
Abstract
Introduction:
Assisted suicide and euthanasia are controversial issues today and have been throughout the history of humanity, mainly because there are individuals for and against them. Currently, the legalization of these practices is being discussed in Chile, and the perception of physicians regarding this issue is unknown. Therefore, this study aimed to assess physicians’ perception of Chile’s euthanasia and assisted suicide.
Methods:
A nationwide cross-sectional study was carried out in Chile. A questionnaire of physicians’ attitudes and opinions on assisted suicide and euthanasia was used. The population was the doctors who work in Chile, and the sample was convenient with a sample calculation of 384 physicians. About 20 variables were considered and included in a form created through the Google forms option, which was distributed through social networks: LinkedIn, Facebook, Twitter, and WhatsApp. To guarantee the anonymity of the participants, the option to request and remember the participant’s email was deactivated. A generated database allowed the quantitative analysis of the variables and their expression through frequencies, percentages, and graphs. The European University of the Atlantic’s research ethics committee approved this study as stated in the document CE-55 of March 2021.
Results:
A total of 410 physicians were surveyed. 50.7% (n = 208) of the participants identified themselves as men, and 69.8% (n = 286) were Chilean. The city of Santiago was the area of residence of 72.9% (n = 299) of the participants. About 34.6% (n = 142) of participants were general practitioners, and 39.3% (n = 161) of the physicians had more than 20 years of experience. About 68.7% had favorable attitudes toward euthanasia and 54.4% toward assisted suicide; However, although the majority favored legalizing euthanasia and assisted suicide, approximately 48.8% stated that they would not participate in an assisted suicide procedure.
Conclusions:
There was evidence of support for the implementation and legalization of euthanasia and assisted suicide by physicians in Chile. However, there are still professionals who have not yet decided on a definitive position on these practices.
Introduction
Assisted suicide and euthanasia are controversial issues today. Exist individuals for and against, as well as institutions and religious creeds that have taken sides against the topic. 1 The interpretation of the word “euthanasia” as a good death according to its etymological origin has generated ethical and social conflicts. Mainly because death is a loss, it is difficult to understand it as something positive additionally, several historical events, such as the Nazi experiments, related the term euthanasia more to murder than to a kind and compassionate act. 1 More current texts mention that euthanasia is that process in which, through the use or abstention of clinical measures, in the case of a patient in an incurable or terminal condition, can accelerate death to avoid excessive suffering. Can explain that the difference between assisted suicide and euthanasia occurs because, in the first situation, the patient takes the final action; however, for some authors, both practices are brought together under the term of assisted death. 2 Therefore, euthanasia is currently understood as the deliberate intervention to end a patient’s life with no prospect of cure. At the same time, assisted suicide corresponds to the help or assistance of another person who wishes to end their life. Assisted death is a generic term for help to die that can refer to euthanasia or assisted suicide.1,2 Several countries legally authorize assisted death, including the Netherlands, Luxembourg, and Canada. Other countries such as Belgium and Colombia have regulations that decriminalize euthanasia, and other places have additionally legislated on assisted suicide; within those territories are Switzerland and 5 states of the United States of America, specifically Oregon, Vermont, Washington, California, and Montana.2,3 Spain recently joined the list of countries that have legislated on euthanasia through Organic Law 3/2021 of March 24, which regulates euthanasia in public and private institutions. 4
Delving deeper into the crucial aspects of the definition of assisted dying, some authors think that some elements are essential in the term itself, such as the fact that it is an event that seeks to cause death and looks to eliminate the suffering. Other elements in the definition of assisted death are (1) the patient’s consent, which must be granted respecting autonomy and freedom; this refers to the fact that must not coerce the patient in any way. (2) Another aspect is the terminal nature of the disease, which must be irreversible and generate precariousness in the last days of life, in a condition in which it is inherent to think of a loss of the person’s dignity. (3) Furthermore, the painless nature of the death caused (through the use of drugs such as high-potency analgesics, such as opioids, high-potency muscle relaxants, and even anesthetic drugs) is also taken into account. (4) Finally, the health context in which the action occurs (essential in some legislation to be considered euthanasia).5,6
Nonetheless, another crucial element in this scenario is the will of the professional who performs the procedure and is legally responsible for clinical decisions, that is, the physician. In this context, it is essential to remember that the medical oaths of Hippocratic roots that are made at the time of graduation of professionals are mostly categorical when mentioning the rejection of the practice of euthanasia and assisted suicide. 7 It is also important to say that many of the oldest universities in the Western world originated through the Catholic Church. For that reason, the creed condemned the practice of euthanasia and continues to blame it to this day, a situation that leads doctors trained in these schools to behave based on humanistic principles under the protection of faith and religion and therefore reject the possibility of euthanasia.8,9
Currently, in Chile, the bill “Dignified death and palliative care” is being debated in Congress, which seeks to regulate the issue of euthanasia and assisted suicide in the country. Similar to the reality of several Latin American countries, actually Chile does not have a law on euthanasia or assisted suicide, nor is this type of practice decriminalized in the national territory; Even several professionals, despite knowing the situation of patients suffering from a terminal and irremediable illness, have difficulty identifying how far the care of the patient goes and where the postponement of suffering begins. Additionally, the congress is currently discussing the project that, if regulated, would allow euthanasia and assisted suicide in Chile; This is why it is important to know the attitudes of medical professionals, who ultimately are the ones who would be in charge of monitoring these practices and participating in them, in the eventual case that the law is sanctioned in favor of what is has called “a dignified death.” Additionally, the interest of bioethics in this area makes it especially necessary to research this topic, to take into account the attitudes of physicians, who, together with other health professions, will address day-to-day the care of these patients.
The importance of this research additionally is based on the current scientific literature, where no study was found that addresses this issue in the medical population of Chile. In fact, in 2018, a bibliometric analysis study on the euthanasia publications available in the Scopus, Medline, and Scielo databases revealed that Latin America has a very low scientific production regarding the subject of euthanasia. 10 Additionally, the Chilean medical association 2019 surveyed its associates, finding that of the professionals who answered the questionnaire, 59% mentioned that they would be willing to participate in a medically assisted death procedure, provided that they were met the requirements to carry out this procedure. However, apart from these data, it was impossible to find other texts that referred to the subject or addressed the attitudes of medical professionals in Chile regarding euthanasia or medically assisted suicide. 11 Due to the above, it was proposed to study the perception of physicians who work in Chile toward assisted suicide and euthanasia.
Methods
The reporting of this study conforms to The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines that were created to aid the authors in ensuring high-quality presentation of the observational studies. 12
Study Design
Cross-sectional study.
Setting
The study was carried out in Chile, a long, narrow country that straddles the western edge of South America, with more than 6000 km of coastline on the Pacific Ocean. Santiago, its capital, is located in a valley surrounded by the Andes and the Cordillera de la Costa. The study was carried out from January to December 2021. Recruitment began on January 15, 2021, and ended on December 30, 2021. Data collection was done through a web form that is described in the data sources/measurement section.
Participants
The population/universe were the doctors who work in Chile, which correspond to 53 344 professionals, according to the registry of individual providers of the health superintendence of the Chilean Ministry of Health (data as of July 1, 2021).
Variables
Twenty variables were considered and included in a form developed through the Google forms option, which was distributed via the Internet. The independent variables were: age, sex, Chilean city of residence, medical specialty, years of professional practice, country of graduation, and nationality.
The dependent variables came from the questionnaire and were: point of view of assisted suicide; point of view on euthanasia; thinking about whether people should be able to decide their death freely; attitude about whether it should be accepted that other people help someone to die if asked; thinking about whether life is a higher value than the autonomy of the person; respect for autonomy as a good superior to life; life and autonomy as values that deserve respect and must be contextualized; knowledge about the current law on assisted suicide and euthanasia; consideration of whether the law on assisted suicide/euthanasia should change; point of view about whether assisted suicide and euthanasia should be legalized; considerations on participation in an assisted suicide procedure and euthanasia.
Data Sources/Measurement
The questionnaire of attitudes and opinions on assisted suicide and euthanasia in physicians by Rodríguez-Calvo et al 13 was used, which consisting of a 5-level Likert-type survey measurement, where 1 means totally disagree, and 5 totally agree. As mentioned in their manuscript, the authors validated this instrument and reviewed its viability by conducting a pilot test that included 12 individuals. Later, they made the appropriate adjustments to refine the survey. 13
The form’s web link was taken and distributed through social networks: Facebook, Twitter, LinkedIn, and WhatsApp to disseminate the questionnaire. Obtained Written informed consent from all participants involved in the study and, to guarantee anonymity in the answers, an email was created to which only the researchers had access and from where the Google form was designed. With the same email, accounts were created on social networks with the name of the study and were used exclusively for this purpose. Additionally, in the data collection options, the option to request participants to enter with an account was deactivated; therefore, access to the form was not linked to the email addresses of the participants; identification data was not requested.
As selection criteria, it was considered as inclusion criteria that the participants were national or foreign doctors with studies in the country or outside that currently work in Chile and doctors belonging to all medical specialties. Regarding the exclusion criteria, doctors who did not exercise their clinical practice in the country were not considered, nor were doctors in training, for example, interns.
The original questionnaire had 17 items and was divided into 4 sections: (1) demographic data: age, gender, program of study, and a question about the respondent’s opinion about the importance of ethics in the health professions curriculum; (2) participants’ attitudes toward assisted suicide and euthanasia and their ethical reasoning; (3) knowledge and opinion about the law, and (4) willingness to participate in assisted suicide and euthanasia, if legalized.
The original questionnaire was carried out in Spain, in the Spanish language, and applied to health sciences professionals in training and validated through a pilot test in a small group of students (n = 12) and then refined with qualitative validation by experts.
To apply it to this work to know the perception of physicians working in Chile toward assisted suicide and euthanasia, we decided to include 3 additional questions in the first demographic data section; these questions were (1) specialty, (2) years of professional practice, and (3) country of graduation. We sent the questionnaire to 10 bioethics experts to assess content validity, and they made their corrections and suggestions, with which we refined the manuscript. Additionally, a pilot test was carried out with 50 participants, and the internal consistency was measured through exploratory and confirmatory factor analysis, finding the same structure proposal in the original study. Also, we found a result in the Kaiser-Meyer-Olkin test of sampling adequacy of .89; a Bartlett sphericity test with a significance <.001. The anti-image correlation had all values higher than .86, verifying the construct validity. In addition, we measured internal consistency through the Cronbach’s Alpha of the questionnaire, which was .88.
Bias
To reduce the risk of measurement bias, the questionnaire was validated qualitatively and statistically. To reduce the risk of random error, a sample by sample was used for convenience with a sample calculation that was representative of the target population.
Study Size
The sample corresponded to a convenience sample with a sample calculation. For calculating the sample and taking into account that it is known how many doctors are registered in the registry of individual providers of the Ministry of Health of Chile but exceed 10 000 individuals, the formula for calculating the sample in an infinite population was used. In this way, the representative sample of the total population of professionals was 384 doctors.
n = Z2.P.q/d2; n = Z2.(P).(1 − P)/d2; n = (1.96)2.(.5).(1 − .5)/(.05)2; n = (3.84).(.5).(.5)/.0025;
n = .96/.0025; n = 384
n = sample size; Z = critical Z value, calculated from the normal curve area tables. Also called confidence level; d = level of absolute precision. Referred to the amplitude of the confidence interval desired in the determination of the average value of the variable under study; P = approximate proportion of the phenomenon under study in the reference population; q = proportion of the reference population that does not present the phenomenon under study (1 − P). The sum of P and q must always give 1. For example, if P = .8 then q = .2.
Statistical Analysis
Data from the Google form was exported to a Microsoft Excel digital spreadsheet. Subsequently, the data was exported to the statistical software IBM SPSS (Chicago, IL) version 25. Quantitative variables such as age were analyzed using measures of central tendency such as mean and median, with their respective measures of dispersion such as standard deviation and the interquartile range. Qualitative variables such as gender, nationality and others will be coded using numbers. An analysis was performed using absolute and relative frequencies using the same software. Graphs and tables were also made to show the answers to the questionnaire in an illustrative way.
Results
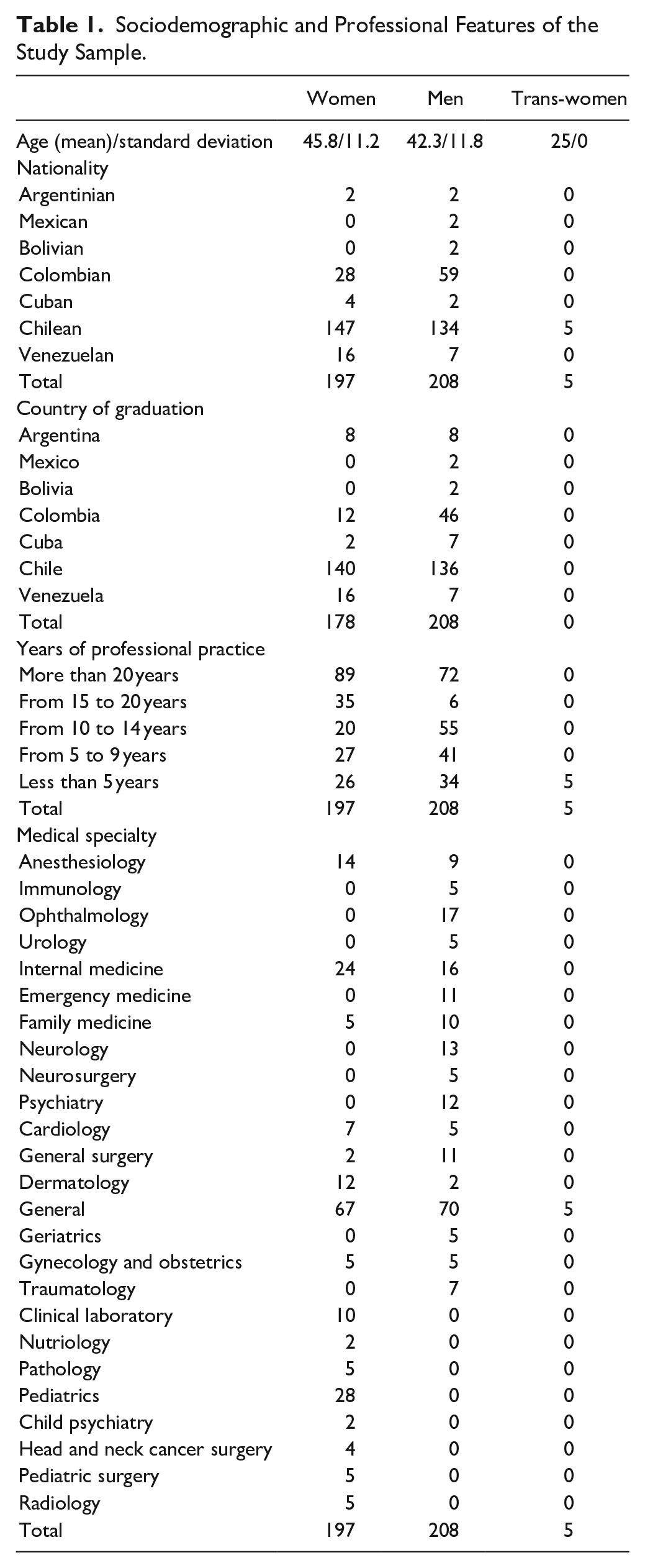
A total of 420 surveys were answered by medical professionals, of which 10 were discarded because they were answered by professionals who did not work in Chile. Regarding age, the median was 42 years (IQR 22); the youngest participant was 25 years old, and the oldest participant was 70 years old. About 17.6% (n = 72) of the participants were 56 years old. About 50.7% (n = 208) of the participants identified themselves as men, 48% (n = 197) as women, and 1.2% (n = 5) as transgender women. About 69.8% (n = 286) were Chilean, 21.2% (n = 87) Colombian, 5.6% (n = 23) Venezuelan, 1.5% (n = 6) Cuban, 1% (n = 4) Argentines, and finally Bolivians and Mexicans 0.5% (n = 2) each one. All demographic data is shown in Table 1.
Sociodemographic and Professional Features of the Study Sample.
The city of Santiago was the area of residence of 72.9% (n = 299) of the participants, followed by the city of Viña del Mar in 7.3% (n = 30) and Concepción in 6.8% (n = 28). The entire distribution according to the town of residence is shown in Figure 1. Figure 2 shows Chile’s map and the respondents’ distribution according to the region where they worked. The Metropolitan region was the one with the most significant number of participants; followed by the Valparaíso and Biobío regions. Next in terms of the number of participants was the Araucanía region.

Distribution of the respondents according to the city of residence in Chile.

Distribution of the respondents according to the region of work in Chile.
Regarding the medical specialty in which the study participants worked, 34.6% (n = 142) were general practitioners, 9.8% (n = 40) were specialists in internal medicine, 6.8% (n = 28) were pediatricians, 5.6% (n = 23) anesthesiologists, 4.4% (n = 17) were ophthalmology, 3.9% (n = 15) were family medicine, 3.6% (n = 14) were dermatology and the rest other specialties like neurology, surgery, cardiology, psychiatry, etc.
The years of professional practice were also investigated, finding that 39.3% (n = 161) of the physicians had more than 20 years of experience, followed by 18.3% (n = 75) who had more than 10 years of experience, but less than 15. Also, 16.6% (n = 68) had more than 5 years of work, but less than 10; and 15.9% (n = 65) had less than 5 years of professional experience, and finally, 10% (n = 41) had more than 15 years of professional experience but less than 20 years. The most frequent graduation country was Chile in 68.5% (n = 281), Colombia in 16.3% (n = 67), Venezuela in 5.6% (n = 23), Cuba in 4.6% (n = 19), Argentina in 3.9% (n = 16), and Bolivia and Mexico in 0.5% (n = 2) of the cases.
Respondents were asked for their views on physician-assisted suicide, finding what 39.5% (n = 162) agreeing strongly, and 21.5% (n = 88) was strongly disagreed. Regarding the point of view on euthanasia, 56.3% (n = 231) strongly agreed with this practice, and 13.9% (n = 57) strongly disagreed with this practice. Participants were asked whether people should be able to freely decide their death, finding that 53.4% (n = 219) strongly agreed with this judgment, while 20% (n = 82) agreed, and 8.5% (n = 35) strongly disagreed (Table 2).
Frequencies and Percentages Based on the Answers to the Different Scale Questions of Attitudes Toward Euthanasia and Physician-Assisted Suicide.
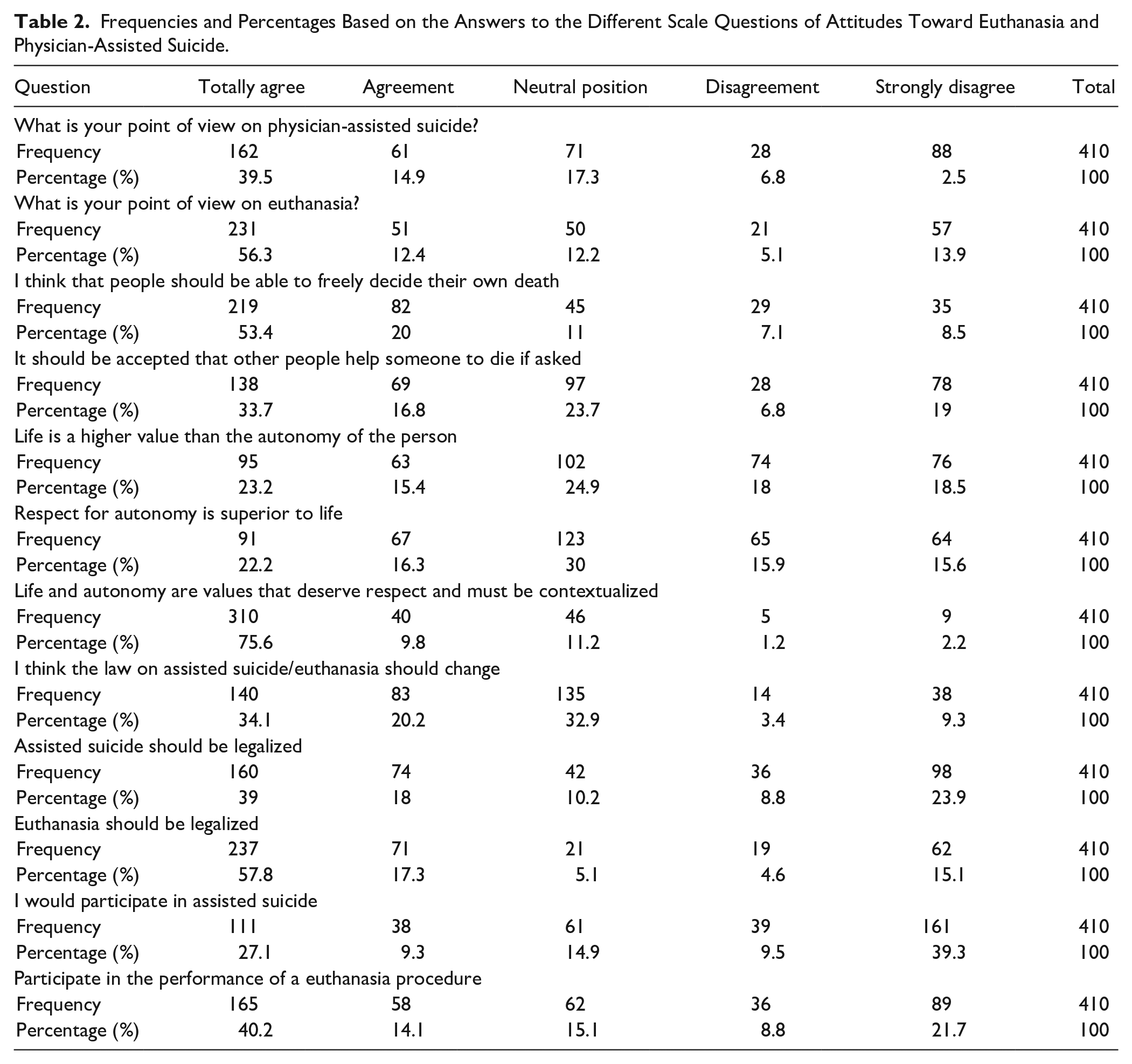
When asked if it should be accepted for other people to help someone die if asked, 33.7% (n = 138) strongly agreed, 23.7% (n = 97) had neutral attitudes, and 19% (n = 78) strongly disagreed. Life is a higher value than the autonomy of the person, it was an affirmation with which 23.2% (n = 95) strongly agreed, 24.9% (n = 102) had neutral attitudes, and 18.5% (n = 76) strongly disagreed.
In contrast, the thought that respect for autonomy is superior to life was reported as strongly agree by 22.2% (n = 91) of the respondents, an attitude neutral in 30% (n = 123) of the subjects, disagree in 15.9% (n = 65) and strongly disagree in 15.6% (n = 64). They were asked if life and autonomy are values that deserve respect and have to be contextualized; Given this, 75.6% (n = 310) strongly agreed and 11.2% (n = 46) had neutral attitudes.
When inquiring about whether the research participants knew the current law on assisted suicide and euthanasia in Chile, 53.4% (n = 219) mentioned not knowing it, while the remaining 46.6% (n = 191) did know the current law in this regard. Regarding whether they considered that the law on assisted suicide/euthanasia should change, 34.1% (n = 140) strongly agreed that the law should change, 32.9% (n = 135) had neutral opinions, 9.3% (n = 38) strongly disagreed. When asked if assisted suicide should be legalized, 39% (n = 160) strongly agreed, and 23.9% (n = 98) strongly disagree. Similarly, when asking whether euthanasia should be legalized, 57.8% (n = 237) strongly agreed and 15.1% (n = 62) strongly disagreed.
Finally, the participants were asked if they would participate in an assisted suicide or the performance of a euthanasia procedure, obtaining that for the first event, 27.1% (n = 111) would strongly agree with the practice and 39.3% (n = 161) strongly disagreed. On the other hand, in the case of participation in euthanasia, 40.2% (n = 165) stated that they strongly agreed with the involvement in this procedure, and 21.7% (n = 89) strongly disagreed (Table 2).
Some statistical associations were made, although they are not considered causal due to the type of work that was carried out. In that sense, regarding the point of view on euthanasia and the possibility of participating in a procedure of this type; the correlation was significant with a P ≤ .05. Also. When asking the participants about their point of view on assisted suicide and the possibility of participating in one, the correlation between these 2 variables was significant with a P ≤ .05.
Discussion
This study analyzed the information provided by physicians working in Chile about their opinions and attitudes about euthanasia and physician-assisted suicide. These professionals are characterized by having an approach to the phenomenon of care at the end of life and are exposed to requests from patients and family members to provide support in the terminal phase of diseases. 14 The presence of an attitude in favor of euthanasia and medically assisted suicide stands out; also, the value of the autonomy of people to think and decide about their own death. The majority of those surveyed stated that euthanasia should be legalized in the country.
In this order of ideas, the age of the doctors and the years of experience are essential variables to consider since opinions can vary between a recently graduated doctor and another with skills and knowledge acquired on the subject of end-of-life care throughout his professional career. In this study, the median age was 42 years, with the youngest participant being 25 years old and the oldest being 70 years old. Similarly, this research had a diversity of participating physicians whose years of professional practice varied from those with less than 5 years of work to participants who had more than 20 years of experience, the latter being the most representative group of the sample.
Similar studies were carried out in other Latin American countries like Brazil, where euthanasia is also not legal. They sought to identify the attitude of professionals and students toward assisted suicide and euthanasia, founding that, among those surveyed in his study, 68.1% favored the legal approval of assisted suicide and 73.2% favored euthanasia, in the case of patients with terminal pathologies. 3 This study also addressed the attitude in certain diseases, determining that the participants approved assisted death for people with neurodegenerative diseases in 46.9% and 30.8% for individuals with quadriplegia. 3 Del Río and Marván, 15 in 2011, conducted a study to examine the psychological meaning and attitudes toward euthanasia in Mexican individuals who had any relationship with the health area (students or already graduated doctors). Participants were divided into 3 groups: beginning students, advanced students, and practicing physicians. These authors found that positive psychological meanings, as well as positive attitudes, were more frequent among advanced students and already graduated doctors, who defined euthanasia with words such as “relief, calm, respectable, ethical, and dignified.”
In contrast, ambivalent attitudes prevailed in the group of beginning students. 15 Based on these results, it could be considered that opinions and behaviors regarding euthanasia may vary according to the knowledge of the subject, which highlights the influence that cognition and work experience in the field of health has on the response given in this type of survey. For this reason, to ensure that doctors have the knowledge and skills that they will increasingly need to deal with a request for assisted death, the inclusion of intensive care and treatment courses at the end of life is necessary for training programs, including training in bioethical aspects. 16
On the other hand, most of the participants in this study expressed that they strongly agreed (56.3%) or agreed (12.4%) when asked about their opinion regarding Euthanasia. These results show that the doctors consulted have positive attitudes toward these events. This is similar to what was experienced in countries such as Belgium and the Netherlands, where assisted dying was practiced with considerable frequency even when these interventions were not technically legalized, possibly because; for example, in Belgium, the criminal code has never Assisted suicide is sanctioned if it is done for philanthropic purposes and to help a suffering patient.16-18 Recent studies that have investigated attitudes toward these procedures have also revealed the growing acceptance of these practices in countries where euthanasia and assisted suicide are legalized and those that are not. Among these studies is the work carried out by Torres et al 19 where it was revealed that 65.7% of those surveyed considered euthanasia to be an acceptable practice, and the study by McCarthy and Seal 20 carried out among doctors in training in Canada, where the authors found that almost 60% of the respondents stated that they would perform medical assistance to die in their patients if they suffered from a terminal illness. Likewise, these procedures have not only been proposed to end the life of terminally ill patients with intolerable suffering; but also, for patients with neurological disorders such as advanced dementia, in which patients lose connection with the environment and may end up dependent conditions at a level that they cannot survive without specialized help.21,22
A probable explanation for the fact that a health professional who is dedicated to caring approves the idea of assisted death could be the more significant attribution given to the value of autonomy. And especially to what is related to each person’s decision-making power on relevant aspects of his life, such as the right to receive or refuse treatment according to his convictions and internal needs. But above all, the right to decide under what conditions die, especially if this act can reduce the suffering of painful disease.3,13 Based on the above, the theory has been postulated that, just as autonomy is part of the person’s daily life by being present when a decision is made or in the ability to forge their future, it should also be respected in the final chapter of life; since it is incoherent that it allows a person the freedom to do what they want during their life (as long as it does not harm third parties) and not to decide about their suffering and death, especially in the ambit of terminal illnesses.13,23
In this way, taking into account what was mentioned above, it was observed that 73.3% of the doctors surveyed in this study believed that people should be able to decide on their death freely, and 85.4% that life and autonomy are values that deserve respect and have to be contextualized. In addition, when the participants were asked if these behaviors should be legalized in the country (referring to assisted suicide and euthanasia), it was observed that a total of 237 people strongly agreed (57.8%) and 71 people (17.3%) agreed with the legalization of euthanasia, and 234 people (57%) also had a favorable opinion regarding the legalization of assisted suicide. In both cases, more participants agreed with legalization than those who disagreed or strongly disagreed with the practice of these procedures. The results of this research are similar to those obtained in the study carried out by Brandalise et al 3 which had already been mentioned previously; where the 68.1% of those surveyed agreed with the legalization of medically assisted suicide and 73.2% with the legalization of euthanasia for terminal patients, which shows that the majority was also in favor of this action. The study by Rodríguez-Calvo et al 13 also indicated a positive attitude toward these practices, as well as toward their legalization.
However, it was also observed that if euthanasia and assisted suicide were legalized in Chile, more doctors would not participate in medically assisted suicide than those who would, although the opposite happens in the case of euthanasia. These results are comparable with those obtained in other studies where it was observed that, although there is a favorable response regarding the acceptance of requests for assisted death and its legalization, fewer would be willing to participate actively in these practices.3,13,24,25
Similarly, the percentage of participating physicians who did not have a reasonable opinion regarding the practice of these procedures should be taken into account, which, although they were not the majority, had a high percentage and this may be associated with the fact that the physicians and health professionals are the ones who ultimately face patient requests for assisted death and religious convictions, political or moral conflicts enter into debate, since the term euthanasia in the past was has been related to indiscriminate death, eugenics, and murder,26,33 like what happened during the Nazi experiments and this situation has permeated the population to the present day. In addition, religious institutions of significant influence are categorical in strongly opposing these practices, as they have let it be known through documents such as the “Samaritanus bonus letter”; where she is more motivated toward palliative care in terminal illness and categorically condemns the idea of euthanasia.9,15,26
Within the limitations of this work is the size of the population since, although the sample in numbers was representative of the universe studied, the sampling was by intention and the dissemination was done through social networks, leaving many doctors who do not use social networks without the opportunity to express their opinions in this work. In addition, a greater participation would have allowed a better approximation to the phenomenon studied. Another limitation was the low participation of professionals from remote regions of the country because, although a massive campaign was attempted through social networks to publicize the study, there were few participants in peripheral cities, and the bulk of the participants focused on the country’s capital.
Some of the explanations for these results could be the influence of social and professional movements on human rights, liberal and progressive proposals, which influence the sustainability of traditionalist dogmas. Many of the physicians studied were young, and they tend to share these ideals. Likewise, many medical schools and the growing emergence of evidence on the subject have been able to modify previous beliefs. It is necessary to continue with this type of work that leads to knowledge and socialization of the broad scope of euthanasia and physician-assisted suicide, especially in the current context where discussions are taking place in governments that will lead to decisions regarding the legalization of these procedures. It is fair that physicians offer their point of view on this topic, and these professionals must receive education on care’s legal, ethical, and social aspects.27-29 It is important to motivate more authors to develop works in this sense and to know why doctors agree or disagree with euthanasia and assisted suicide to allow further reflection on the matter.
Conclusions
There was evidence of support for the implementation and legalization of euthanasia and assisted suicide by physicians in Chile. However, there are still professionals who have not yet decided on a definitive position on these practices.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
The statement that accompanied the link consisted of an informed consent that was prepared following the guidelines and recommendations of the European University of the Atlantic research ethics committee, which was the body that approved this research as recorded in the act CE-55 of March 5, 2021.