6.23) and having macro- and micro-diabetic complications (OR = 2.73; 95% CI = 1.03-7.21) were significantly associated with “difficulty staying asleep.” Having macro- and micro-diabetic complications (OR = 3.70, and 95% CI = 1.45-9.49% CI), high depressive symptoms (OR = 1.06; 95% CI = 1.02-1.11), and any sleep complaints at baseline (OR = 2.57; 95% CI = 1.12-5.89) were significantly associated with “waking up after the usual amount of sleep feeling tired and worn out.”
Generalized Linear Mixed Modeling Analyses for Sleep Complaints as a Function of Diabetes Complications Over 10-Year of Follow-Up in Older Mexican Americans With Type 2 Diabetes Mellitus.
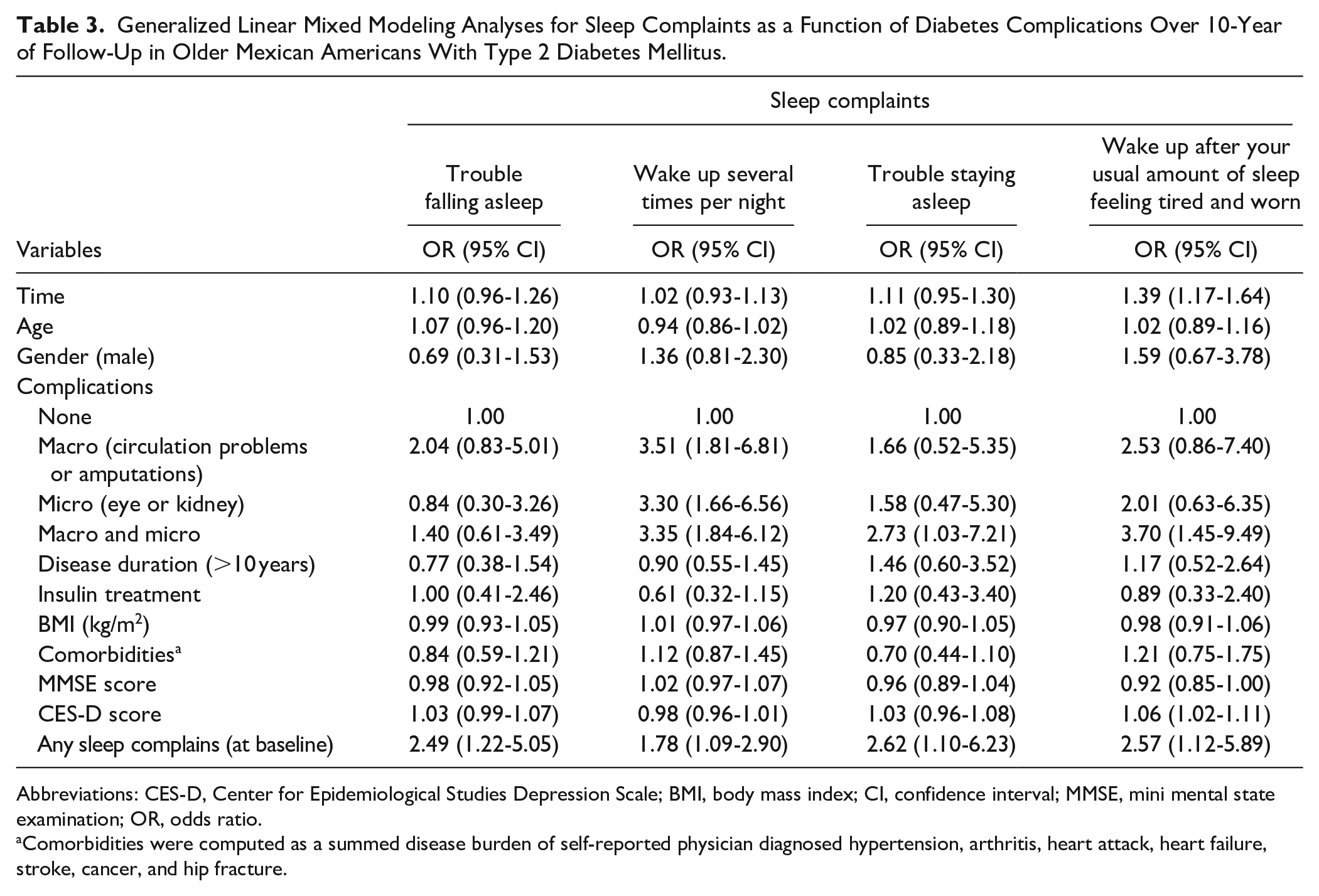
Abbreviations: CES-D, Center for Epidemiological Studies Depression Scale; BMI, body mass index; CI, confidence interval; MMSE, mini mental state examination; OR, odds ratio.
Comorbidities were computed as a summed disease burden of self-reported physician diagnosed hypertension, arthritis, heart attack, heart failure, stroke, cancer, and hip fracture.
Additional analyses were conducted to examine the factors associated with sleep complaints at Wave 6 (baseline). We found high BMI and high depressive symptoms associated with “difficulty staying asleep” in the past month (OR = 1.07, CI = 1.00-1.13, OR = 1.10, and 95% CI = 1.06-1.14% CI, respectively). High number of comorbidity score was associated “waking up several times per night” (OR = 1.31, CI = 1.00-1.71). High BMI, high depressive symptoms, and macro-diabetic complications were associated with “trouble falling asleep” (OR = 1.07, CI = 1.01-1.14, OR = 1.08, and 95% CI = 1.04-1.12% CI, and OR = 2.87, and 95% CI = 1.11-7.38% CI, respectively). High depressive symptoms were associated with “waking up after the usual amount of sleep feeling tired and worn out” (OR = 1.10, CI = 1.07-1.16).
Discussion
This study sought to investigate the relationship between T2DM-related complications and sleep disorders in community-dwelling elderly Mexican Americans, one of the fastest growing segments of the US aging population. Overall, the study demonstrated a significant association between T2DM macro-and micro-vascular complications and increased risk of frequent night awakening and awakening feeling tired and non-rested. T2DM participants with any diabetic complications were more likely to have experienced sleep complaints for 15 days or more. As expected, baseline sleep concern and high depressive symptoms were significantly associated with awakening feeling tired and non-rested. Unlike prior studies in younger or non-Hispanic populations,23-25 diabetes duration, insulin use, comorbidity burden, and cognitive function were not significantly associated with increased odds of reporting sleep complaints.
The results of this study align with a large body of research that suggests diabetes and sleep problems are inter-connected. An analysis by Cho et al 26 found that 50% to 70% of patients diagnosed with T2DM experience different types of sleep disorders including insomnia, daytime sleepiness, and poor sleep. The population studied was middle-aged patients with a mean age of 59 years. Existing research studies26,27 provide biological, epidemiological, and behavioral evidence of a close and significant connection between sleep and T2DM. The present findings of Cespedes et al 28 support previous research in Hispanic populations that found a connection between T2DM and sleep complications. However, the focus of Cespedes et al 28 was on middle-aged and older women. Based on their analysis, they found that chronic short sleep duration resulted in an increased risk of T2DM. Our study showed that this relationship might be bidirectional as our data showed that T2DM complications were also associated with increased odds of sleep disorders.
In a systemic review, Leong et al 29 observed a relationship between sleep apnea and diabetic nephropathy. Our study supports this finding by showing evidence of increased frequency of sleep complaints in older Mexican Americans with diabetic complications. Similarly, Nishimura et al 13 studied 136 middle-aged non-Hispanic patients and reported that sleep disorder breathing contributed to the development of diabetic retinopathy. Diabetic eye complications were among the most commonly reported diabetes complications in our study. Lee et al 30 even provided an explanation for a causal relationship between sleep disorders and the development of T2DM by showing that poor sleep quality independently increases the incidence of diabetes.
Evidence supports a bidirectional association between sleep disorders and T2DM. Sleep disorders are associated with an increased risk for elevated HbA1c levels, and high HbA1c is a risk factor for sleep disorders. 31 Sleep disorders such as obstructive sleep apnea, insomnia, and chronic and partial sleep deprivation are associated with the development of T2DM, diabetic neuropathy, poor glycemic control, and overnight hypoglycemia. 29 Short sleep duration is associated with reduced insulin sensitivity and impaired β-cell function. 32 The relationship between T2DM and sleep disorders may be due in part to the high prevalence of sleep disorders such as obstructive sleep apnea among adults with obesity, a known risk factor for T2DM. 33 T2DM in turn is also associated with initiation and maintenance of sleep difficulties. However, little is known about the effect of T2DM on the full range of sleep concerns, especially in the old (75-84 years) and oldest-old (≥85 years). Research indicates that 50% to 70% of patients diagnosed with T2DM experience some form of sleep disorders. 26
Sleep disorders also worsen diabetes complications. Studies have shown a relationship between sleep disorder breathing and diabetic retinopathy. The degree of intermittent hypoxia associated with respiratory events during the nighttime is an important factor in diabetic retinopathy. 13 Other studies also suggest a likely 2-way association between obstructive sleep apnea and diabetic kidney disease. 34
Study Limitations
Our study has some limitations. First, the Hispanic EPESE does not collect polysomnography data. This fact precludes us from a more rigorous analysis of the association between sleep apnea, T2DM, and diabetes-related complications, especially among participants with “waking up and still feeling tired and worn,” an important symptom of sleep apnea, a subpopulation who will be candidates for future effective interventions such as continuous positive airway pressure (CPAP). Second, measures for sleep assessment, diabetes, and medical conditions were based on self-report, which can produce recall bias. This is important to consider in this analysis, given the sample population were 77 years and older. Short et al 35 studied accuracy of self-recall among patients and concluded that male, young patients, and those with higher education can have better recall than their counterparts. Short recall duration was also linked to accuracy. Although there is a significant association between sleep apnea, T2DM, and diabetes-related complications, there is insufficient empirical evidence to support the causality of these findings. Our findings only showed associations—not causal relationships—between DM-complications and sleep disorders.
Study Impact
Nevertheless, with these findings, health professionals, and subsequently the public, can gain a better understanding of the nature of T2DM and how it affects one’s health, particularly in terms of sleep schedules. Physicians, nurse practitioners and physician assistants caring for older patients with diabetes need an acute clinical awareness of the high rates of sleep concerns in this population and have a high level of suspicion for a wide range of sleep disorders, from circadian rhythm disturbances to the more serious sleep apnea disorders. Our findings thus underscore the need to incorporate screening for sleep disorders in persons with diabetes, especially those with DM-complications. Early diagnosis and management of sleep disorders has the potential to improve quality of life and survival, and lower cost of care in elderly patients with T2DM.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Institutes of Health/National Institute on Aging (R01-AG010939, R01MD010355). The study sponsors had no role in the study design, analysis, or interpretation of the data. Study sponsors did not have any role in the writing of the article or the submission to a journal.