
Abstract
Introduction/Objectives:
We aimed to verify whether a sense of community scale developed for hospital wards can be applied to hospitals.
Methods:
A cross-sectional study was conducted using a self-administered questionnaire between July and October 2018 in 3 hospitals in Japan. The subjects were staff members working in these hospitals who provide direct medical or administrative services to patients and their families. The questionnaire inquired about the participants’ basic attributes and workplace satisfaction, and included the sense of community scale and the Japanese version of the Assessment of Interprofessional Team Collaboration Scale-II. We evaluated the scale’s structural validity, internal consistency, and hypothesis testing for construct validity.
Results:
Of 826 eligible staff members, 539 were included in the analysis. Mean age was 40.4 years and 77.4% were female. Exploratory factor analysis showed that 24 of the 28 items in the sense of community scale could be categorized under 3 factors. Confirmatory factor analysis demonstrated a goodness of fit index of 0.794, adjusted goodness of fit index of 0.752, comparative fit index of 0.885 and root mean square error of approximation of 0.092. Cronbach’s α for score in the sense of community scale was high (.96). Participants who reported high workplace satisfaction had significantly higher scores in the sense of community scale than those who indicated low workplace satisfaction (P < .001).
Conclusions:
We verified the reliability and validity of the Japanese version of the sense of community scale, which was originally developed for hospital wards, for the community in hospitals. With further verification, we hope the scale will be useful for evaluating the sense of community in hospitals.
Introduction
Rapid aging of the world’s population, particularly in advanced countries, 1 has led to a rise in the number of patients, including those with multimorbidity.2,3 Accordingly, the nature of patient and family problems has diversified.4,5 In this context, professionals working in healthcare settings are increasingly facing complex health issues. Given that no individual professional is equipped to solve these complex issues on their own, interprofessional collaboration is becoming increasingly necessary. 6 However, as the Austrian-American author Peter Drucker 7 notes, “A hospital is altogether the most complex human organization ever devised.” This complexity arises from the multiple professionals 8 such as doctors, nurses, and pharmacists working in hospitals who have different professional identity. 9 In addition, there are also non-medical staff such as clerical staff. Clerical staff can contribute to better patient care through sharing information and collaborating with medical staff because they often have opportunities to learn about patients’ economic and life conditions that are not known to medical staff. However, the lack of mutual understanding between medical and non-medical staff regarding their roles, effective communication, or shared vision within the hospital can reduce the quality of patient and family care and make it difficult to achieve patient-centered care. 10
The growth of interprofessional collaboration in recent years has been attributed to improvements in the quality of patient and family care.11,12 In 2010, the World Health Organization proposed a framework for interprofessional collaboration. 13 Since then, the concept of interprofessional education has gradually spread worldwide, and several countries have developed interprofessional competency frameworks.14 -17 In Japan, an interprofessional competency framework for collaborative practice was developed in 2016, 18 and the importance of interprofessional collaboration has been gradually recognized. To operationalize and sustain patient- and family-centered care requires a strong sense of teamwork, 19 a strengthening of a sense of belonging to the health community and a sense of efficacy. 20 The sense of belonging to a community, known simply as “a sense of community,” is defined as “a feeling that members have of belonging, a feeling that members matter to one another and to the group, and a shared faith that members’ needs will be met through their commitment to be together.” 21 That is, a sense of community describes an awareness and attitude that surrounds an individual in the community itself. A previous study reported that a low sense of community among hospital staff is associated with increased staff burden and reduced psychological health (quality of life). 22 A sense of community is expected to serve as a catalyst for interprofessional collaboration. Thus, assessing both interprofessional collaboration and sense of community may provide a strategy by which to visualize the collaboration in healthcare institutions. 23 However, few sense of community scales can be used in healthcare contexts. Previous studies that reported an association of the burden of primary health workers 22 and physician wellbeing 24 with a sense of community used part of the Copenhagen Psychosocial Questionnaire (COPSOQ) 25 to assess a sense of community. While some items of the COPSOQ assess a sense of community, the limited number of items and questions is insufficient to provide a detailed evaluation. In addition, because perceptions of the organization and community may differ among nations, measures used to assess a sense of community in studies conducted in other countries may not be useful in Japan without modification.
In Japan, a sense of community scale was developed by Yamaguchi et al 26 (Supplemental Material: Table S1) for nurses working in hospital wards. To ensure that this measure can be used to evaluate hospitals as communities beyond wards, it is necessary to verify its reliability and validity among all staff working in hospitals. The purpose of this study was, thus, to verify whether the sense of community scale developed for nurses working in hospital wards in Japan can be applied to the community in hospitals.
Methods
Research Design
We conducted a cross-sectional study using a self-administered questionnaire.
Participants and Settings
This study was conducted between July and October 2018 among all staff working in 3 hospitals (all regional hospitals with less than 200 beds) in Ibaraki Prefecture, Japan, who provide direct medical or administrative services to patients and their families (excluding cleaning, kitchen staff, etc.). The questionnaire was distributed to and collected from participants through our research collaborators. Of the participants, those who received the questionnaire but did not return it, did not consent to this study, or had missing values in the sense of community scale were excluded.
Contents of the Questionnaire
We collected participants’ basic attributes, including age, gender, profession, years of professional experience, and years of service in the current workplace, and their workplace satisfaction. The questionnaire also included the sense of community scale and the Japanese version of the Assessment of Interprofessional Team Collaboration Scale-II (J-AITCS-II). 27 The sense of community scale 26 is a 28-item (5-point grading method) scale developed for nurses working in hospital wards.21,28,29 The reliability and validity of this scale have been verified among nurses working in hospital wards based on a three-factor structure: Trust in coworkers (14 items), Professional orientation (9 items), and Open communication (5 items).26 J-AITCS-II is a 23-item measurement tool for evaluating collaboration within teams across various practice settings in Japan. We used J-AITCS-II to verify convergent validity because few sense of community scales can be used in healthcare contexts in Japan. Additionally, we evaluated workplace satisfaction using a visual analog scale (VAS) from 0 to 100, because VAS has been shown to be an appropriate method for evaluating satisfaction. 30
Statistical Analysis
The purpose of the analyses was to evaluate the sense of community scale’s structural validity, internal consistency, and hypothesis testing for construct validity. The sense of community scale was tested for ceiling and floor effects using the mean ± standard deviation (SD) score and percentage of participants with floor and ceiling scores. Unlike previous reports, which have only studied nurses working in hospital wards, we targeted various professions in the hospital. Thus, we conducted exploratory factor analysis (EFA) followed by confirmatory factor analysis (CFA). The sample size required for factor analysis was set at 200, based on a previous study. 31 EFA was performed to explore structural validity using data from hospital A. In EFA (maximum likelihood method, promax rotation), factor loading for all component items had to be at least 0.4. Items with factor loadings of 0.4 or higher for 2 or more factors were excluded. The researchers discussed the interpretability and then identified the factors. In addition, we also performed CFA to explore the hypothesis that the factor structure matches the results of EFA using data from the remaining 2 hospitals (B and C). The Goodness of Fit Index (GFI), Adjusted Goodness of Fit Index (AGFI), Comparative Fit Index (CFI), and Root Mean Square Error of Approximation (RMSEA) were calculated as indicators of model goodness of fit in CFA. According to a previous report, GFI and AGFI values of 0.9 or higher and CFI values closer to 1 indicate that a model has good fit, and RMSEA values less than or equal to 0.05 show that a model fits the data well, while a value of 0.1 or higher indicates that the model is undesirable. 32 Furthermore, internal consistency across each factor determined by EFA was calculated using Cronbach’s α coefficient. In addition, we hypothesized that the sense of community scale total score is associated with self-assessment of interprofessional collaboration and workplace satisfaction based on previous reports.33,34 First, for comparison with another measurement instrument (convergent validity), the sense of community scale and J-AITCS-II were assessed using Spearman’s rank correlation coefficient. Second, for comparison between subgroups (known-groups validity), we used the Mann-Whitney U test to analyze differences in the sense of community scale score between participants who reported high versus low workplace satisfaction. This assessment was based on the finding that enhancing a sense of community increases job satisfaction reported in a previous study. 34 Participant’s workplace satisfaction was categorized as high or low based on the median score. Missing variables, except for the sense of community scale, were handled using the pairwise deletion method. Analyses were performed using SPSS statistical software version 27 (IBM Corp., Armonk, New York) and Amos software version 25.
Results
Participant’s Attributes
A total of 826 participants were eligible, of whom 196 did not return the questionnaire, 54 did not consent to the study, and 37 were excluded because they had missing values in the sense of community scale, leaving 539 for inclusion in the analysis (Figure 1). Mean age was 40.4 ± 11.1 years and 77.4% were female. Participants belonged to the following professions: nurse (52.5%), clerical staff (18.4%), and doctor (4.6%) (Table 1). EFA was conducted using data from 241 patients in Hospital A and CFA using data from 298 patients in Hospitals B and C.

Study participant flow.
Subject attributes.
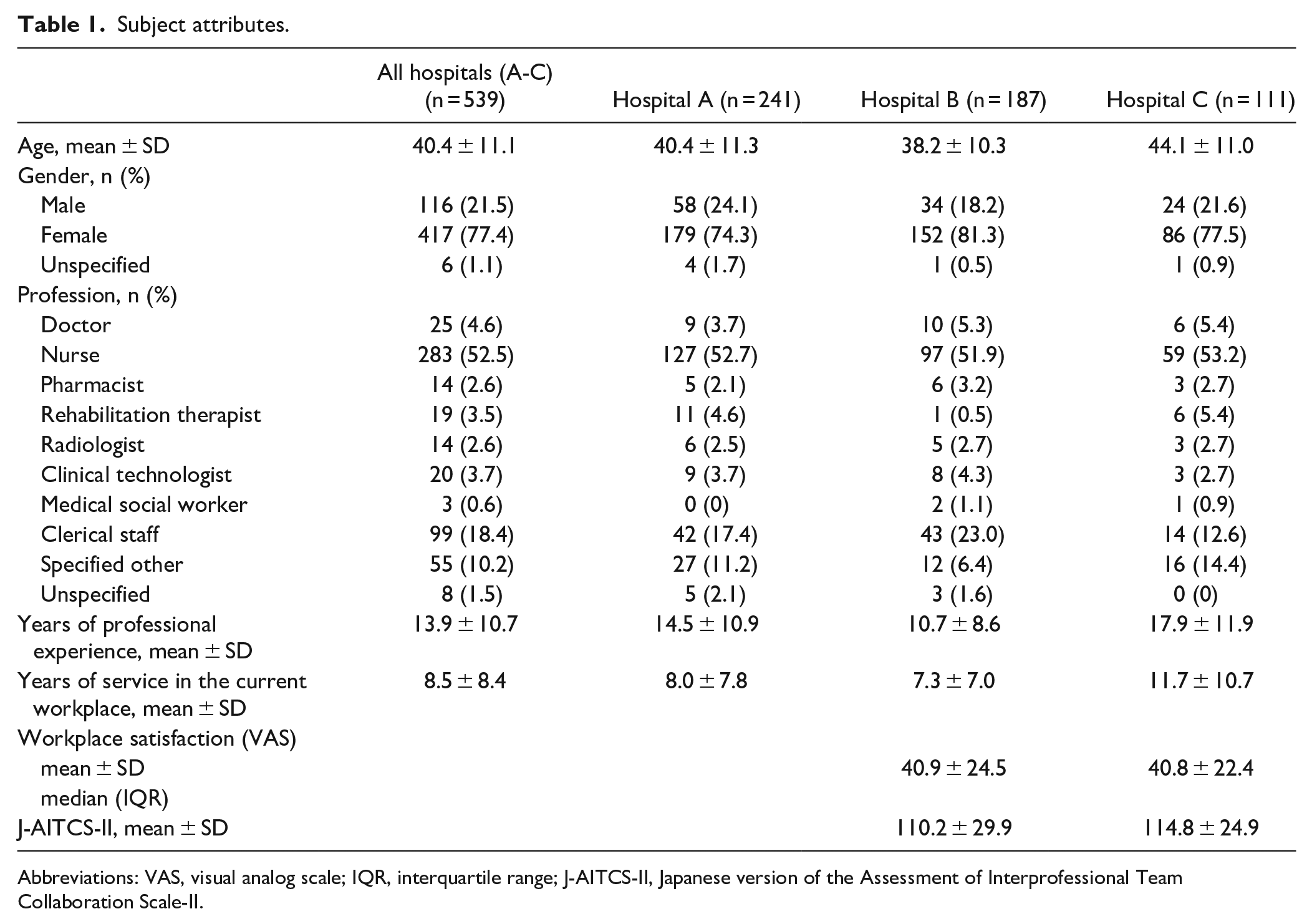
Abbreviations: VAS, visual analog scale; IQR, interquartile range; J-AITCS-II, Japanese version of the Assessment of Interprofessional Team Collaboration Scale-II.
Description of the Scale
Responses to the sense of community scale are shown in Supplemental Table S2. No floor or ceiling scores were found for any of the items. In addition, nearly one-third of the participants (30.7%) reported the maximum possible score for item 22, while 21.6% reported the minimum score for item 28. Therefore, no ceiling or floor effect was found in either item.
Structural Validity and Internal Consistency
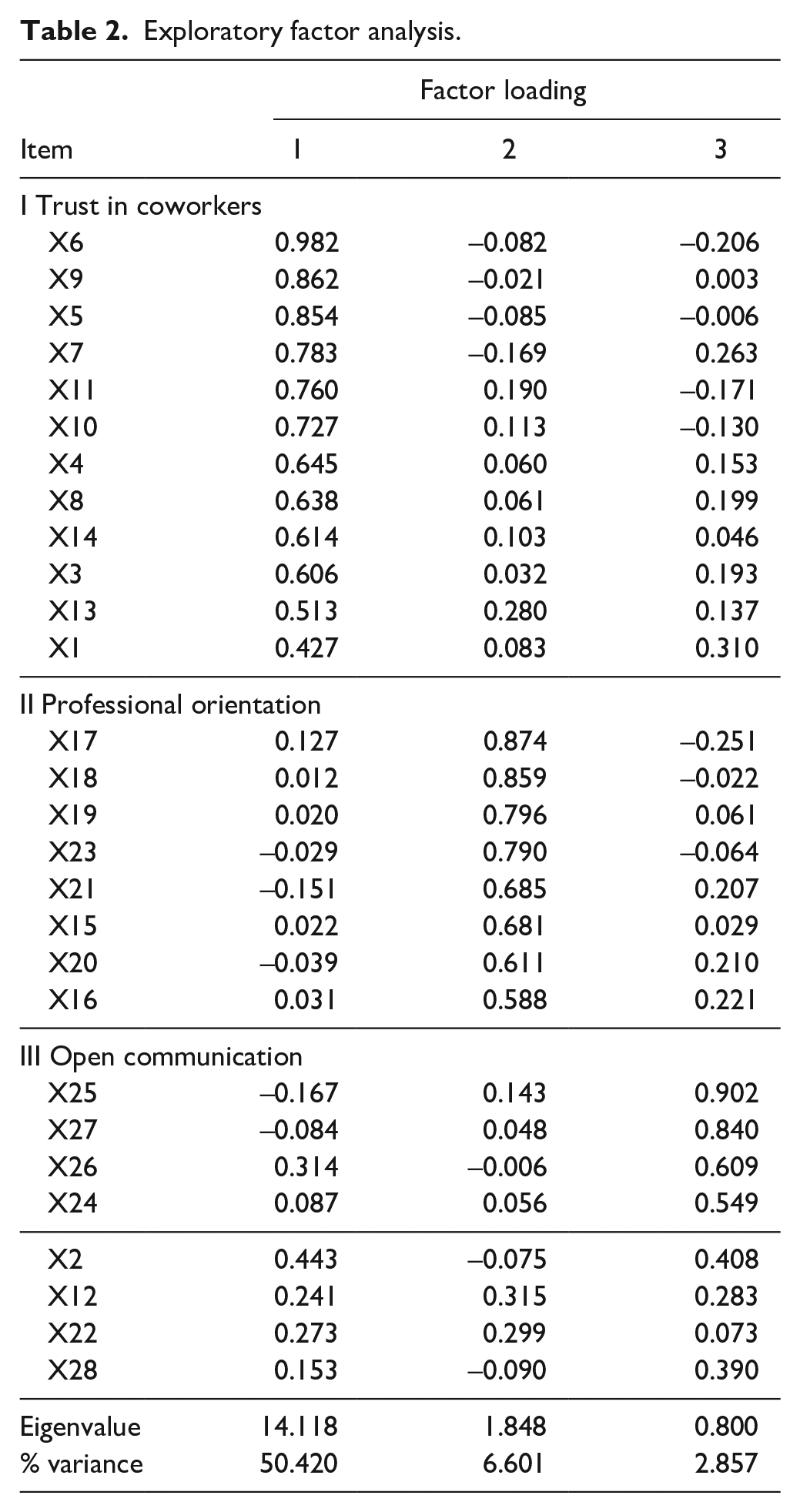
In EFA, 24 of the 28 items in the sense of community scale could be classified under the 3 identified factors. Three items could not be classified because they had factor loadings less than 0.4: “12. My colleagues and I respect each other,” “22. At the moment, I do not want to be transferred from my present workplace to another one,” and “28. I borrow things from other members or exchange favorite things with other members.” The remaining item, “2. Communication among the members is discussed,” could not be classified because it had factor loadings greater than 0.4 for 2 factors (Table 2). The 24 items were categorized among the following 3 factors: “Trust in coworkers” (12 items), “Professional orientation” (8 items) and “Open communication” (4 items), as in the original study. 25 The correlation coefficient was .649 between the first and second factors, .730 between the first and third factors, and .724 between the second and third factors. The Kaiser-Meyer-Olkin (KMO) value was 0.946 and Barlett’s test for sphericity was significant (χ2 = 5576.032, df = 378, P < .001). The 3 factors identified in EFA showed a cumulative contribution rate of 59.9%; the individual contribution rates were 50.4% for factor I, 6.6% for factor II, and 2.9% for factor III. In addition, CFA was performed using the factor structure revealed in EFA. Factor loadings of the hypothetical model and correlations between the factors are shown in Figure 2. Regarding goodness of fit for this model, GFI was 0.794, AGFI was 0.752, CFI was 0.885 and RMSEA was 0.092. Cronbach’s α was .96 for all items, .95 for the first factor, .90 for the second factor, and .88 for the third factor.
Exploratory factor analysis.

Confirmatory factor analysis of the sense of community scale.
Hypotheses Testing (Convergent Validity and Known-Groups Validity)
The median (interquartile range) J-AITCS-II score and sense of community scale score (24 items), which were not normally distributed, were 69 (62-81) and 81 (72-92), respectively. Spearman’s rank correlation coefficient between these scales was .44 (P < .001). In addition, the median sense of community scale score of participants who reported high (>41) and low (≤41) workplace satisfaction, categorized based on a median score of 41, was 88 (79-97) and 74 (66.3-84), respectively. Congruent with our hypothesis, these scores were significantly different (P < .001).
Discussion
We verified the reliability and validity of the Japanese version of the sense of community scale, which was originally developed for nurses in hospital wards, for the community in hospitals. EFA demonstrated that when conducted among hospital staff, the sense of community scale comprised a 3-factor structure: Trust in coworkers, Professional orientation, and Open communication. In addition, Cronbach’s α was greater than 0.8 for all 3 factors, confirming the internal consistency of this scale. We also confirmed the convergent validity and known-groups validity. However, while we confirmed the construct validity of this scale using CFA, the data did not show good fit. Therefore, we suggest that the results of factor-by-factor analysis be carefully considered when using this scale to evaluate the sense of community in hospitals.
The 3-factor structure revealed in EFA was the same as that described in a previous study. 26 However, 4 of the 28 items in the sense of community scale were not included under any of the 3 identified factors. This may be because the participants of this study had varying professions, whereas the previous study involved only nurses. The first of the excluded items was “12. My coworkers and I respect each other.” The interpretation of “coworker” may differ among staff with different professions in hospitals. Each healthcare profession is specialized and has a professional identity, defined as one’s professional self-concept developed based on one’s attributes, beliefs, values, motives, and experiences.9,35 These characteristics are fostered throughout undergraduate and postgraduate education, and in job assignments (work in the same ward or in different wards). We predict that these differences may have affected the participants’ interpretation of the term “coworker,” leading to the exclusion of item 12 from the 3 identified factors related to a sense of community among all hospital staff in this study. The second item was “22. At the moment, I do not want to be transferred from my present department to another one.” Given the organizational structure of hospitals, the intragroup trust or relationship between nurses and other staff may differ. Nurses are the most numerous of the professionals working in hospitals, 36 and are typically assigned to a single ward. In contrast, other professionals typically work across wards because they are fewer in number. We predict that professionals other than nurses may have thought that the term “transferred” did not apply to them, leading to the exclusion of item 22. The third item was “28. I borrow things from other members or exchange favorite things with other members.” The exclusion of this item in our study may be related to the fact that most nurses are women. Women are reportedly more likely to see themselves as being interdependent or relational—a phenomenon termed “interdependent self-construal”37,38—making them more likely to possess peer awareness. 39 We predict that this item may only be useful for studies in nurses and not those involving other hospital staff. The fourth item was “2. Communication among the members is discussed.” This item had factor loadings greater than 0.4 for both “Trust in coworkers” and “Open communication.” The use of an ambiguous question asking about communication among members may be the reason why this item did not apply to a specific factor.
CFA showed the goodness-of-fit values of the 3-factor model revealed in EFA. A previous study that administered the sense of community scale to nurses working in hospital wards confirmed the tool’s content validity and criterion-related validity, but not construct validity. 26 In the present study, GFI was 0.783, AGFI was 0.741, CFI was 0.88, and RMSEA was 0.093, which indicate that the scale has a degree of validity but does not meet the criteria for high model goodness of fit. The reason for this may be that, because a hospital is a place where professions with diverse identities coexist, 34 differences in relationships among those with different professions and their self-perception of “wards” and “professions” affect the sense of community in the workplace.
There was a positive correlation between the sense of community scale and J-AITCS-II used to assess interprofessional collaboration (ρ = .44), confirming the tool’s convergent validity. The authors of a previous study argued that a greater sense of community is useful for improving isolated and fragmented relationships between professionals. 40 Therefore, in addition to existing methods for assessing interprofessional collaboration, our verification of the validity of a sense of community scale for all hospital staff is significant for facilitating the development of future sustainable interprofessional collaboration.
The present study had some limitations. First, the sample size per hospital was insufficient. Although differences in workplace satisfaction and J-AITCS-II between participants in hospitals B and C were small, it is possible that combining the 2 populations into a single group in the analysis affected the results. Second, more than half of the participants were nurses, which may explain the similarity in results to previous studies that only included ward nurses. However, given that nurses typically account for half of the total working population in hospitals, 36 we expect that the results will be generalizable to other hospitals of similar size. In addition, as there are cultural differences between Japan and other countries, the results of this study should be interpreted with this in mind.
Conclusions
We verified the structural validity, internal consistency, and construct validity of a sense of community scale for use in hospitals. With further verification, this scale may be useful for evaluating the sense of community among not only nurses in hospital wards but also hospitals in Japan.
Supplemental Material
sj-xlsx-1-jpc-10.1177_21501319221107317 – Supplemental material for Verification of a Sense of Community Scale for Hospitals in Japan
Supplemental material, sj-xlsx-1-jpc-10.1177_21501319221107317 for Verification of a Sense of Community Scale for Hospitals in Japan by Ryohei Goto, Junji Haruta and Sachiko Ozone in Journal of Primary Care & Community Health
Supplemental Material
sj-xlsx-2-jpc-10.1177_21501319221107317 – Supplemental material for Verification of a Sense of Community Scale for Hospitals in Japan
Supplemental material, sj-xlsx-2-jpc-10.1177_21501319221107317 for Verification of a Sense of Community Scale for Hospitals in Japan by Ryohei Goto, Junji Haruta and Sachiko Ozone in Journal of Primary Care & Community Health
Footnotes
Acknowledgements
We sincerely appreciate the participation of healthcare professionals from the 3 community hospitals. Moreover, we thank Dr. Yuto Takeuchi, Dr. Akie Sakakura, and Dr. Satoko Takahashi for data input.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by the Ethics Committee of the Faculty of Medicine, University of Tsukuba (approval number: 1202-3). All study participants provided informed consent in writing after being given an explanation about the purpose and methodology of the study, that study participation was voluntary, and the protection of personal information.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.