
Abstract
Background:
Skepticism among the public surrounding the COVID-19 vaccine is still prevalent despite vaccine-positive communication and many Americans having already received the vaccine. Side effects of the vaccine, as well as its expeditious research and development, are among the top concerns among those hesitant to receive the coronavirus vaccine. Moreover, there is additional concern regarding the association between comorbidities and severity of illness due to the coronavirus pandemic.
Objective:
We aimed to describe the pandemic- and vaccine-related concerns of South Texas residents who attended the UT Health San Antonio School of Nursing’s vaccine clinic with the goal of better understanding vaccine-related misconceptions and hesitancy for subsequent vaccination campaigns and boosters.
Methods:
An electronic survey accessible via a QR code on printed flyers was distributed throughout the waiting areas and post-vaccine observation rooms within the COVID-19 vaccine clinic at UT Health San Antonio School of Nursing from April 5 to 16, 2021. The survey contained a primary open-ended question designed to obtain information on concerns of the clinic attendees regarding the COVID-19 pandemic and COVID-19 vaccine. A thematic analysis was performed on the qualitative data to identify major themes to better understand concerns of vaccine clinic visitors.
Results:
During the 11-day period, 510 attendees received vaccinations through the vaccination clinic and completed the survey. Five areas of concern were identified by the 277 attendees: immunity, future vaccinations, vaccine symptoms and safety, protocol post-vaccination, and child vaccinations. Post-hoc sentiment analysis showed that responses were generally neutral or negative.
Conclusion:
This study provides a perspective regarding questions and concerns of South Texas residents regarding the COVID-19 pandemic, the vaccine, and their general health status within a vaccinated population. Vaccine recipients were found to still have questions even after receiving the vaccine, suggesting that eliminating uncertainty surrounding the COVID-19 vaccine is not necessary to motivate individuals to receive the vaccine. Instead, addressing concerns through public health messaging could be a useful strategy to address vaccine-related concerns and increase subsequent vaccine uptake in future vaccination campaigns and boosters.
Introduction
In December 2020, vaccinations for the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2 or COVID-19) gradually became publicly available. As more people became qualified to receive the vaccine, national, state, and local healthcare agencies had to combat skepticism people held about the Food and Drug Administration’s (FDA) emergency approval of the vaccine, the benefit of the vaccine, and the impact it would have on their lives. 1 Concerns about side effects and the rapid nature of vaccine development top the list of reasons cited by those who plan not to receive the coronavirus vaccine. 1 In order to decrease vaccine hesitancy, it is important to create modalities that uniquely target specific populations. 2
An area of concern during the pandemic has been the association between risk factors, such as sedentary lifestyle and unhealthy diets, and comorbidities, such as obesity and hypertension, to the severity of illness in individuals infected with COVID-19. The most common comorbidities of patients hospitalized with COVID-19 have been hypertension, obesity, chronic lung disease, diabetes, and cardiovascular disease and associated with increased intensive care unit (ICU) admissions and mortality rates. 3 Additionally, more than 75% of the US population do not meet recommended standards of physical activity, putting them at greater risk of developing co-morbidities and adverse outcomes related to COVID-19 infection. 4 Furthermore, a recent survey by our group summarized the pandemic had negatively impacted the psychological well-being of respondents, potentially impacting vaccination rates in our community. 5
As of January 25th, 2022, over 76% of Americans have received at least one dose of the vaccine, over 63% of Americans have received both doses of the vaccine, and 25% have received both doses and the vaccine booster. 6 Vaccine hesitancy remains a prevalent issue, with an estimated 5% to 33% of people across counties nationwide expressing hesitancy or uncertainty about receiving the COVID-19 vaccine. 7 In Bexar County specifically, 15.87% of the population remains hesitant or unsure about getting vaccinated, while 6.41% remain strongly hesitant. 7 Among vaccine hesitant adults, healthcare attitudes, political partisanship, and other demographic characteristics have been associated with willingness to receive a vaccination. 8 After controlling for demographic variables, a recent publication found that people high in agreeableness, conscientiousness, and emotional stability were more likely to regard vaccination in a positive perspective, showing that personality plays a significant role in an individual’s vaccine hesitancy. 9 This implies even those who chose to get vaccinated may be doing so based on social predilections and may still not be fully informed on the vaccine. Thus, to better understand strategies to increase US vaccination rates, it is also important to understand the concerns and questions of vaccinated individuals, an often-overlooked population.
To better develop resources that demonstrate the benefits of the vaccination for future vaccine campaigns and boosters, it is important to first understand the concerns of individuals who have taken the vaccine. Therefore, the primary purpose of this study was to ascertain concerns of vaccine clinic attendees regarding the COVID-19 pandemic and the COVID-19 vaccine. In order to do this, we conducted a qualitative cross-sectional study to understand the questions and concerns that San Antonio residents have about the COVID-19 pandemic and vaccine after receiving the vaccine. Knowledge of vaccine-related concerns will serve to aid future public health campaigns that counter vaccine hesitancy and address vaccine-related health concerns.
Methods
Study Design
This study was approved by the University of Texas (UT) Health San Antonio Institutional Review Board as not regulated research. This was a cross-sectional study with a qualitative study design. We applied the basic components of a phenomenological research design in creating this study, investigating perceptions and pre-conceived assumptions regarding the COVID-19 vaccine. Consolidated criteria for reporting qualitative (COREQ) research guidelines were followed. The study was conducted over a 12-day period from April 5 to April 16, 2021, through an anonymous online survey. 10
Survey Development and Distribution
The survey was designed by UT Health San Antonio medical students and faculty with consideration to the clinical setting of the vaccine clinic in which it would be administered. To maximize engagement, the survey was kept succinct as it was designed to be answered by participants during the post-vaccination observation period. Furthermore, the survey was also provided in Spanish to accommodate the large Spanish-speaking population in Bexar County. The survey specifically gathered information regarding patient concerns about the COVID-19 vaccine and pandemic. Only one question pertinent to addressing the objective of the study was included in the survey. Questions regarding demographics and other personal information were omitted to ensure respondents thoroughly expressed their thoughts when answering the key questions of the survey. Open-ended responses for the following question was collected:
Having received your vaccination, what questions do you have today about the vaccine and life after the vaccine?
The survey was administered electronically and accessible through printed flyers with quick response (QR) codes. The flyer contained a short message affirming the decision of those who received the vaccine along with brief instructions regarding how to access the survey through the QR code.
Sampling, Data Collection, and Analysis
Respondents were recruited to complete the electronic survey using convenience sampling method of patients that came to the vaccine clinic located at the UT Health San Antonio School of Nursing. Flyers were distributed throughout waiting areas and observation rooms. At the time of data collection, only adults >18 years were eligible for vaccines. Visitors were not allowed, ensuring that only those receiving the vaccine were answering the survey. All data sets were received electronically and compiled electronically into Google Forms for qualitative content analysis. Thematic analysis was conducted by 3 qualified reviewers assessing each response and to classify under an identifying theme. Each reviewer assessed and classified each response separately prior to meeting and reviewing the responses collaboratively to finalize upon themes.
Data Analysis
A qualitative descriptive approach was used to analyze data collected from free-text entries in online surveys collected from anonymous respondents (n = 529 compared to n = 510 vaccine recipients, with a 3.7% rate in response duplication). 11 NVivo (QSR International Pty Ltd, 2020) was used to (a) code free-text survey entries, (b) organize the codes into interrelated themes, (c) assess codes and themes for sentiment, and (d) as a cross-check to confirm thematic relationships, perform code-based cluster analysis using NVivo-automated word similarity metrics. 12
Sentiment analysis
Sentiment scoring using standardized categorization (eg, no sentiment, moderately negative, very negative, moderately positive, very positive) was applied to the same codes used to generate themes and subthemes. Aggregate scoring of coding references by themes were then organized by scoring results by proportion of neutral, negative, and positive coding references.
Results
Concerns About the Vaccine
Of the 510 attendees who completed the survey, 277 attendees (54%) provided responses to the question regarding the vaccine and/or about life post-vaccination. The highest number of responses expressed patients’ questions about vaccine onset and length of time the vaccine provides immunity (n = 90; 32.1%) and whether additional boosters will be needed in the future (n = 74; 26.4%). Approximately a quarter of responses focused on concerns regarding side effects and/or vaccine safety (n = 73; 26%). The remaining concerns included what life was going to be like after vaccination and post-vaccination protocols (n = 41; 14.6%) and vaccinations for minors (n = 2; 0.7%) (Figure 1). Several themes regarding post-vaccination protocols and future vaccinations emerged from the responses. Acute reactions or symptoms were the primary concern regarding the side effects of the vaccine.
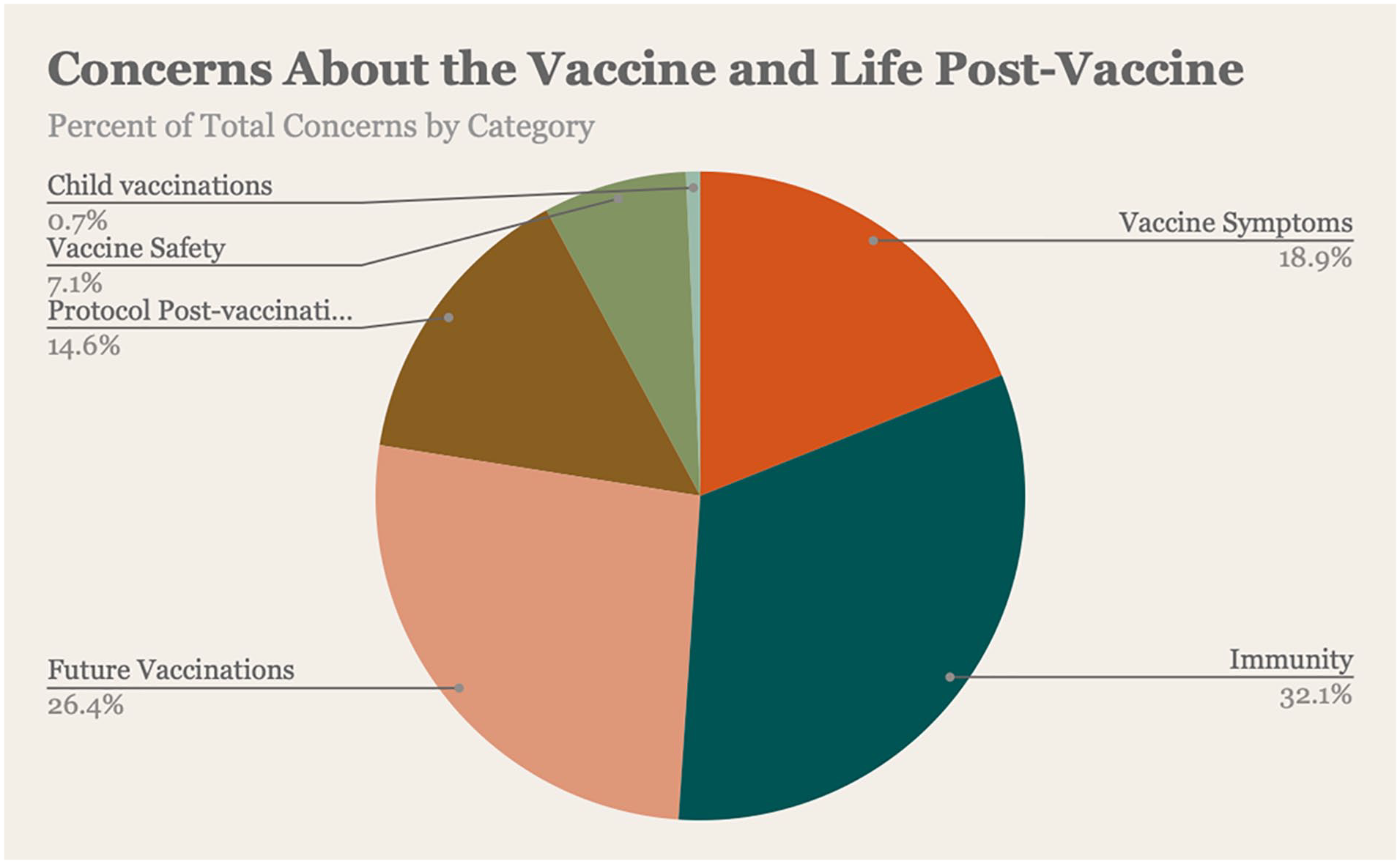
Concerns about the vaccine and life post-vaccine.
Themes
The following major themes and subthemes were generated from the coded data (Table 1).
Survey Themes and Subthemes.

“How effective is it?”/COVID-19 vaccine efficacy
The largest proportion of free-text entries and generated codes were related to questions about the efficacy of the COVID-19 vaccine, that is, onset (“how long after vaccinated is considered ‘fully vaccinated’?”), degree (“how protected am I from COVID after this?”), and duration (“how long will it be effective?”) of protection from COVID-19 infection. Closely tied to questions about vaccine efficacy were inquiries about the planned COVID-19 vaccination schedule (“how often will we have to take the vaccine?”) and post-vaccination COVID-19 infectivity (“si me contagio puedo infectar a otras personas”/if I am infected, can I infect other people). Several respondents asked if widespread vaccination would prompt a return to normal, pre-COVID-19 environment (“Will there be any quarantine necessary after the vaccine?”). One respondent stated:
I’m curious about the future. I know there aren’t answers. I think it will be interesting to see how long this goes on as the virus continues to mutate.
“How will it affect me now and in the future?”/COVID-19 post-vaccination concerns
Post-vaccination concerns centered on 3 distinct categories: vaccine-related symptoms and symptom management, vaccine-related long-term side effects, and access to vaccine-related follow-up information. Several respondents asked about symptom management strategies (“What can I take if I feel sick? What do I do if I have an allergic reaction?”), with many also wondering if they could expect similar or worse symptoms compared to their first dose (“I had terrible side effects from my first shot. . .a 104 [degree] fever. Will the second be the same?”). Most often, respondents asked for information about long-term side effects associated with the COVID-19 vaccine (“What are some side effects that may occur months to years following full vaccination?”). Some respondents asked specifically for manufacturer contact information (“would like a contact number . . . for specific questions”). One respondent commented:
Is there an open forum for those who have been vaccinated with Pfizer, etc. Later down the line, what if we have questions?
“How do you get rid of the ambiguity?”/Unclear or conflicting COVID-19 guidance
Several respondents commented that unclear or conflicting guidance about COVID-19 and related restrictions were problematic. One respondent stated:
I don’t trust the news because it will say one day that you can go without a mask after vaccination, but then it’ll say that we aren’t safe. Is there a guideline that doctors will have that doesn’t go back and forth?
Related to mask use, respondents typically asked how the COVID-19 vaccine might impact personal actions (“Do I still need to use a mask?”) or government regulations (“would masks still be enforced?”). This mirrored other respondent requests for guidance on social distancing post-vaccination. One respondent asked, “When is it ok to gather socially with others and what does that interaction look like?” while another asked, “Will there be any quarantine necessary after the vaccine?” A few respondents wanted instructions regarding their vaccination card (“Do we need to hold onto our vaccine records permanently?”) out of concern about future travel (“Are we going to have to travel with our covid [sic] vaccination card?”)
Finally, several respondents expressed concern that while they now were vaccinated, their children were not. “How are unvaccinated youth affected?” asked one respondent, while another commented, “Will school teachers get the vaccine?” These respondents all asked, “When will the vaccine be available for children?”
“This has certainly heightened the awareness of my own health”/Health status during COVID-19 period
Several respondents indicated that their chronic illness (most self-reported a history of diabetes, hypertension, or obesity) was exacerbated by social isolation resulting from COVID-19 related social distancing mandates and fear of COVID-19 infection. One respondent shared:
I have gained over 20 pounds just from staying home over the last year and not working and not being as active in general as I was before so my hypertension has gotten worse and I am at risk for heart disease and diabetes. I am very concerned about my physical health but not sure how to fix it.
Some respondents also shared that they had new health concerns related to family health history (“I’ve worked out much less since the start of COVID and diabetes runs in my family so I’m nervous that I will develop it”). Of note, the 3 most commonly reported new health concerns were decreased physical activity (“impact of a mostly sedentary lifestyle for the past year”), weight gain (“just need to lose that COVID 15 pounds!”) and mental health (“depression, anxiety and burnout”). All respondents identified COVID-19-related social isolation as the main reason for their decline in health status. One respondent commented:
Lack of going out from quarantining has me worrying about Vitamin D deficiencies, worsen [sic] mental health, and I’m developing near-sightedness. I feel symptoms of all of the above.
“I am still terrified of this virus”/Fear of COVID-19 infection
For some respondents, receiving the vaccine did not alleviate their concerns. One respondent stated, “I am still terrified of this virus,” while another reported “delaying general health appointments due to not wanting to be exposed [to COVID-19].” Several admitted they were “still cautious” and “got used to quarantining . . . [so] I am a bit nervous about a return [to normal].” A few respondents shared that they had already had COVID-19 and were concerned about related long-term sequelae (“side effects for those with long Covid [sic]”). A respondent wondered “how badly I have been damaged by Covid and long Covid [sic] as I am unable to afford a doctor.”
Sentiment Analysis
The theme fear of COVID-19 infection had the highest proportion of negative responses, while COVID-19 vaccine efficacy had the highest proportion of neutral responses, and customer service feedback had the highest proportion of positive responses (Table 2).
Sentiment Analysis by Theme.


Cluster analysis
As a cross-check to confirm thematic relationships, cluster analysis of codes associated with themes and sentiment was performed using Pearson’s correlation coefficient as a word similarity metric, which NVivo (QSR International Pty Ltd, 2020) then uses to generate word dendrograms. 12 Figure 2 depicts degree of similarity between themes; the closer themes are collocated, the higher the proportion of similar words and similar sentiment between them.

Cluster analysis of themes based on word similarity.
The generated clusters reflect thematic relationships that centered on COVID-19 guidance pre- and post-vaccination, vaccine administration, short- and long-term vaccine side effects, and the impact of COVID-19 on health status. Of note, some coding for the theme of customer service feedback (“Happy to get vaccinated”) was associated with themes reflecting self-management of health, whether self-protection from COVID-19 infection or management of preexisting or new health concerns.
Discussion
The results of this study suggest vaccine recipients are concerned about vaccine efficacy and post-vaccine life, the potential for future vaccinations, vaccine safety and vaccine symptoms, both chronic and acute. Furthermore, several comments from respondents indicate that even after receiving the vaccine, the possibility of COVID-19 infection remains a source of distress within the vaccinated population. In addition, the survey results indicate significant confusion regarding the impact of the vaccine on an individual and populational level, as well as the protocols followed after getting vaccinated. These findings revealed that many of the concerns among those who receive the vaccine are significant enough to be addressed in the context of future vaccination campaigns and boosters. 13 Thus far, public health campaigns from local healthcare agencies, targeted outreach to specific sub-populations, and canvassing by community health workers have been beneficial in addressing vaccine hesitancy and can be further utilized to promote boosters.
The COVID-19 pandemic has been unprecedented in terms of its vast impacts to both individuals and societies worldwide. The uncertainty surrounding the pandemic was only magnified with the rapid approval of the COVID-19 vaccine. As a result, many people in the US and abroad have voiced their skepticism about the efficacy and safety of the vaccines and remain unvaccinated. 1 It is crucial to utilize all resources available to gain a better understanding of the factors contributing to the vaccine hesitancy that remains among Americans. Considering the perspectives of those who received the COVID-19 vaccine is instrumental in clearing misconceptions and vaccine hesitancy, while providing valuable public health messaging regarding the importance and significance of healthy living during the COVID-19 pandemic.
Addressing vaccine concerns is especially important within low-income communities. COVID-19 infections rates are disproportionately affecting individuals from low socioeconomic status and underserved populations.14,15 Karmakar et al 16 found an increase of 0.1 points in social vulnerability index score to be associated with a 14.3% increase in COVID-19 incidence rate. Low wage workers were especially affected, as more precarious employment and economic conditions, such as variable income, lack of paid sick leave, and food insecurity forced this population to continue working and acted as barriers toward adopting COVID-19 mitigation measures. 17 Disparities in socioeconomic status are also reflected in the prevalence of co-morbidities. Those making less than $25 000 a year had a diabetes rate of 27.2%, compared to a rate of 8.1% for those earning over $50 000 a year. 18
With many COVID-19 vaccine makers planning for annual boosters, interventions that utilize the results of this study will be increasingly paramount in order to attenuate any vaccine-related concerns or hesitancy. 19 A study of predictors of uncertainty to receive future COVID-19 booster vaccines shows that the strongest predictor of hesitancy is previous uncertainty and unwillingness. 20 The population at greatest risk of exhibiting these traits were found to be low-wage workers and those from lower socioeconomic background. 20 Thus, it is increasingly important to address concerns with vaccination programs and general vaccine hesitancy at an early stage in order to ensure successful participation in future vaccine booster programs.
Despite the beneficial data discovered in this qualitative study, this study is not without limitations. Limitations within this study are related to the nature and timing of data collection. Firstly, the survey could only be accessed through a QR code, thus, a considerable number of people attending the clinic either did not know how to use the QR code or did not have a phone with the capability of scanning QR codes. This reduced the responses that were received and may have discouraged older individuals who may not have been familiar with this technology from participating. To account for this, the authors volunteered at the vaccine clinic and assisted participants who had any technical issues with accessing the survey using the QR code throughout the data collection period. Additionally, the data collection period was just short of 2 weeks long, lasting from April 5 to 16, 2021. Secondly, given that different groups were eligible to receive the vaccine at different time periods within the last 6 months, the data collected may not be generalizable to the general population. Thirdly, the survey was anonymous and did not collect demographic information, which further complicates our understanding of who engaged with the survey, had questions, and how to apply it to the population. Due to the urgency of the COVID-19 pandemic and to get as many participants to take the survey as quickly and feasibly as possible, we restricted the survey to a small number of questions that focused on the most relevant information to help gain a more informed understanding of what lay people felt confused about with regards to the virus and vaccine. Furthermore, data was collected from participants during a short waiting period of their vaccination process. For these reasons, we consciously chose not to collect information from the participants about their race, gender, and socioeconomic status. This maximized retention, ensuring that the survey wasn’t too long as to deter people from participation.
Conclusion
Given the growing polarization regarding healthcare during the pandemic, it is important to explore concerns regarding COVID-19 vaccinations that exist in the population. This study is the first to examine the attitudes and concerns of individuals who received the COVID-19 vaccine. It was found that individuals who received the vaccine at the UT Health San Antonio School of Nursing vaccine clinic had questions regarding the length of immunity offered by the COVID-19 vaccine, the need for future vaccinations, and side effects after having taken the vaccine. The results of our study provide insight into messaging that can be used to boost vaccine uptake if the need arises in the future, in the form of subsequent vaccination campaigns or boosters. Future studies should be conducted in order to investigate effective messaging campaigns to decrease vaccine hesitancy, increasing vaccine uptake, and promote healthy lifestyles that reduce the frequency and development of co-morbidities during the pandemic.
Footnotes
Authors’ Contributions
Hari Krishnakumar BS conceptualized the study and led the data collection, formal data analysis, and manuscript writing. Gretchel A. Gealogo PhD RN conducted formal data analysis and revised the work to add critically important intellectual content. Taylor Holland BS assisted with data collection and manuscript writing. Monica Martinez BS assisted with data collection and manuscript writing. Lucas Hendrix BS assisted with data collection and manuscript writing. Michael Collins BS assisted with formal data analysis and manuscript writing. Melissa Donate BS assisted with manuscript writing. Maryann England BS assisted with data collection and formal data analysis. Eric Kumana BS assisted with formal data analysis. Joshua Garcia BS assisted with formal data analysis. Andrew Wilkey BS assisted with formal data analysis. Niklesh Akula BS assisted with formal data analysis. Ashley Mai BS assisted with data collection. Darpan I Patel PhD conceptualized and supervised the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by a Community Service-Learning Grant from the Center for Medical Humanities and Ethics in the School of Medicine at The University of Texas Health Science Center at San Antonio.
Ethics Approval
This study was approved by the UT Health San Antonio Institutional Review Board as not regulated research.
Consent to Participate
N/A
Consent for Publication
N/A
Availability of Data and Material
N/A
Code Availability
NVivo