
Abstract
Introduction:
Primary care clinicians are presented with hundreds of new clinical recommendations and guidelines. To consider practice change clinicians must identify relevant information and develop a contextual framework. Too much attention to information irrelevant to one’s practice results in wasted resources. Too little results in care gaps. A small group of primary care clinicians in a large health system sought to address the problem of vetting new information and providing peer reviewed context. This was done by engaging colleagues across the system though a primary care learning collaborative.
Methods:
The collaborative was a grass roots initiative between community and academic-based clinicians. They invited all the system’s primary care clinicians to participate. They selected new recommendations or guidelines and used surveys as the principal communication instrument. Surveys shared practice experience and also invited members to give narrative feedback regarding their acceptance of variation in care relate to the topic. A description of the collaborative along with its development, processes, and evolution are discussed. Process changes to address needs during the COVID-19 pandemic including expanded information sharing was necessary.
Results:
Collaborative membership reached across 5 states and included family medicine, internal medicine, and pediatrics. Members found involvement with the collaborative useful. Less variation in care was thought important for public health crises: the COVID pandemic and opioid epidemic. Greater practice variation was thought acceptable for adherence to multispecialty guidelines, such as diabetes, lipid management, and adult ADHD care. Process changes during the pandemic resulted in more communications between members to avoid practice gaps.
Conclusion:
An internet-based learning collaborative in a health system had good engagement from its members. Using novel methods, it was able to provide members with feedback related to the importance of new practice recommendations as perceived by their peers. Greater standardization was thought necessary when adopting measures to address public health crisis, and less necessary when addressing multispecialty guidelines. By employing a learning collaborative, this group was able to keep members interested and engaged. During the first year of the COVID pandemic the collaborative also served as a vehicle to share timely information.
Keywords
Introduction
Primary care clinicians are presented with hundreds of clinical recommendations and guidelines. The United States Preventive Services Task Force (USPSTF) alone has nearly 100 recommendations, 23 of them new in the past 2 years. 1 Specialty societies and disease or organ specific organizations have over 1000 guidelines related to primary care. 2 Translating research into practice is difficult, often taking many years. 3 Incorporating new recommendations requires practice change, which has costs; costs which may take away from other elements of practice. 4 Before a decision to invest in practice change clinicians must identify relevant information 5 and then develop a contextual framework relating it to one’s practice.6-9
With so much competing and at times conflicting information both intra practice and inter practice variation will result. Inter practice variation may be intentional due to factors such as clinician, administrative, or community preference.10,11 Or it may be unintentional due to knowledge or resource deficits. Likewise intra practice variation may be intentional due to customization or unintentional due to inconsistent processes. 12 To compound the problem, there are often conflicting recommendations such as those with colon cancer 13 or prostate cancer screening.14,15 Whereas customization may enhance the quality and satisfaction of care, 16 unwanted variation may result in added costs, inefficiency, and potential gaps in care. 17
Although individualized care (personalization) is the goal of all primary care clinicians, within specialties, regions, health care systems, or practices, patients should expect consistent care (standardization) surrounding certain elements of practice.2,15 In our large health system 5 primary care clinicians (3 community-based, 2 academic-based) became aware and intrigued by wide variation within and between practices. Observed variation centered around the application of new recommendations such as those by the USPSTF. The group met with leaders from the Department of Family Medicine to discover ways to better understand, and when appropriate address practice variation and potential gaps. A learning collaborative model was adopted.18,19 The collaborative would provide an interactive, inclusive experience that would not only disseminate information, but allow peer-to-peer learning and leverage the collective experience of its members. The goal of the collaborative was to ensure all members were aware of selected recommendations and through shared experiences place them into context for their own practices. Over the first 3 years the years the collaborative continually evolved. For example, changes were made in response to member feedback to include more topical information within the surveys and expand the discussion sent with the results. The SARS-CoV-2 pandemic prompted greater information sharing outside the survey process to help members stay abreast of information not available on the system’s intranet. This is a description of a primary care learning collaborative in a large health system.
Methods
The Primary Care Learning Collaborative
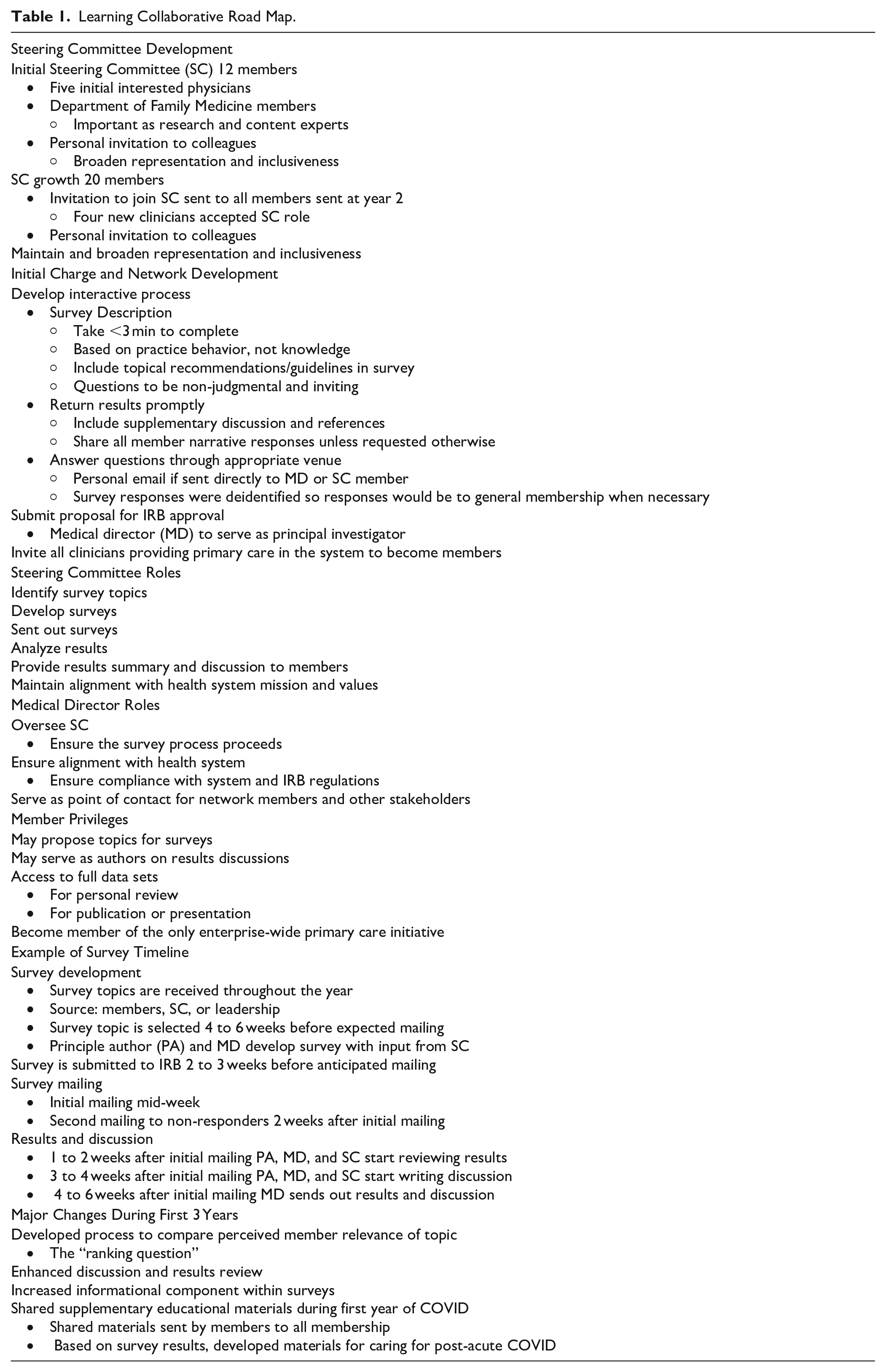
The collaborative resides within a large health system that covers five states including Arizona, Florida, Iowa, Minnesota, and Wisconsin. All share the same electronic health record and intranet. The system houses a medical school and postgraduate programs including family medicine, pediatrics, and internal medicine. The Department of Family Medicine (DFM) agreed to provide infrastructure support and facilitate the development process. A roadmap outlining the collaborative development and process is shown in Table 1. The initial steps were to identify a steering committee (SC) and a medical director. The SC was recruited through personal invitation of known colleagues and through the initial survey with the intention of creating broad representation and diversity. The SC was charged with developing the process, with the medical director taking on responsibility as the principal investigator. It became the responsibility of the SC to identify survey topics, develop and send the surveys, analyze and deliver results, and provide a summary with discussion to members. The role of the medical director was to oversee these activities, serve as the point of contact for collaborative members and interested stakeholders outside the network, ensure compliance with IRB regulations, and maintain alignment with the health system’s values. The initial SC was 12 members and represented all states and included family medicine, primary care internal medicine, primary care pediatrics, nurse practitioners, physicians, and physician assistants. To increase representation after 2 years the SC expanded to 20 members. Participation in the SC was voluntary. In June 2017 the initial email invitation to become a member of the health system’s primary care learning collaborative was sent to 506 primary care clinicians identified from department (family medicine, general internal medicine, general pediatrics) lists, trying to include as many of the system’s clinicians practicing in any outpatient primary care setting as possible. Membership enabled participants to propose survey topics, provided avenues for feedback to practice leadership, created opportunities for benchmarking peers, and to belong to the only systemwide group of practicing primary care clinicians. In July 2019, using an expanded distribution list, 851 primary care clinicians providing any outpatient care were again sent an invitation to promote expanded participation. Both invitations requested completion of a personal and practice demographic survey from participants. Topical surveys were only mailed to members who agreed to participate through the demographics survey. All survey results were deidentified.
Learning Collaborative Road Map.
Surveys
A survey-based collaborative was chosen as the interactive tool to allow participation by busy primary care clinicians; something they could fill out quickly and easily. Based on the steering committee’s previous experience, surveys would be brief, interactive, relevant, informative, inclusive, and allow 360-degree communication-survey with supplementary information sent, receive responses, and promptly return results. Any direct emails to the medical director were answered promptly. Questions generally focused on practice behaviors, not subject knowledge. Examples are shown in Table 2. To ensure appropriate oversight and to utilize the system’s internal survey system, a version of RedCap, all surveys were approved by the Mayo Clinic Institutional Review Board (IRB). IRB review is required for surveys using RedCap.
Selected Survey Questions.

Survey topics were generated from collaborative members, SC members, and system leadership. There was an attempt to select topics that were between early adaptation and widespread implementation or when wide practice variation was expected. 20 In the first 3.5 years there were 18 surveys on clinical or practice management. Surveys were sent via email 6 to 8 times a year, took less than 3 min to complete, and results were communicated to participants in less than 6 weeks from survey closure. The results report included a brief summary, expanded discussion, access to the raw data and often a link to supporting materials. Communication from members occurred within the survey (anonymously) or through the medical director if the member wanted a direct response. All surveys provided respondents the opportunity to add comments which were shared with the collaborative membership unless the writer indicated a preference otherwise. To create better context around the topic, beginning with the fifth survey, we introduced a ranking question addressing the acceptability of practice variation ranked from 1 (variation acceptable) to 10 (consistency important). Question examples are shown in Table 2.
During the second year a survey was sent to better understand the value of the survey components. Respondents were asked to rate each component as useful, somewhat useful, slightly useful, or not useful.
Expanded Communications
Throughout the COVID-19 pandemic in response to changing clinical and personal demands the SC developed additional communications with members. Personal concerns were shared anonymously with appropriate leadership. In the early months of the pandemic the health system posted regularly updated material on the systems website. Even so, rapidly changing information on a variety of subjects left knowledge gaps members would obtain through various methods they would then share with steering committee members. In the spirit of information sharing, this would then be shared with all members when appropriate in separate communications outside the usual survey process. Later in the pandemic, with a paucity of information but an ever-expanding need for addressing post-COVID care, the network again initiated vigorous information sharing on the evaluation and management of those recovering from acute COVID-19.
Statistical Analysis
For the ranking questions median rankings were used rather than means because the data was non-normal and skewed. 21 The 95% intervals were estimated for each median using resampling methods.22,23 Non-parametric resampling methods were used because the rankings were integers not continuous numbers and the data lacked normality. For the resampling, 2000 iterations were done. During each iteration, the ratings provided for each item were resampled to obtain the median and confidence interval. We used R, version 4.0.2 (R Core Team 2020) for all analysis. 24
Results
Results of the 2 demographic surveys are shown in Table 3. In the 2017, 24.7% of invited clinicians elected to participate in the learning collaborative, while in 2019 23.7% participated. The second demographic survey identified more primary care clinicians and more responded from internal medicine (5.6%-18.3%), nurse practitioners (13.6%-24.8%), and women (49.6%-64.7%). Starting in 2019 members of the collaborative were more likely female (65%-57%) and physicians rather than NP/PS’s (64%-57%) when compared to the system’s family medicine clinicians. 25 Respondents of the second survey were more likely to practice in a rural community (12%-21.8%), provide outpatient only care (43%-68%), and provide obstetrical care (21.4%-34.2%).
Primary Care Learning Collaborative Member Demographics July 2017 and July 2019.

Between July 2017 and November 2020 18 topical surveys were sent. Of the 18 surveys, 7 related to USPSTF recommendations, 6 on clinical management, 3 on national guidelines, and 2 on practice management. Overall participation by the learning collaborative in the topical surveys was 1221/2470 (49.4%) with individual survey participation varying from 38.8% to 70.6%. Thirteen percent of individuals completed greater than 85% (11 completed all) and 12% completed less than 15% (4 completed 0) of the surveys.
Inter practice variation was noted throughout most surveys. Some of this is reflected in the written responses with examples shown in Table 4. With the additional ranking question (examples of ranking questions in Table 2) members expressed an expectation for the most consistency and the least variation in practice related to COVID-19 public health management and opioid prescribing. For diabetic guidelines, lipid screening guidelines, fluoride treatment, and adult ADHD they accepted more variation (Figure 1) compared to the other topics.
Selected Survey Results. A. Selected Narrative responses. B. Assessment of Learning Collaborative Elements. C. New or Increased Clinical Problems During COVID Pandemic Surge.


Relative rankings of acceptable variation versus consistency by topic. Respondents’ perception of criticality of variation in care related to survey topic.
A survey to assess the perceived usefulness of the process/survey components was sent after the second year. Results are shown in Table 4. Of 51 respondents, 46 (90%) found at least one of the components useful. Eighty-four percent found topical information sent with the first survey the most useful followed by the brief summary with discussion, 82%. This survey had the lowest response rate of all surveys (44%).
The collaborative continuously evolved. The ranking question was added starting with the fifth survey. The recommendations and information related to the topics under review were initially sent with the results, but progressively more information or links were sent within the survey. The discussion sent with the results was expanded and better referenced.
During the pandemic, there were 2 surveys over the first 9 months. A survey in May 2020 addressed both personal and clinical concerns. Personal concerns were shared anonymously with system leadership in real time. The survey also identified common practice concerns where information was limited. Members shared experience and identified resources which were passed along to all members. A survey in November 2020 identified all primary care clinicians were caring for post-acute COVID patients and a growing number of patients with new or worsened mental health problems. (Table 4). At the time information to address these issues was scare so the SC developed and shared related educational materials with members.
During the first 3.5 years of the collaborative over 50 clinicians and scientists participated in survey development, results discussion authorship, or presentations at academic venues including international meetings. Hundreds of emails have been exchanged across the country not only in the development and dissemination of the process, but by members reaching out with question, comments, and providing input.
Discussion
This is a description of the development and evolution of a learning collaborative of primary care clinicians in a single health system across disparate geographic regions. All participants were in the same health system, but practiced in a wide variety of communities, in a diversity of practices, with varying practice demands and resources. It was initially developed over concerns of practice variation in the adoption of USPSTF recommendations. It expanded to include a range of topics including disease specific guidelines and practice management. The original motivation for developing the learning collaborative was to identify broadly applicable topics thought important and allow members to collectively place them in a contextual framework relevant to their practices. It sought to function as a primary care learning collaborative and in doing so, develop a sense of community among primary care clinicians within the health system. 20
Selection of appropriate topics was successful overall based on member feedback and participation. Topic or survey ideas were submitted from a variety of sources. The SC provided most of the ideas initially, but as members understood the process, they contributed most of the topics for later surveys. When the number of requests exceeded the number of surveys, by merging topics or including 1 to 2 supplementary questions in a survey, most requests could be accommodated.
The collaborative was able to help members gage the relevance of the topic to their practice. This was done in 3 ways. First, the questions were behavior-based, that is, “What are you doing . . .?” providing members insight into their peers’ practices. Second, narrative responses provided rich, honest feedback, and deeper insight. Despite the design as a quick “point and click” survey process, this narrative response was robust and grew. Absolute participation varied across surveys, but frequently members spent the time and effort to write 60 to 100-word responses. Finally, the ranking questions generated member interest in the results while providing stratification of their peer’s perception.
Several trends were identified over the first 3.5 years of the collaborative as shown in Figure 1. When applying practice elements to public health crises such as the COVID pandemic or opioid epidemic, little variation was deemed appropriate. Applying USPSTF or system practice management principles, slightly more variation was viewed as acceptable. When implementing clinical guidelines greater variation and perhaps more customization was tolerated or even expected. The ranking question, though not a validated instrument, was a simple method to provide the SC and members with feedback about the relative tolerance for variation in care when adopting or implementing new or changing recommendations.
As a grassroots initiative, it was a “bottom-up” collaborative, run by members with infrastructure support from the DFM. Most of the SC and over 80% of the members were community-based, not academic-based clinicians. This ensured the collaborative would remain sensitive to members priorities and stay open to input from members.
The COVID pandemic disrupted all aspect of life, including medical education.26-28 During the first several months of the COVID pandemic using the quick turnaround process certain patterns emerged. Most notably, the need to address those with post-acute COVID illness, a problem seen by most primary care clinicians in this group (Table 4). At the time there was a paucity of information for caring for those post-acute COVID, for example the NIH guidelines on the care of those with SARS-CoV-2 contained a single paragraph in a 250-page report. The network identified and shared information among themselves. 29 Likewise, the mental health crisis identified throughout 2021 by national organizations was apparent within collaborative practices in 2020. 30 Although the collaborative lacked the resources to address the clinical needs brought on by the crisis, could provide an awareness and validation of members’ experiences.
There were limitations to the generalizability of this project. It was a review of a collaborative within a single healthcare system. Although involvement of the SC and members was voluntary additional resource availability included access to an IRB, intranet survey system, library, and infrastructure support from an academic department. Membership of the collaborative was not representative of primary care clinicians nationally; members were more likely to be female, younger, and Caucasian-Non-Hispanic since most members were clinicians practicing in small cities or rural upper Midwest. 31 The largest demographic, family physicians, (81, 41.5%), were more likely to practice obstetrics than their peers nationally (27% vs 18%). 31 The instruments used in surveys themselves, the ranking questions, and the survey assessment were all unvalidated. Even so, the process was expected to be subjective and generate dialog. The collaborative was designed to share knowledge, experience, and collegiality, not to be objective research. Responses were based on self-reported practice behavior, a source of bias.32,33
This project demonstrated primary care clinicians in a large health system will participate and find value in a primary care learning collaborative. Although neither the project nor this study had the resources to support practice change initiatives or review whether these activities created practice change, it provided early building blocks to increase clinician awareness.34,35 Future growth and success will require the collaborative to facilitate not only information exchange, but practice change and the ability to measure that change without disrupting the current collegial process. While part of a single health system, the ability of the collaborative to reach across a diversity of practices suggests the principals applied here could be adopted among other primary care groups.8,18,36 The collaborative achieved early success for many reasons, among them inclusivity, strong identification with community-based clinicians, and an intentionally diverse SC. While many academic departments struggle to engage physicians in their communities with scholarly activity, those associated with this collaborative were able to do so. This was through listening and supporting the members. It succeeded through the goodwill, time, and efforts of the SC members. But most importantly it was the members that made the collaborative successful. Collectively they generously gave hours of their time on each topic for the betterment of their colleagues. This project demonstrates that a group of primary care clinicians dedicated to their practices, colleagues, and especially their patients will work together for the benefit of those they serve.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.