
Abstract
Background:
Early detection, treatment, and care are important for the prevention of dementia. Though olfactory impairment has been reported to be associated with mild cognitive impairment (MCI), there are few reports involving community-dwelling older adults with no difficulty in daily life in Japan.
Objective:
This study aimed to identify the frequency of MCI in community-dwelling elderly people attending community salons in a city with a high aging population, and to determine the usefulness of a pocket olfactory discrimination test.
Methods:
We recruited 268 independent older adults attending community salons. The Japanese version of the MCI Screen was used to evaluate cognitive function, defining MCI as <49.8 out of 100 scores of the memory performance index (MPI). The Japanese version of the University of Pennsylvania Smell Identification Test (UPSIT-J) was used for olfactory discrimination and the number of correct answers out of 4 questions was noted.
Results:
Of the salon participants, 138 (51.5%) were classified as having MCI. As the number of correct answers on the olfactory test decreased, the percentage of participants with MCI increased. The MPI score of the low UPSIT score group was significantly lower than that of the high UPSIT score group.
Conclusions:
This study revealed that approximately half of the elderly local residents living without daily problems were suspected of having MCI. The UPSIT-J-4 is a simple olfactory identification test, and can be used at any time and any place. It is useful for screening cognitive function via olfactory identification in a salon-like setting.
Introduction
The elderly population is growing dramatically worldwide, and the accompanying increase in the number of people with dementia has become a major health care issue. According to An Ageing World 2015, 1 the percentage of people aged ≥65 years worldwide was 8.5% in 2015, but is expected to increase to 12% in 2030, and 17% in 2050. In Japan, the population is aging more rapidly than in any other country in the world, the dementia population is estimated to reach 7 million, and the percentage of people aged ≥65 years 38.8% by the year 2025. 2 Given the increasing dementia burden, it is important to detect dementia in its early stages and to slow its progression. Mild cognitive impairment (MCI) is a transitional state of cognition between normal aging and dementia that may progress to dementia. 3 MCI is defined by subjective or objective evidence of cognitive decline that is greater than expected for age and education level but does not significantly interfere with daily living. 4 Several studies have indicated that these individuals are at an increased risk for developing Alzheimer’s disease (AD) ranging from 10% to 15% per year.5,6 On the other hand, a meta-analysis has shown that 4% to 24% of MCI patients recover to normal with subsequent follow-up.5 -7 Specific lifestyle activities, such as attending community meetings, participating in hobbies or sports activities, and efforts to lower blood pressure, are associated with reversion from MCI to normal cognition.8,9 Continued productive activity has been shown to help maintain MCI status, even if it does not return to normal. 10 Given that MCI is a reversible or progression-preventable condition, early MCI detection is important to avert progression to dementia; therefore, community-wide approaches are becoming increasingly important for early detection of MCI.
A systematic review published in 2012 reported a prevalence of MCI ranging from 0.5% to 42% in different countries and populations. 11 Different diagnostic confirmation tools will yield different results in MCI prevalence. In addition, factors that influence the prevalence of MCI include age, gender, years of education, and economic status.12,13 It has also been shown that the prevalence of cognitive impairment is higher in the rural area relative to urban areas. 14
The screening test for detecting MCI in community-dwelling older adults should be as simple and timesaving as possible in the absence of specialized staff. It is well known that olfactory dysfunction is present in symptomatic AD,15,16 but recent studies have shown that olfactory dysfunction can be detected in the very early stages of AD as well as in MCI.17,18 Furthermore, olfactory impairment may predict future cognitive decline among cognitively normal adults.19,20 There are 4 types of olfactory function: odor identification, odor discrimination, odor detection thresholds, and odor memory. Odor identification is likely the most impaired in MCI. 18 In this regard, the olfactory test is a simple and inexpensive method. Therefore, it has been suggested that assessment of olfactory identification ability may be useful as a screening test for MCI in elderly persons living in the community.16,21,22
Bungotakada City is located in the northern part of Oita Prefecture, Japan. It has 22 000 residents, of whom 38.9% (8500) are aged ≥65 years. Here, elderly people who have no difficulties in their daily lives gather voluntarily in salons. The Salons are places where community residents gather spontaneously to engage in health and cognitive activities. The city has over 100 salons and in April 2018, Bungotakada City and the City Medical Association, in collaboration with Oita University, launched the “Research Project for Creating a Community Living with Dementia.” Through this project, various efforts are made at salons to maintain cognitive function, and the usefulness of these efforts is being evaluated. In addition, cognitive function and olfactory tests are conducted as screening methods, with the aim of detecting elderly people suspected of having dementia at an early stage and connecting them with specialized institutions. Data from this project were used in the present study.
The aims of this study were to identify the frequency of MCI in community-dwelling elderly people attending community salons in a city with an aging population and to determine the usefulness of a pocket olfactory discrimination test.
Material and Methods
Participants
The salon targeted healthy elderly local residents who were self-reliant enough to gather a salon alone. The inclusion criteria were local residents who gathered at the salon and agreed to participate in the study. The exclusion criteria were those under treatment of cognitive impairments or certification of nursing care, or whose cognitive decline was noticeable by those around them. Those with obvious olfactory impairment due to nasal disease or head trauma.
Information on the demographics (age and gender), cognitive function, and smell identification test results were collected. Participant demographics are taken at the time of initial participation in the salon. Data were anonymized.
Informed Consent
First, city officials explained the study to salon representatives at a separate space in the large room. The representatives who agreed with the study signed a consent form. Next, city officials explained the study to the participants, who also signed a consent form.
Cognitive Function Test and Smell Identification Test
A Japanese version of the MCI Screen (J-MCIS) 23 developed by Medical Care Corporation was used for this cognitive function evaluation. The J-MCIS consists of an immediate recall task, a ternary comparison task, a judgment task, a delayed free recall task, a cued-recall task, and a rehearsed recall task, which is administered interactively using the Internet environment. The MCI Screen is a simplified scale for the assessment of cognitive function that has been approved by the United States Food and Drug Administration. The examination takes approximately 10 min to complete, and the questions differ for each section. A scoring algorithm is then used to calculate a memory performance index (MPI) score based on the patient’s test results, age, educational background, and race. The MPI quantifies the pattern of correctly recalled words from the Consortium to Establish a Registry for Alzheimer’s Disease wordlist on a scale from 0 to 100, which distinguishes normal from MCI with an accuracy rate of 96% to 97%. 24 The Japanese version has been shown to have negligible differences from the English version in both sensitivity and specificity, 23 with MPI scores of 49.8 or higher classified as the normal and those below 49.8 as the MCI. 22
Odor identification testing was performed with the Japanese version of the University of Pennsylvania Smell Identification Test (UPSIT). UPSIT is known for its accuracy in odor identification testing and is considered one of the most reliable tests. 25 It is composed of 4 microencapsulated odorants applied to the base paper and when the area where the odorants are applied is lightly rubbed with a cotton swab, the odorants are volatilized. As shown in Figure 1, if participants rub the left brown area with a cotton swab, they can smell the soap, but they must get their nose very close to it. The brown area is made to be as far away as possible, so the smell of the previous test does not interfere. Once one question is finished, they quickly move on to the next. This study used 4 Version B odors (soap, grape, onion, and rose). By selecting the name of the relevant odor from the 4 options, the test is conducted in about 3 min. The number of correct answers among the 4 odors was regarded as the score in the smell identification test (scores 0-4). Cognitive function and smell identification tests were paid for by Bungotakada City and no charges were incurred by the participants.

Japanese version pocket olfactory identification test. The correct odors are from left to right: (a) soap, (b) grape, (c) onion, and (d) rose.
Statistics
Statistical analyses were performed using StatFlex version 7.0 (Artec, Osaka, Japan), SPSS version 25 (SPSS Inc., Chicago, IL), and EZR version 1.37 software (Saitama Medical Center; Jichi Medical University, Saitama, Japan). Differences in groups were analyzed using Mann-Whitney U test and χ2 tests were used to analyze differences in categorical variables. The correlation between the number of correct answers of UPSIT-J-4 and the MPI score was assessed using Spearman’s rank correlation coefficient. The Cochran-Armitage test was used for trend testing. P-values less than .05 were considered statistically significant.
Results
Participant Characteristics
Figure 2 shows participants disposition. There were 272 people who attended the salon. Two of them had an olfactory impairment, so they could not perform the sniff test. Two were also excluded due to missing data. As a result, 268 participants were enrolled, of whom 70 (26.1%) were males, with an average age of 77.0 ± 6.7 years.

Participants disposition.
Cognitive Function Test
All participants underwent J-MCIS. The average MPI score was 46.4 ± 14.1. There were 137 participants who presented with an MPI score of <49.8 and 131 participants with an MPI score of ≥49.8. As a result, this study demonstrated MCI was suspected in 51.9% of those. The mean age of the participants suspected of having MCI was 81.1 ± 5.1 years, which was significantly higher than that of another group of 72.7 ± 5.3 years (P < .001).
UPSIT-J-4 Answers
As shown in Table 1, participants were divided into 2 groups based on the number of correct UPSIT-J-4 answers. The low score group was defined as those with 2 or less correct answers, and the high score group was defined as those with 3 or more correct answers. The low score group was 129 (48.1%), and the group with the higher score was 139 (51.9%) (Table 1). The mean age of the low score group was 78.4 ± 6.9 years, which was significantly higher than that of the normal group of 75.7 ± 6.3 years (P < .0003). The MPI score of the low score group was 43.0 ± 14.0, which was significantly lower than that of the high score group of 49.8 ± 13.4 (P < .0045). The proportion with decreased smell identification was not associated with gender.
Characteristics of Participants With Smell Identification Test (UPSIT-J).

Abbreviations: MPI, Memory Performance Index; UPSIT-J, Japanese version of the University of Pennsylvania smell identification test.
Low score group: UPSIT-J score ≤2.
High score group: UPSIT-J score ≥3.
The Mann-Whitney U test.
The Chi-square test.
Relationship Between Cognitive Function and Olfactory Impairment
Figure 3 shows the relationship between the number of correct answers in the UPSIT-J-4 olfactory test and the MPI scores from the J-MCIS. As the number of correct answers increased, the percentage of participants classified as normal group increased significantly (P < .001, Cochran-Armitage). Among participants with 0, 1, and 2 correct answers, 87.5%, 77.0%, and 62.8% were classified as MCI, respectively.
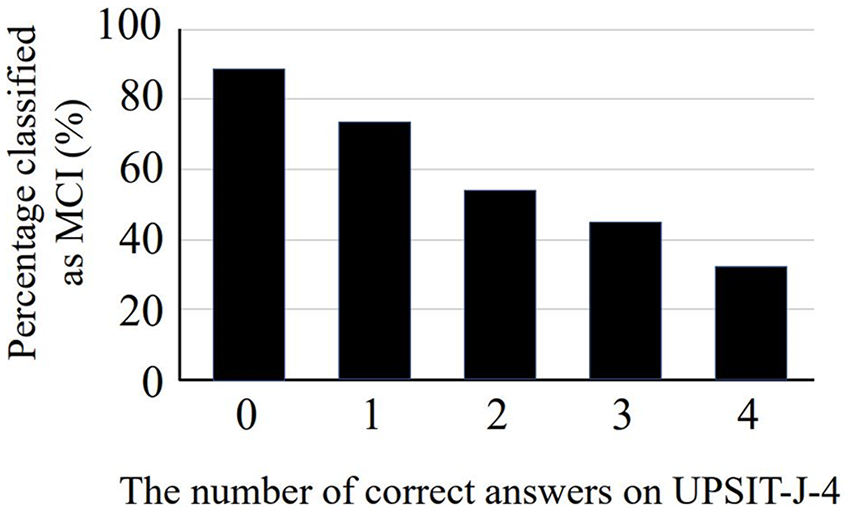
Correlation between the number of correct answers on Japanese version of the University of Pennsylvania Smell Identification Test (UPSIT-J) and ratio of mild cognitive impairment (MCI). MCI is defined as having memory performance index score of <49.8.
Discussion
This study showed that about a half of the salon participants were suspected to have possible MCI although they did not interfere with their daily lives and seemed to have no problems with their cognitive function. This suggests that MCI can be suspected even before those around them are aware of cognitive impairment. Therefore, it is crucial to develop simple methods leading to early detection and intervention, as well as to find appropriate places to implement them.
A recent study in Japan reported a 17.0% prevalence of MCI among the elderly aged ≥65 years living in 8 specified regions, and a 25.5% prevalence among those aged ≥75 years. 26 Compared to the studies described above, the percentage of MCI in the community-dwelling older adults in this study was extremely high. The prevalence of MCI varies considerably across countries, 27 and one of the reasons for this is thought to be differences in diagnostic confirmation tools. To screen for MCI, the J-MCIS is an excellent tool to use outside of a specialized medical institution because of its simplicity and self-assessment. It has been shown that the MPI score correlates with dementia severity and is 2 to 3 times more discriminative than traditional cognitive scoring methods. 24 In a recent study that screened participants in a health measurement event for cognitive decline using MPI scores, 57% had MPI scores of ≤49.8. 22 Our results are comparable to those of this study. Although not shown in the current study, most participants in the low MPI score group in this study who visited a specialized institution were diagnosed with MCI or dementia. This indicates that the J-MCIS is useful as a screening test for cognitive decline among community-dwelling elderly persons. Thus, a simple olfactory test that correlates with MPI score could be useful for screening of cognitive decline.
This study examined whether the olfactory identification test, UPSIT-J-4, could be used as a screening method for cognitive decline in community-dwelling older adults. As a result, among those tested, 48.1% of the elderly had ≤2 correct answers, and the lower the number of correct answers on the UPSIT-J-4, the greater the likelihood of having MCI. Nogi et al 22 reported that an olfactory discrimination test using UPSIT with 20 different odorants is a simple and useful tool for screening MCI. They showed that the difference in scores between the healthy group (median 13, range 7-18) and the cognitively impaired group (median 12, range 3-17) was significant. Our method is a further simplification of theirs. It is a very simple and quick test for olfactory identification ability using UPSIT-J-4 and has proven to be a feasible method for extracting MCI from the community-dwelling older adults.
The present study revealed that olfactory identification ability as well as cognitive function declined with increasing age. In a Japanese cohort of 1102 individuals, the mean score on UPSIT-J-4 was associated with an age-dependent decline in olfactory identification function. 28 On the other hand, unlike previous reports, no gender differences were found in olfactory identification ability in our study. This may be related to the fact that there were no gender differences in the MPI scores. Similarly, there are studies reporting insignificant sex difference in MCI, 29 or even higher prevalence of MCI in older adult males. 30
A unique aspect of our study was the use of salons as the location to administer a cognitive function test and an olfactory test to elderly residents of the community. This study is linked to the city’s health promotion plan. The salon serves as a social capital fostering site at the community level. The salons are run by local volunteers and receive financial and administrative support from the town office. They allow people to meet and interact with others through cooking, and physical and mental exercises. Previous studies showed that participation in a salon is associated with a 50% reduction in the incidence of needing nursing care and about a one-third reduction in the risk of developing dementia.31,32 Salons are open to all older adults, and a higher percentage of low-income residents than those of higher-income are reported to participate in salons, 33 suggesting that salon-type community interventions may reduce inequalities in social interactions. This study showed that salons, where the elderly congregate, are very suitable places for early screening of individuals with seemingly normal cognitive dysfunction. This may suggest that this study enabled the early detection of persons with cognitive decline and linked them to a specialized medical facility for detailed examination.
This study had several limitations. First, because this study was conducted among those who voluntarily participated in the salon, the sample size and the proportion of males were small. Given that gender differences were not significant in cognitive and olfactory impairment in this study, it is not considered to have affected the results. Second, classified into the MCI group by J-MCIS was not confirmed to have MCI or dementia at a specialized medical facility. The J-MCIS is only a screening test for cognitive function and is not used for definitive diagnosis. The latter should be made by a physician at a specialized institution. Third, only 4 odors of the UPSIT-J-4 were used in this olfactory identification test. Although reliability may be a concern, this study showed that those who scored less than 2 correct answers had a higher probability of having an MPI of ≤49.8. The results of this study are meaningful from the perspective that a simpler method is recommended for routine screening of MCI.
This initiative is feasible in other regions and even abroad. It is excellent not only for enabling referrals to hospitals at an early stage of the disease, but also for longitudinal studies due to the nature of the salons.
Conclusion
This study revealed that about half of the elderly residents living without daily problems were suspected of having MCI. Therefore, it is crucial to develop simple methods leading to early detection and intervention, as well as to find appropriate places to implement them. The UPSIT-J-4 is a simple olfactory identification test, and can be used at any time and any place. It is useful for screening cognitive function via olfactory identification in a salon-like setting.
Footnotes
Acknowledgements
Authors’ Note
All work was performed at Oita University Faculty of Medicine.
Author Contributions
KY, AY, TC, ST, and EM were involved in study design and data interpretation. KY, SS, and EM were involved in the data analysis. All authors critically revised the report, commented on drafts of the manuscript, and approved the final report.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
The present study was approved by the ethics committee of Faculty of Medicine, Oita University (Approval No. 1686). Written informed consent was obtained from all participants.