
Abstract
Purpose:
Evidence-based models of cancer survivorship care are lacking. Such models should take into account the perspectives of all stakeholders. The purpose of this integrative review is to examine the current state of the literature on cancer survivorship care from the cancer survivor, the oncology care team, and the primary care team perspectives.
Methods:
Using defined inclusion and exclusion criteria, we conducted a literature search of PubMed, PsycINFO, CINAHL, and Scopus databases to identify relevant articles on the stakeholders’ perspectives on cancer survivorship care published between 2010 and 2021. We reviewed and abstracted eligible articles to synthesize findings.
Results:
A total of 21 studies were included in the review. Barriers to the receipt and provision of cancer survivorship care quality included challenges with communication, cancer care delivery, and knowledge.
Conclusion:
Persistent stakeholder-identified barriers continue to hinder the provision of quality cancer survivorship care. Improved communication, delivery of care, knowledge/information, and resources are needed to improve the quality of survivorship care. Novel models of cancer survivorship care that address the needs of survivors, oncology teams, and PCPs are needed.
Introduction
An estimated 16.9 million Americans, most over the age of 65, were living with a history of cancer as of January 2019. 1 By 2030, the number of cancer survivors in the United States is expected to exceed 22 million. 1 This trend is primarily fueled by advances in early detection and treatments. 2 However, survival comes with its own challenges. Many survivors suffer from multiple comorbidities and have complex medical and psychosocial needs.3,4 In addition to quality of life (QOL) concerns, survivorship care can be complex and fragmented. 5 For survivors of cancer, the completion of treatment does not mark an end to their cancer experiences. 6 Survivorship care may include follow-up surveillance, management of late and long-term adverse treatment effects, healthy living recommendations (diet, physical activity, tobacco cessation, other cancer screening), and comorbidity management. 5 Continued relationships with the healthcare system are often needed to manage long-term survivorship care. 7
Current models of cancer survivorship care often fail to meet survivors’ physical, psychosocial, and informational needs. 8 Such needs are compounded by the challenges of a fragmented healthcare system where coordination and communication between different medical specialties are often challenging. Evidence suggests that the implications of fragmentation of care can result in greater spending, delays in treatment, prevention, and surveillance for recurrences and new cancers and comorbid conditions. 9 Initially, post-treatment follow-up and surveillance may primarily be provided by oncologists; however, this places a heavy burden on the oncology team.10,11 By contrast, a full transition to primary care physicians (PCP) can also create burden and PCP care delivery constraints. In addition, PCPs may have limited knowledge and formal training on survivorship care.6,7,12,13 Cancer survivors often develop strong emotional bonds with the oncology team and may prefer to be followed by their oncology team for cancer surveillance and management of late and long-term treatment effects, as well as preventative care. 14 Historically, systems have not coordinated care ongoing between primary care and oncology throughout treatment, which can exacerbate survivors’ hesitancy to return back to primary care following cancer care.
The purpose of this integrative review is to examine the literature on cancer survivorship care from the perspectives of the cancer survivor, the oncology care team, and the primary care team. Findings will be used to understand knowledge gaps, identify potential barriers to the provision of cancer survivorship care, and inform improvements to current survivorship care delivery models.
Methods
This integrative review was conducted using methods proposed by Russell 15 and Toronto and Remington. 16 Integrative reviews are used to represent the state of the research literature on a given topic, identify central issues in an area, and identify future research and practice implications.15,16 The method was selected for this review to provide a more holistic approach to understanding stakeholder perspectives of cancer survivorship care. The 5 stages of the integrative review were used: problem formulation, literature search, data evaluation, data analysis, and presentation.
Problem Formulation
This review was undertaken due to the longstanding, persistent challenges in communication, care delivery, and knowledge during cancer survivorship. 13 Our specific review questions include the following: (1) What are the overall perspectives of various stakeholders on the provision of cancer survivorship care? (2) What are the barriers to the provision of cancer survivorship care from the stakeholders’ perspectives? The National Cancer Institute’s (NCI) Office of Cancer Survivorship defines a “cancer survivor” as an individual from the time of cancer diagnosis through the balance of life and recognizes that there are many phases of cancer survivorship, including those living with cancer and those free of cancer. 17 This definition was used to guide our review to include the various challenges associated with this extended period, ranging from Acute to Extended to Permanent Survival. 18
Literature Search and Data Evaluation
A comprehensive, computerized search of the literature in Medline (PubMed), PsycINFO, CINAHL, and Scopus was conducted in August 2021. The search was restricted to English language articles published from 2010 to 2021. Search keywords included “Shared Care Model,” “Cancer Survivorship,” “Oncology,” “Oncology Nursing,” “Oncology Advanced Practice Nurse,” “Primary Care,” “Patient,” and “Survivor.” MeSH terms for Medline and CINAHL included “Oncology,” “Primary Care,” and “Survivorship.”
As proposed by Russell 15 and Toronto and Remington, 16 data evaluation involves the appraisal of the relevance of the selected literature. Publications were selected for full-text reviews by a screening of titles and abstracts. Full-text articles were selected for inclusion based on the following criteria: (1) any cancer type; (2) any phase of cancer survivorship based on NCI definitions; (3) articles that focused on one or a combination of stakeholder perspectives on the provision of cancer survivorship care; and (4) studies conducted in the United States. Exclusion criteria included: (1) editorials and case studies; and (2) studies conducted outside of the United States. We chose to exclude studies conducted in other countries in an effort to focus on cancer survivorship care delivery within the United States healthcare delivery system. Published systematic reviews and other narrative reviews were accessed for their reference lists. Two investigators (ML, VS) reviewed all articles for inclusion, and discordant reviews were discussed until consensus was reached.
Data Analysis and Presentation
All articles selected for final review were read by 2 reviewers (ML, VS). Data abstraction was completed using a pre-determined data document. Extracted study characteristics include first author, year of publication, study aim, stakeholders involved, sample size, cancer type(s), phase of cancer survivorship based on NCI definitions, and study design. Articles were categorized by survivor, oncology, and/or primary care perspectives. All articles that focused on one stakeholder alone were counted as one article, while those that included multiple stakeholder perspectives were counted once for each of the stakeholders that were included. To identify findings related to the provision of cancer survivorship care, all 21 articles were reviewed and coded for themes relevant to care provision (ML, VS). Discordant codings were discussed until consensus was reached.
Results
The flow chart of search and selection procedures is depicted in Figure 1. A total of 551 articles were identified in the initial search. Of this total, 305 were excluded after accounting for duplication, leaving 246 articles that underwent title/abstract screening. After title/abstract screening, 211 articles were excluded, leaving a final of 35 for full-text review. After a full-text review, 14 articles were excluded, yielding a total of 21 articles (3.8%) that met the inclusion criteria. Of the 21 eligible articles, 12 articles (57%) addressed cancer survivor perspectives (see Table 1). Of note, 8 out of the 12 articles (67%) focused on cancer survivors exclusively. A total of 10 articles (48%) addressed the oncology care team’s perspective (oncologists and oncology nurses); none of the articles targeted oncology perspectives exclusively. Finally, 12 articles (57%) addressed the primary care team’s perspective (57%); only 3 articles (25%) were exclusive to primary care.
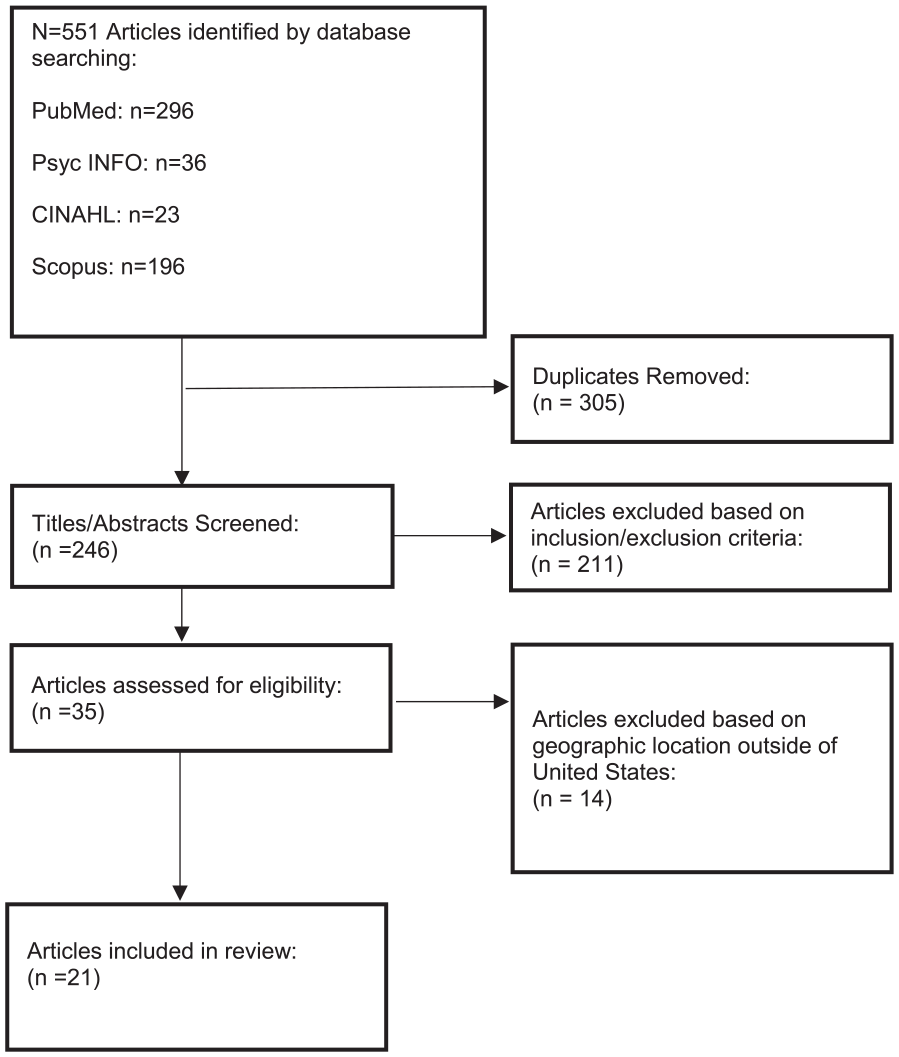
Search and study selection flow chart.
Characteristics of Studies Included in the Review (Organized by Stakeholders).

Overall Summary of Findings
Key study characteristics for the 21 articles are presented in Table 1. For articles that included cancer survivor perspectives, the most common cancer type is breast and colorectal. Many articles included multiple cancer types that were not specified. The most common phases of cancer survivorship were the extended phase and the permanent phase. The majority of articles were qualitative studies; of note, 4 articles described findings from randomized trials on survivorship care planning and care delivery.
Findings by Survivorship Care Provision Themes
Survivor Perspectives
For the 12 articles that either focused exclusively or included survivor perspectives, 3 overarching themes emerged. They included communication (11/12; 91.7%), cancer care delivery/post-treatment care (11/12; 91.7%), and a lack of information/limited knowledge (10/12; 83%).
Communication
The theme of communication from the survivor’s perspectives was primarily focused on barriers. These barriers ranged from lack of timely communication, poor communication/information from the medical team, transparency of out-of-pocket costs, and a need for consistent advice from multidisciplinary care team members. Many studies reported the need for care coordination as survivors often experienced instances of issues in relaying information to both primary care and oncology care teams. Additionally, survivors reported the need for consistent advice from providers as confusion over conflicting instructions often occurred.
Care delivery
Survivors reported a lack of confidence in their general practitioner’s knowledge and ability to provide cancer survivorship care, and dissatisfaction with health providers for reasons such as unresponsiveness and dismissiveness. Extended wait times for follow-up appointments, tests, and lack of access to services also posed problems to post-treatment care from the survivor’s perspective. Additionally, patients faced instances of delaying or canceling treatment due to the financial toxicity associated with survivorship care. According to the NCI, financial toxicity is defined as the problems a survivor faces related to the cost of medical care that may lead to debt and bankruptcy, which can negatively affect a patient’s quality of life and access to care. 41
Limited knowledge
Overall, survivors expressed a lack of information in multiple facets of their post-treatment follow-up care. The unmet informational needs were focused on cancer treatments, treatment-related side effects/toxicities, diet, healthy living, recurrence, follow-up, long-term effects of treatment, and when to see their providers in the future. In addition, survivors perceived a lack of clarity on the PCP’s role in their cancer care, further compounding the survivor’s confusion on matters related to their follow-up care.
Oncology Perspectives
For the 10 articles that either focused exclusively or included oncology perspectives, 2 common themes were identified: communication (9/10; 90%) and care delivery (8/10; 80%). Approximately one-third of the oncology articles included perspectives from oncology nursing teams (3/10; 30%), contributing a unique point of view to the overall oncology perspective.
Communication
Similar to survivors, the oncologists and oncology care teams experience significant obstacles to communication. The critical barrier is the lack of communication with PCPs regarding survivorship care. Oncologists/oncology teams also perceived communication barriers with survivors in some cases, specifically with language barriers that pose challenges in transferring information on survivorship care.
Care delivery
As a result of the communication barriers, several concerns related to care delivery and post-treatment care were reported. These include concerns regarding general preventive healthcare responsibility, duplicated care, requests from survivors for unnecessary testing, and insurance restrictions on tests or treatments. The oncology care teams also expressed difficulties in transferring care responsibilities and finding the time and resources needed to provide personalized survivorship care plans.
Oncology nursing perspective
Of the articles reviewed, one-third included perspectives from registered nurses, nurse practitioners, and advanced practice nurses. Nurses expressed challenges with both communication and care delivery. In terms of communication, nurses reported a lack of systematic referrals from either oncology or primary care teams to survivorship care nurses. Additionally, nurses voiced continuous efforts to make survivorship care plans more patient-friendly in order to meet varying literacy levels of patients. For care delivery, nurses expressed that they were often tasked with completing survivorship care plans. However, they reported insufficient organizational resources, such as time, staff, money, and training to support their role in some cases. In addition, there were often inconsistent institutional systems to facilitate care plan completion (ie, electronic templates embedded in electronic medical records).
Primary care perspectives
For the 12 articles that either focused exclusively or included primary care perspectives, 3 underlying themes were identified: communication (11/12; 92%), care delivery (11/12; 92%), and limited knowledge (10/12; 83%).
Communication
For primary care teams, a common communication obstacle was the lack of consistent updates on survivor prognosis throughout the course of treatment. Primary care teams report being informed of their survivor’s cancer diagnosis; this is often followed by a long period of communication gap during treatment. Consequently, primary care teams expressed concerns with the quality and fragmentation of care associated with the lack of communication across medical specialties.
Care delivery
Concerns regarding care delivery were prevalent in the primary care perspective and were focused on follow-up and comorbidity management. For the primary care team, the quality of oncology follow-up care remains a concern as the primary care responsibility of managing certain aspects of care is often not clearly defined. The primary care team also reported a lack of training on how cancer treatments can further exacerbate comorbidities. Consequently, there are concerns about the quality of comorbidity management. For example, survivors undergoing treatment for lung cancer with chronic obstructive pulmonary disease as a comorbid condition may experience exacerbated symptoms. 42 Instances such as this can cause complication in the decisions made in the course of comorbid condition treatment due to the limited consensus on how to manage comorbidities in the context of cancer.
Limited knowledge
Primary care teams report a lack of or insufficient formal training on cancer survivorship care. Consequently, PCPs reported limited knowledge on the principles of cancer survivorship care and on management guidelines. Areas of deficiency in knowledge and training included the frequency/types of cancer surveillance and the long-term effects of cancer treatments.
Discussion
Since the introduction of the U.S. Institute of Medicine’s 2006 seminal report, “From Cancer Patient to Cancer Survivor: Lost in Transition,” a range of research has been carried out to better address the unique needs of cancer survivors. 43 This report outlined the vital components of survivorship care and recommended the development of a survivorship care plan to improve communication and coordination between oncologists and PCPs. Nearly a decade and a half later, many of the same stakeholder-identified barriers to the delivery of quality survivorship care remain. Persistent challenges remain in areas such as timely communication between medical specialties, unmet informational/training needs, and challenges in coordinating care responsibilities between medical specialties. Notably, PCPs reported a lack of communication from the oncology team after being notified of a patient’s cancer diagnosis. The provider-to-provider communication voids are often filled by survivors themselves, with many serving as the communication “bridge” between providers on their treatments and surveillance plan. Although most PCPs view survivorship care as an important component of their work and agree with the importance of their role in survivorship care, more research is needed to understand why persistent barriers exist for PCPs. A viable strategy is to design cancer survivorship research with PCP involvement and engagement. The review also revealed support for caregivers as an unmet need from the survivor’s perspective.
Many of the reported challenges continue to focus on the time and resources needed to complete a survivorship care plan. This result may be associated with previous survivorship care accreditation guidelines from the American College of Surgeons’ Commission on Cancer (CoC), which required the completion and provision of a care plan. Published systematic reviews and meta-analyses found that care plans alone do not improve the quality of care delivery and coordination following treatment. 44 Accreditation guidelines, including those from the CoC, have since been revised to emphasize the development of robust survivorship programs rather than achieving a threshold percentage for the receipt of a survivorship care plan document. 45 Future research should focus on stakeholder perspectives on developing comprehensive survivorship care programs to improve communication and care coordination. Additionally, research should encourage the integration of primary care and oncology care throughout care delivery to foster equally strong relationships among patients and all of their providers.
The findings of this review were consistent with those of recent systematic reviews on the topic.44-46 Calls for more defined roles in cancer follow-up care, improved and timely information sharing, and protocols for survivorship care were also highlighted in these systematic reviews. Importantly, an understudied area of research is the critical perspectives on the challenges faced by oncology nurses as integral members of the cancer survivorship care team, a point further revealed in our findings. As vital members of the care team, oncology nurses participate in survivorship care; advanced practice nurses (ie, nurse practitioners, clinical nurse specialists) are often leading survivorship care efforts, either working alone or collaborating with interdisciplinary teams. Nurse-led care coordination and communication can potentially reduce care fragmentation after cancer treatments, and research is needed to test interventions and programs that include oncology nurses as crucial care team members. 47 With advances in treatments such as immunotherapies, the field of cancer survivorship has expanded its focus to address the care for survivors living longer with advanced and metastatic cancers. Research is needed to test models of comprehensive survivorship care for these populations, including care delivery research that addresses the preferences of survivors and providers and care team integration of primary care in partnership with subspecialists. 19 Finally, our review found a noticeable lack of evidence on the support person/family caregiver’s perspectives on cancer survivorship care; only one of the studies included in this review included this population.
A potential model of cancer survivorship care that may address the needs of all stakeholders is the Self-Management Shared Care Model. 48 The model fosters transdisciplinary collaboration among oncologists, oncology nursing, and primary care teams, with a focus on care coordination among medical specialties and communication between survivors and providers. Survivors are coached on the principles of self-management, which aims to empower and enable them through goal-setting, identifying challenges, and developing an action plan to overcome challenges. The model also leverages supportive care expertise (ie, dietitians, rehabilitation, psychology/psychiatry) for a more comprehensive survivorship care approach.49,50 Evidence from other countries suggests that in breast cancer survivors, the shared care approach improved receipt of timely follow-up screening, decreased waiting time to receive oncology care, and freed up clinician time by shifting resources to survivors with more complex needs. 51 Implementation of the self-management shared care model will likely be more complex in the United States due to diverse care delivery systems, and more evidence is needed on its effectiveness in the United States healthcare system. 47
Limitations
While the review was guided by an integrative review framework15,16 and used a methodological approach, we did not focus on the quality/level of evidence. Additionally, the review was limited to studies conducted in the United States and articles published in the English language, potentially excluding stakeholder perspectives published in other languages and countries with different healthcare systems. We acknowledge that much of the existing evidence on cancer survivorship care delivery is from Canada, Australia, and Europe; however, this was beyond the aim and scope of the review.
Conclusions
Persistent barriers in providing quality cancer survivorship care exist from the perspectives of survivors, the oncology team, and PCPs. These barriers included the need for improved communication, delivery of care, knowledge/information, and resources for the provision of quality survivorship care. Research is needed to test the impact of novel models of care that address the needs of survivors, oncology teams, and PCPs. The design of comprehensive cancer survivorship care program and research should include the perspectives of all stakeholders, including oncology nurses and family caregivers.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this paper is supported by the National Cancer Institute of the National Institutes of Health under award number R01CA249501-01 (PI: Sun). The statements presented in this article are solely the responsibility of the author(s) and do not necessarily represent the official views of the National Institutes of Health.