
Abstract
Aims
To determine the effect of choice of inhalational anaesthetic (sevoflurane vs propofol) on the incidence and severity of postoperative cognitive dysfunction (POCD) in elderly patients (aged ≥ 60 years) with mild cognitive impairment (MCI).
Methods
Elderly patients with MCI undergoing radical rectal resection were randomly assigned to receive sevoflurane or propofol general anaesthesia. Cognitive function was assessed using neuropsychological testing before and 7 days after surgery. POCD severity was graded as mild, moderate or severe using standard deviation cut-offs.
Results
At 7 days after surgery, the incidence of POCD was 29.7% in the propofol group (n = 101) and 33.3% in the sevoflurane group (n = 99). There was a significant between-group difference for POCD severity: sevoflurane anaesthesia had a more severe impact on cognitive function than propofol anaesthesia.
Conclusions
There was no difference in the incidence of POCD at 7 days after radical rectal resection under sevoflurane or propofol-based general anaesthesia. Both propofol and sevoflurane were associated with negative cognitive effects, but sevoflurane had a more severe impact on cognitive function than propofol, in elderly patients with MCI.
Introduction
Postoperative cognitive dysfunction (POCD), which is a common brain complication following surgery and anaesthesia, is characterized by the impairment of recent memory, concentration, language comprehension and social integration. POCD may occur after any type of surgery, but is most often associated with cardiac surgery. 1 However, the prevalence of POCD after noncardiac surgery in elderly patients is substantial, with 25–56% of patients being affected during the first postoperative week. 2 Although studies have shown that inflammatory cascades may play a role in the pathogenesis of POCD, the precise interplay between its underlying mechanisms remains unclear. 3
The aetiology of POCD is complex: age, preoperative low baseline cognition, limited education and type of surgery may contribute to its occurrence. 4 Furthermore, the choice of anaesthetic drugs has also been alleged to affect cognitive function. 4 A number of animal studies have suggested a relationship between the inhaled anaesthetic administered and the development of dementia.5–8 Sevoflurane anaesthesia impaired spatial learning and memory in aged rats through an effect on amyloid β peptide oligomerization and deposition.5,6 Conversely, propofol, which is a commonly used intravenous (i.v.) anaesthetic, appears unlikely to produce persistent learning impairments in older animals.4,6 Clinical studies exploring the effect of sevoflurane on POCD in elderly patients have reached varying conclusions: some found that sevoflurane worsened cognitive impairment;9,10 some indicated that sevoflurane may have a beneficial effect on cognition,11,12 whereas some reported no cognitive effects. 13 However, none of these studies focused on patients with mild cognitive impairment (MCI) before surgery. MCI is thought to be an intermediate state between normal ageing and the development of Alzheimer’s disease (AD), and patients with MCI were found to experience a greater decline in concentration after surgery, compared with normal individuals. 14 These findings pose an interesting question as to whether patients with MCI experience greater cognitive decline after exposure to an inhaled anaesthetic.
We hypothesized that sevoflurane anaesthesia may result in more serious cognitive impairment than propofol anaesthesia. The present study aimed to establish whether there was a difference in the incidence and severity of POCD in an elderly cohort with MCI, following general anaesthesia with sevoflurane or propofol.
Patients and methods
Study population
This prospective, double-blind, randomized clinical trial recruited elderly patients with MCI (age ≥ 60 years; American Society of Anesthesiologists [ASA] grades I–III 15 ), scheduled for radical rectal resection surgery (Miles type) at The Affiliated Hospital of Luzhou Medical College, Luzhou, China, between January 2010 and November 2013. MCI was diagnosed according to the following criteria: 16 (i) memory complaints, documented by the patient and a collateral informant; (ii) Montreal Cognitive Assessment test score 15–24; (iii) Mini Mental State Examination (MMSE) 17 score ≤27; (iv) Activities of Daily Living 18 score <22; (v) no evidence of dementia. The control group comprised age- and ability matched elderly patients with a diagnosis of MCI who were not scheduled to undergo surgery. The control group was included simply to reduce the influence of any practice effect (which can be observed when neuropsychological testing is repetitively used). Control subjects were recruited from volunteers who were being treated on medical wards at the study hospital.
Exclusion criteria for all participants were: (i) current diagnosis of dementia (preoperative MMSE score <23); (ii) current or past psychiatric illness (that is, any brain disorder affecting cognition other than MCI); (iii) current use of antidepressant or antianxiety medication; (iv) history of drug dependence or alcohol abuse; (v) history of coronary artery, peripheral arterial or cerebrovascular disease; (vi) severe visual, auditory, or motor handicap; (vii) acute infection; (viii) preoperative haemoglobin <85 g/l.
This study was approved by the Affiliated Hospital of Luzhou Medical College Health and Human Research Ethics Committee. Written informed consent was obtained from each participant prior to enrolment.
Neuropsychological evaluation
Each participant underwent neuropsychological testing the day before surgery (day 1 in the control group) and 7 days postoperatively (day 8 in the control group). All tests undertaken for the purposes of the present study were performed in a quiet ward by one investigator (N.T.).
The neuropsychological evaluation test battery applied in our study was based on a Chinese version of neuropsychological testing. 19 The battery of tests assessed cognitive functions including executive function, motor skills, attention, learning and memory. Mental processing speed and visual scanning were tested with the trail-making test part A. 20 The amount of time that patients required to complete the test was measured. Concentration and the ability to ignore distracting stimuli were tested with the Stroop Colour and Word Test part 3. 21 This records the time needed to complete the test, as well as the number of errors. Concentration, processing speed and visual scanning abilities were tested with the Digit Symbol Substitution Test. 22 The total number of correct matches was measured.
Memory was evaluated with the Auditory Verbal Learning Test, 23 in which the physician reads 15 words that participants are required to recall immediately. The test was repeated five separate times. The total number of correct words immediately recalled across all five trials was recorded. After 30 min, free recall was used to evaluate long-term memory. Parallel versions of the word list were randomly used to minimize practice effects. Short-term memory and attention were assessed by the Digit Span Forward and Digit Span Backward tests. 22 The number of correctly recalled digits was measured.
Rates of depression and anxiety in the patients undergoing surgery were assessed by the Self-Rating Depression Scale 24 and the Self-Rating Anxiety Scale, respectively. 24
The visual analogue scale (VAS; 0, no pain; 10, severe pain) was used to assess pain at 1 week postoperatively.
Anaesthesia
Patients were randomly assigned to receive sevoflurane-based (group S) or propofol-based (group P) general anaesthesia. Random assignment was achieved before surgery by applying a computer generated, blocked random-allocation sequence with a 1 : 1 ratio. To ensure blinding, neuropsychological assessment work was carried out by a physician trained in psychology (N.T.). Neither the physician nor the patient knew which anaesthetic had been used during surgery.
Patients were not medicated prior to anaesthesia induction. All patients were anaesthetized according to the following standard induction protocol:midazolam (0.03–0.04 mg/kg, i.v.); fentanyl (0.002–0.003 mg/kg, i.v.); vencuronium (0.15–0.2 mg/kg, i.v.). Propofol (1.5–2.0 mg/kg, i.v.) was administered to patients in group P; 8% sevoflurane (fresh gas flow[FGF] 6 l/min, inhalation, decreased after loss of consciousness to 3–4%, FGF 1–2 l/min) was administered to those in group S. After endotracheal intubation, patients in group S were maintained under anaesthesia with sevoflurane (2–3%); those in group P were maintained with propofol (6–10 mg/kg per h). Bispectral indices (BIS) were monitored in both groups; a target range of 30–60 was maintained during anaesthesia by adjusting either the sevoflurane or propofol flow. Remifentanil (9–12 µg/kg per h, continuous i.v. infusion) was administered for analgesia and vencuronium (intermittent i.v. infusion), for muscle relaxation. All patients received routine anaesthetic monitoring and postoperative patient-controlled i.v. analgesia (150 ml normal saline containing fentanyl 1.5 mg, tropisetron 12 mg; infusion rate 2 ml per h; lockout time 15 min; duration 3 days).
Data recording
Intraoperative data that were recorded included: anaesthesia and surgical duration; remifentanil dose; atropine dose (0.2 mg atropine administered if heart rate ≤55 beats per min); hypotension (6 mg ephedrine administered if systolic blood pressure ≤90 mmHg or <30% of baseline for 5 min). Postoperative data that were recorded included pain score and postoperative complications.
POCD assessment
To assess POCD, the Z-value was calculated according to a published formula: 19 Z = (X–Xreference)/standard deviation (SD); where X is the difference between baseline and postoperative cognitive test scores in the trial group, Xreference is the difference between baseline and final time point in the control group, and SD is the change in score for the control group. When more than two tests had a Z-score ≥ 1.96, we defined the patient as having POCD. 19 SD cutoffs were used to grade severity of change as mild (change > 1 SD), moderate (change > 1.5 SD) or severe (change > 2 SD).
Outcome measures
Primary outcome measures were incidence and severity of POCD. Secondary outcome measures included anaesthesia duration, dose of remifentanil, and variations in heart rate and blood pressure.
Statistical analyses
Calculation of sample size was based on a pilot trial, with type I error probability 0.05 and power 85%. Based on these data, 110 participants were required for each group (1 : 1 ratio), allowing for a 20% dropout rate.
Data were presented as mean ± SD or n (%) and compared using one-way analysis of variance (ANOVA) and χ2-test with Fisher’s exact test, respectively. Between-group differences in continuous data were analysed using ANOVA with post hoc Tukey test. Between-group differences in categorical data were compared using Mann–Whitney U-test or Pearson χ2 analysis (when n ≥ 40 and theoretical frequency ≥ 5) or correction for continuity analysis (when n ≥ 40 and theoretical frequency 1–5). Statistical analyses were performed using SPSS® version 13.0 (SPSS Inc., Chicago, IL, USA) for Windows®. P-values < 0.05 were considered statistically significant.
Results
The study enrolled 220 patients with MCI: 68 were male and 152 were female; mean age 69.5 ± 4.3 years; age range 60–69 years (n = 126), ≥70 years, (n = 94). In addition, there were 60 control subjects: 22 were male and 38 were female; mean age 68.7 ± 5.2 years; age range 60–69 years (n = 42); ≥ 70 years (n = 18). There were no statistically significant differences in these data between the control and surgery groups (P ≥ 0.05).
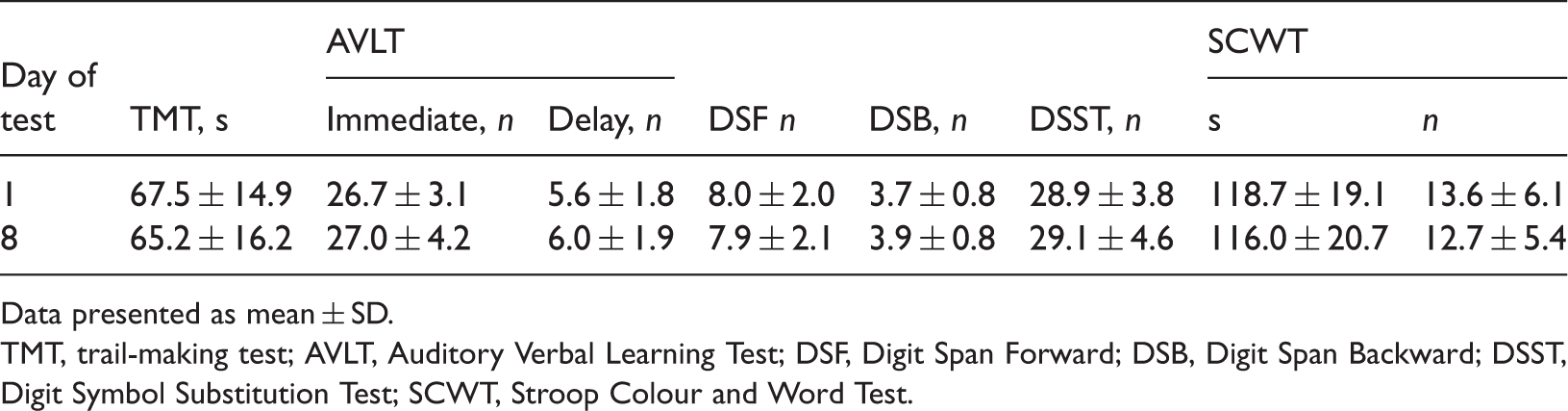
A flowchart of the trial is presented in Figure 1. A total of 20 patients (11 patients in group S; nine in group P) were not included in the final analysis: five patients with wound infection (group S, n = 2; group P, n = 3), seven with postoperative pneumonia (group S, n = 2; group P, n = 5); one who required repeat surgery (group P) and seven patients in group S who refused follow-up. The final analysis included 99 patients in group S and 101 in group P. There were no statistically significant differences between group P and group S with respect to demographic and perioperative data (Table 1). Test results for the control group are presented in Table 2; there was no significant difference in day 1 and day 8 (p ≥ 0.05).
Flow-chart of a study to determine the choice of inhalational anaesthetic (sevoflurane vs propofol) on the incidence of postoperative cognitive dysfunction in patients with mild cognitive impairment aged ≥60 years, scheduled for radical rectal resection surgery, and healthy volunteers of the same age range. Demographic, clinical and surgical characteristics of elderly patients (aged ≥ 60 years) with mild cognitive impairment, undergoing radical rectal resection under general anaesthesia using sevoflurane or propofol, included in a study investigating the effect of inhalational anaesthetic on postoperative cognitive dysfunction. Data presented as mean ± SD or n (%). COPD, chronic obstructive pulmonary disease; MMSE, Mini Mental State Examination; SDS, Self-rating Depression Scale; SAS, Self-rating Anxiety Scale; VAS: Visual Analogue Scale pain score (0, no pain; 10, severe pain). No statistically significant between-group differences (P ≥ 0.05; one-way analysis of variance [continuous variables] or χ2-test with Fisher’s exact test [categorical variables]). Assessments undertaken in elderly patients (aged ≥ 60 years) with mild cognitive impairment, recruited as the control group in a study investigating the effect of inhalational anaesthetic on postoperative cognitive dysfunction. These patients did not undergo any surgical procedures and merely underwent neurocognitive analyses to reduce the influence of any practice effect. Data presented as mean ± SD. TMT, trail-making test; AVLT, Auditory Verbal Learning Test; DSF, Digit Span Forward; DSB, Digit Span Backward; DSST, Digit Symbol Substitution Test; SCWT, Stroop Colour and Word Test.

Incidence and severity of postoperative cognitive dysfunction (POCD) in elderly patients (aged ≥ 60 years) with mild cognitive impairment, undergoing radical rectal resection under general anaesthesia, stratified according to inhalational anaesthetic.

Data presented as n (%).
χ2-test (POCD incidence), Mann–Whitney U-test (POCD severity) [Query 11]; bdecline in Z-score 1–1.5 SD from baseline; cdecline 1.5–2 SD from baseline; ddecline ≥2 SD from baseline.
NS, not statistically significant (P ≥ 0.05).
Discussion
The present study investigated the relationship between exposure to anaesthesia and POCD in patients with MCI. We found that the choice of sevoflurane or propofol as a general anaesthetic did not affect the incidence of POCD at 7 days in elderly patients with MCI, but a greater proportion of patients in the sevoflurane group experienced severe cognitive decline compared with the propofol group. This finding has several possible explanations.
Although its precise mechanism remains unclear, neuroinflammation has been implicated in the pathogenesis of POCD 3 and neurodegenerative diseases such as MCI. 25 Surgery is likely to be a trigger for inflammation, 3 since proinflammatory cytokine levels increase during surgery. These elevated levels of inflammatory biomarkers are associated with the activation of microglial cells that may lead to changes in cognitive function, through both direct and indirect effects on neurons.26,27 It is notable that the operative procedure is a necessary and major factor involved in the development of cognitive impairment, 3 since neuroinflammation elicited by the surgery itself appears to enhance ongoing neurodegeneration. 27 However, anaesthetics are capable of modulating inflammation and may alter the neuroinflammatory response.28,29 Propofol and sevoflurane have been shown to elicit only modest changes in cytokine expression in resting microglia without a specific ongoing inflammatory process (which acts through lipopolysaccharide [LPS] stimulation). 30 However, once these microglia were activated by LPS stimulation, sevoflurane allowed the LPS response to proceed unabated, and propofol exhibited dramatically reduced anti-inflammatory effects. This finding suggests that propofol may be a better general anaesthetic in terms of minimizing the neuroinflammatory response. The findings of the present study indicate that sevoflurane anaesthesia can aggravate the degree of impairment in patients with MCI, when compared with propofol anaesthesia.
Animal studies have found that inhaled anaesthetics can enhance amyloid β oligomerization and cytotoxicity in phenochromocytoma cells. 28 However, propofol modestly enhanced amyloid β oligomerization at very high concentrations and could attenuate sevoflurane-induced cytotoxicity. 31 Thus, it has been proposed that sevoflurane may promote Alzheimer’s disease neuropathogenesis. 28 In addition, sevoflurane may promote the progression of amnestic MCI after 2 years’ follow-up in older patients. 32
In direct contrast to the present findings, clinical studies have suggested that sevoflurane-based anaesthesia may be associated with better cognitive function than propofol-based anaesthesia for on-pump cardiac surgery. 12 This apparent difference may be due to the use of patients with MCI in the present study. Compared with those who do not have MCI, individuals with MCI have an increased risk of progressing to dementia, and patients with lower cognitive reserve might be more vulnerable to cognitive decline after surgery. 2 Furthermore, the age range of patients differed widely in these studies (≥18 years 12 vs ≥60 years in the present study), and there is evidence that the role of inhalational anaesthesia in cognitive function may be age-dependent. 31
The present study had a number of limitations. First, BIS were maintained at 30–60 instead of 40–60 during the anaesthesia, since BIS were always <40 when the recommended dose of propofol was injected at induction. Secondly, only short-term follow-up was performed, and larger studies of longer duration will be needed to clarify whether inhaled sevoflurane promotes long-term POCD in patients with MCI.
In conclusion, this study found no difference in the incidence of POCD at 7 days after radical rectal resection under sevoflurane or propofol-based general anaesthesia, in elderly patients with MCI. Both propofol and sevoflurane were associated with negative cognitive effects, but sevoflurane had a more severe impact on cognitive function than propofol in these patients.
Footnotes
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.