
Abstract
Introduction:
Australia has one of the highest rates of obesity in the developed world. In response to increasing rates of overweight and obesity in rural Australia, one regional primary health network commissioned the development of a multi-faceted weight and lifestyle management program, addressing nutrition, physical activity, and psychological approaches to behavioral change. This study evaluated the success of the program that was implemented in multiple general practices within regional New South Wales.
Methods:
De-identified data were received from 16 general practices that participated in the Murrumbidgee Lifestyle and Weight Management Program (MLWMP). Patient weight outcome and functional status measures were determined using descriptive statistics (SPSS).
Results:
Mean body mass index (BMI) of the 1217 participants was 37.4 kg/m2 and 75% of participants were female. Almost 40% of participants who had a BMI ≥ 40 kg/m2 had been diagnosed with a mental health condition. Upon completion of the program at 6 months, participants had lost an average of 3.2 kg. Over 31% of participants had lost at least 5% of their initial weight and 40% had reduced their waist circumference by at least 5 cm. Overall health and functional status measures were significantly higher upon program completion. There were significant improvements in quality of life measures regardless of level of weight loss during the program.
Conclusions:
The MLWMP, implemented in general practices within rural and regional Australia, had positive effects on both practices and participants demonstrating the value of intervention programs in primary care. Participants achieved a modest reduction in BMI, waist circumference, and weight. Further work is needed to determine the longer-term success of the program.
Keywords
Introduction
Australia has one of the highest rates of obesity in the developed world, ranking fifth out of 23 countries with available data, and the proportion of Australian people aged ≥15 years with obesity (30%) was higher than the overall average (24%). 1 Rates of overweight and obesity are increasing in Australia, from 56% in 1995 to 61% in 2007/2008 2 and to 67% in 2017/2018. 3 In 2017/2018, a greater proportion of men aged 18 years and over were overweight or obese than women (74.5% and 59.7% respectively). 3 Obesity is particularly a problem in rural areas, with a greater proportion of overweight or obese adults living in inner regional, outer regional, and remote (72%) areas compared with major cities (65%). 3
A systematic review of international evidence-based guidelines on the management of overweight and obesity in primary care concluded that multifactorial programs of at least 6 to 12 months that include calorie intake, physical activities, and measures to support behavior change should be used with body mass index (BMI) as a routine measure. 4 Both general practitioners (GPs)5,6 and their patients 7 feel that primary care has a role in weight management. Despite this, it has been suggested that obesity is under-managed in general practice both in Australia and internationally8-10 suggesting a need to support GPs to improve obesity management.
Murrumbidgee Primary Health Network (MPHN) is a regional PHN in south-western NSW servicing almost 250 000 people where a greater proportion of the population (61.7%) is overweight or obese than the state average (50.5%). 11 The MPHN commissioned a local provider to co-design and implement the Murrumbidgee Lifestyle and Weight Management Program (MLWMP). Social cognitive theory (SCT), used in the development of the program, suggests a multifaceted causal structure for behavior, in which beliefs about self-efficacy interact with the ability to develop personal goals and outcome expectations while recognizing both environmental barriers and facilitators of behavior. 12 Setting goals for behavior change and self-monitoring with detailed records of food intake, physical activity, and body weight have been recognized as key components in behavioral management of obesity. 13 The MLWMP involved a multi-component approach addressing nutrition, physical activity and psychological approaches to behavioral change and upskilling of general practice teams by a health-coaching expert. In session 1 of the 5 sessions, participants were given a workbook containing information on how to set personal goals for activity and diet and included information on food diaries. There was also discussion about a wellness wheel that allowed participants to consider how they balanced areas of their lives and which areas (ie, “weight,” “happiness,” “fun,” “fitness”) needed attention. Subsequent sessions provided motivational interviewing and review of progress toward goals as well as dietary/nutrition information, such as “reading nutrition labels” and exploring barriers to change and how to address these in session 3 and review of “lifetime goals” in session 5.
Resources included a wellness wheel, used to support behavioral change by allowing self-exploration of choices and situations that impact on overall wellness, current satisfaction, and short and long-term goals. Dartmouth COOP Functional Health Assessment Charts-World Organization of Family Doctors charts (hereafter called COOP-WONCA charts) were used to explore changes in functional status of participants as they have been shown to be an easy to use measure of functional status. 14 Charts were modified to use a 4-week rather than 2-week recall period due to the longer, 3-month, duration between measures and the length of the program. This study aimed to evaluate the success of the program implemented within multiple general practices in the south-west region of NSW.
Methods
General practices within the MPHN were invited to apply for a grant to fund their participation in a primary care based intervention (MLWMP) for obesity management. The PHN aimed to improve access to weight management and lifestyle programs for general practice patients who were identified as overweight or obese, and particularly those who were from a low socio-economic background and/or had a mental health condition. Having a government-issued concession card to reduce healthcare costs was used as a surrogate marker for having a low socioeconomic background in this study.
LiveBetter Community Services was contracted to provide face-to-face support with the practices via practice visits, teleconferences, webinars, and training workshops. This support was provided by allied health staff, predominantly dietitians. The funding supported 16 rural and regional practices to upskill staff and enroll patients between May 2017 and December 2019 with a BMI > 30 kg/m2 to participate in 5 sessions over a 6-month time-frame and to provide quarterly de-identified data (until July 2020) to the PHN to enable program evaluation by independent researchers (named authors).
The study used a mixed methods research design, separately analyzing quantitative and qualitative data, then integrating the results in the interpretation. Weight, waist circumference, and blood pressure were measured at each session by practice nurses and deidentified data were supplied to researchers. A specific duration was not set for sessions, and ranged from 20 to 60 min. BMI was calculated by dividing patient weight (kg) by the square of their height (m2). Individual practices managed recruitment of patients. Recruitment methods included GP or practice nurse recommendation of the program to the patient and waiting room posters. While the program was delivered by members of the general practice team in each practice, there was both individual and group support from allied health staff such as dieticians, exercise physiologists, and psychologists. Availability of this allied health support varied with the location of the practice. While a number of the larger practices enlisted the support of either a dietician or an exercise physiologist most relied on general practitioner or nurse practitioners skills to provide sessions.
Interviews were undertaken with 12 general practice staff (2 GPs, 9 nurses, and 1 practice manager) who participated in the program to explore their views on the development, implementation, and sustainability of the program. Their views on barriers to weight loss were not a focus of the study, although some were raised. Qualitative interview data were audio-recorded and transcribed. Two researchers independently reviewed the transcripts to identify common themes.
Quantitative data were analyzed using SPSS (v25) and an alpha of P < .05. Descriptive statistics plus Pearson’s chi-square were used to describe patient characteristics and patient weight loss outcomes were analyzed via Student’s independent t-tests, one-way analysis of variance (ANOVA) and paired t-tests to compare weights between 2 sessions. For multiple sessions, repeated measures ANOVA was used with a Greenhouse-Geisser correction and a Bonferroni adjustment for multiple comparisons. Functional status and quality of life of participants were explored using COOP-WONCA charts. Functional components of the COOP-WONCA charts include overall health/quality of life, daily activities, physical fitness, feelings, social activities, and change in health. 14 Functional measures were analyzed via Wilcoxon signed ranks test. In the event that participants selected a midpoint between 2 choices or 2 adjacent values, the higher value (worse score) was utilized for analysis. This was consistent for both the initial and 3-month (session 4) COOP-WONCA charts. Patients who appeared to have repeated the program were counted as new patients. Ethics approval was granted by The University of Notre Dame Australia Human Research Ethics Committee.
Results
Patient Weight Outcome Measures
Of the 1217 participants who attended session 1, three-quarters were female. Age ranged from 16 to 89 years (mean 53.3 years [standard deviation (SD) 15.7]). Almost 6% of participants were aged ≥75 years and 5% of were of Aboriginal descent (First Nations). More than 40% (42.8%) of engaged patients were concession card holders and almost 30% of engaged patients had a previous diagnosis of a mental health condition.
BMI of participants at session 1 ranged from 23.1 to 80.0 kg/m2, with a mean of 37.4 kg/m2 (SD 6.5). Around 6% (6.3%) of patients had a BMI < 30 and two thirds of patients had a BMI of 30 to 34.9 (33.6%) or 35 to 39.9 (33.6%). More than a quarter of participants had a BMI > 40 kg/m2 and 11.5% had a BMI > 45 kg/m2. There was a significant negative correlation between age and BMI (Pearson’s r = −.164, P < .001). Concession card holders had a higher mean BMI than those without a concession card (BMI of 38.1 [95% CI 37.5-38.7] vs 36.7 [95% CI 36.3-37.1], t(971.2) = −3.632, P < .001). Waist circumference at session 1 ranged from 71 to 176 cm. Mean waist circumference for male participants (122.5 cm [95% CI 121.0-123.9]) was higher than the mean waist circumference for female participants (111.1 cm [95% CI 110.2-112-1], t(1166) = 12.300, P < .001).
The mean BMI for participants with a mental health condition was 38.6 kg/m2 (95% CI 37.9-39.3), significantly higher than those without such a diagnosis (36.8 kg/m2 [95% CI 36.4-37.2], t(596) = −4.310, P < .001). With increasing BMI category, significantly more participants had been diagnosed with mental health conditions (χ2(4) = 24.468, P < .001). Only 17.3% of patients with a BMI < 30 kg/m2 had been diagnosed with a mental health condition versus almost 40% of participants with a BMI ≥ 40 kg/m2.
Attendance at sessions decreased over time. Almost 72% of patients attended session 3 and 52% attended session 4. Overall, 36.9% of patients completed the program (attended session 5 of the program at 6 months after the initial session). Overall, 41.5% (n = 214/516) of patients with a concession card and 36.0% (n = 128/356) of patients diagnosed with a mental health condition completed the program.
There was a reduction in weight between each session for all participants who attended (Figure 1). Overall, mean weight decreased from 103.3 kg (95% CI 102.1-104.5) at session 1 to 98.6 kg (95% CI 96.7-100.5) at session 5. This reduction was significant for all pair-wise comparisons of sessions other than for between sessions 4 and 5 (Table 1). However, when per cent weight loss was calculated, there was a significant reduction in weight loss (%) between all session pairs including sessions 4 and 5 (Table 2, Figure 2). Of the 449 participants who completed the program, 31.4% had lost at least 5% of their initial body weight. Participants lost 1671.7 kg, however, there was a 254.3 kg gain so the net weight loss was 1417.4 kg overall, an average of 3.2 kg per participant who completed the program. There was no association between weight loss and gender, concession card status or presence of a diagnosed mental health condition. There was also no difference in weight loss (%) by initial BMI categories.

Mean weight at all 5 sessions and the number of participants who attended each session.
Comparison of Participant Weight at All Sessions.

Abbreviations: SD, standard deviation; SE, standard error.
Weight Loss (%) at Each Session.

Abbreviations: SD, standard deviation; SE, standard error.
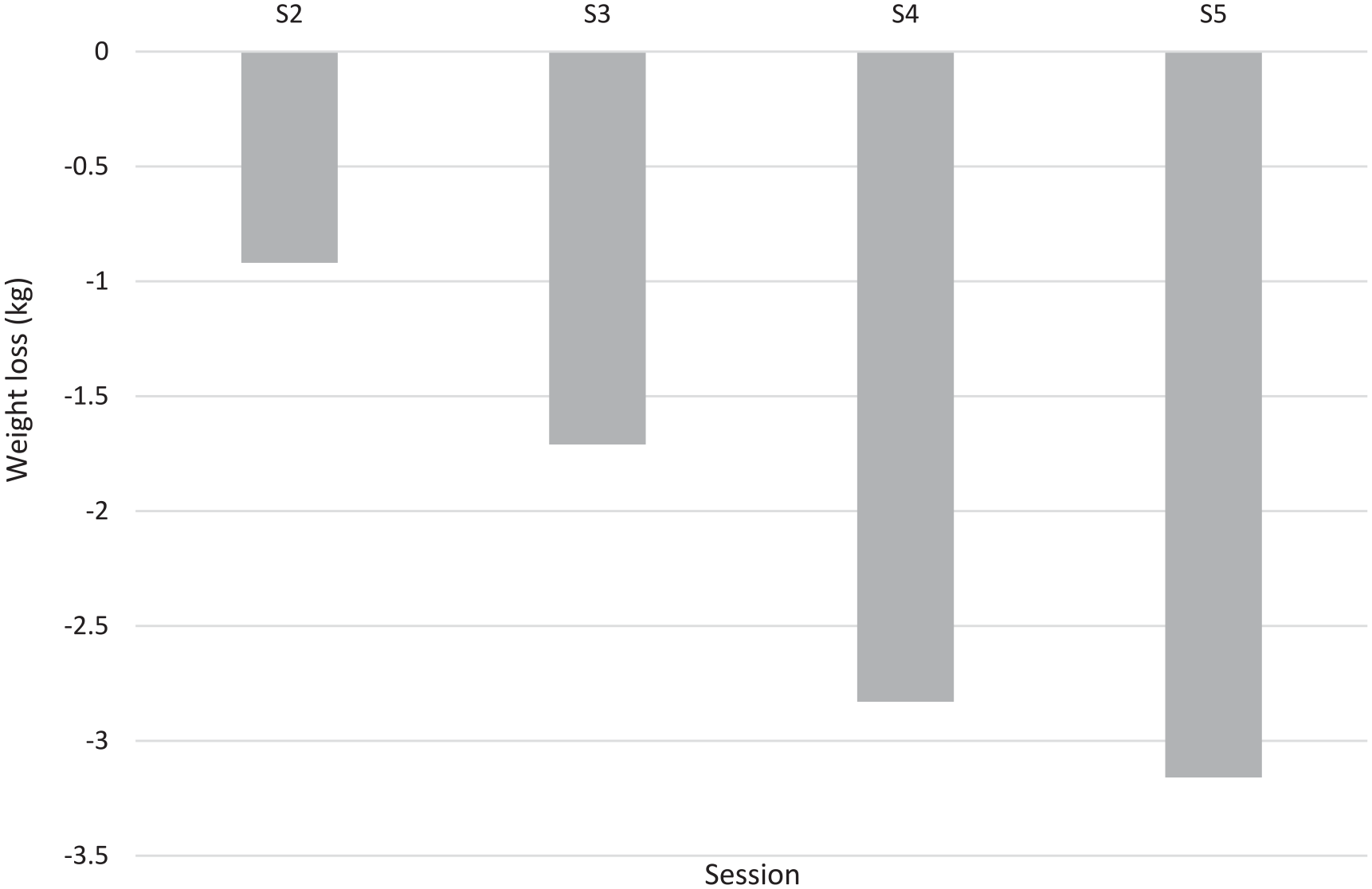
Mean weight loss (%) across all sessions for participants who completed the program.
Mean waist circumference at session 5 was 109.4 cm (95% CI 108.0-110.7), significantly less than mean waist circumference of all participants at session 1 (114.0 cm [95% CI 113.2-114.8], P < .001). There was a significant reduction in mean waist circumference across all sessions (P < .001) other than for between sessions 4 and 5 (P = .067) (Table 3). Upon completion of the program, change in waist circumference ranged from a loss of 32.5 cm to a gain of 13.5 cm. Overall, 40% of participants who completed the program had reduced their waist circumference by at least 5 cm and 11% had lost at least 10 cm. A total of 1818 cm were lost, however, there was a gain of 280.3 cm. Net reduction in waist circumference was 1537.7 cm, a mean loss of 3.7 cm per participant who completed the program. Participants with a diagnosed mental health condition lost less waist circumference than patients without such a condition (−2.6 cm [95% CI −3.6 to −1.7] vs −4.0 cm [95% CI −4.6 to −3.3], t(416) = −2.205, P = .028).
Mean Waist Circumference of Participants at All Sessions.
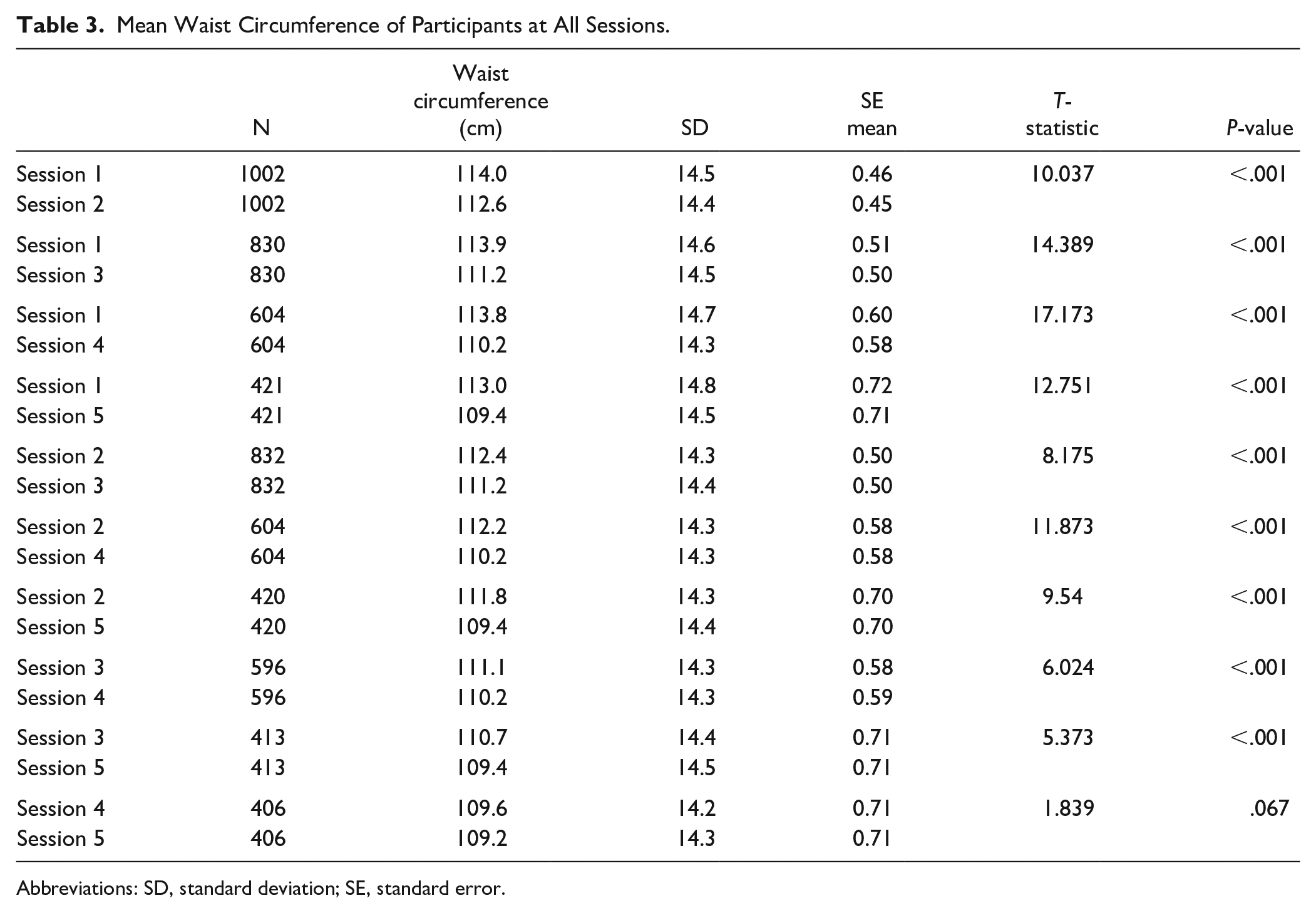
Abbreviations: SD, standard deviation; SE, standard error.
Functional Status Measures
Participants’ functional status was assessed using COOP-WONCA charts at the initial assessment and again at 3 months. Over 17% of participants reported that they had much difficulty or could not do their usual indoor and outdoor activities because of their physical and emotional health at initial assessment and 26.7% of participants reported that their emotional problems had bothered them quite a bit/extremely during the prior 4 weeks. In addition, more than half the participants (52.7%) reported that the hardest physical activity they could do for at least 2 min was light or very light.
However, at session 4, 70% of participants reported they could do moderate exercise (43.3%), heavy exercise (21.4%) or very heavy physical exercise (5.3%). There were improvements in all components of COOP-WONCA between the initial and 3-month visits (P < .001 for all components other than social activities where P = .006, Table 4). Of the 210 participants who had completed COOP-WONCA charts for both sessions 1 and 4, reported physical fitness at session 4 was the same (n = 80; 38.1%) or better (n = 100; 47.6%) than at session 1. At session 1, when patients were asked to rate their overall health now compared to 4 weeks ago (“change in health”), the majority said about the same (59.5%) or worse (15.2%) (Figure 3). However, at session 4 more than two thirds reported that they felt a little better (35.1%) or much better (32.7%).
Improvements in Functional Components Between Sessions 1 and 4.

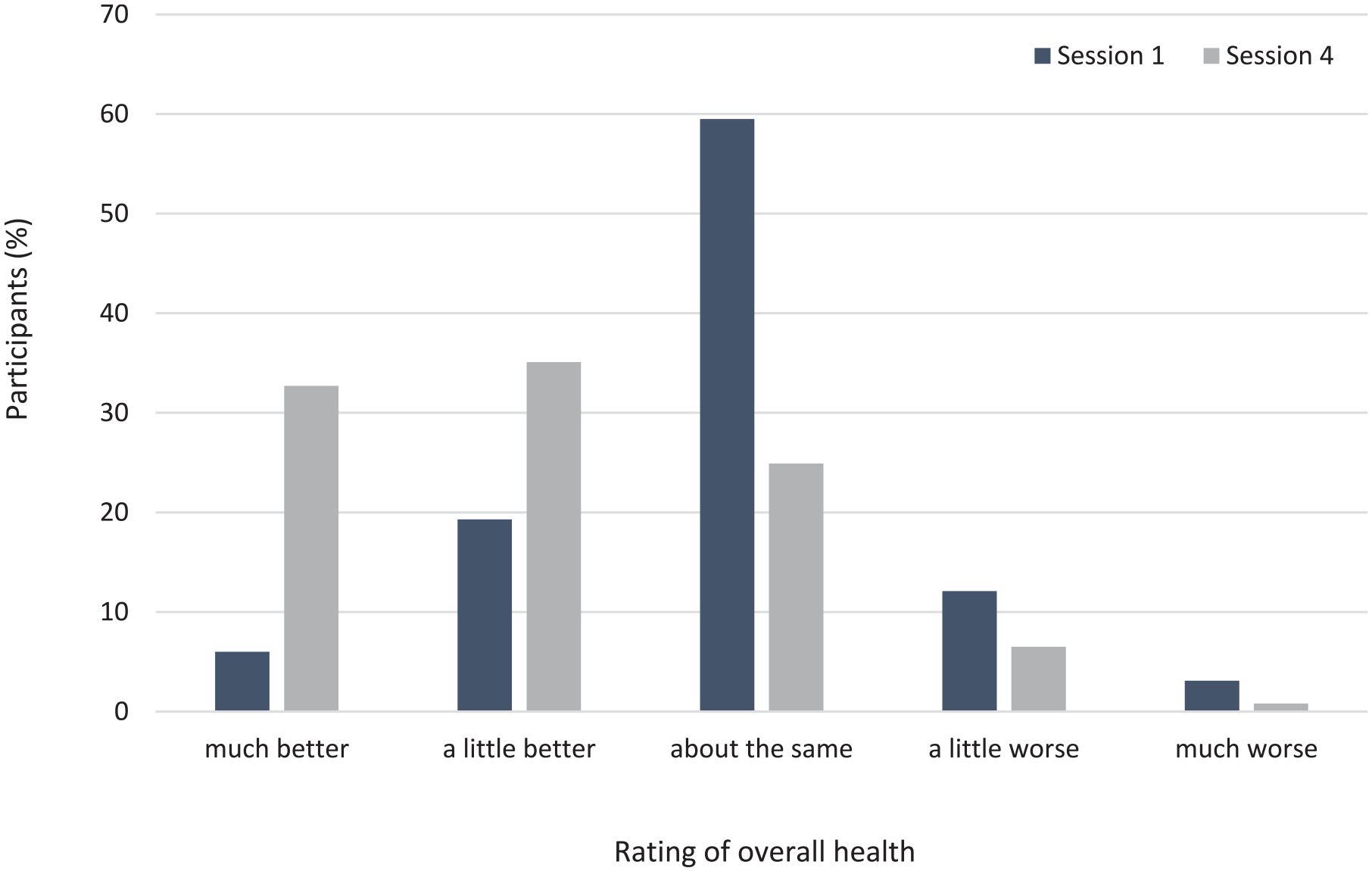
Reported rating of overall health at initial assessment and at 3-month visit relative to their health in the prior 4 weeks.
Staff Interviews
MPHN provided primary care practices with written resources for the program, mandated number of sessions and that those conducting program should attend training including motivational interview techniques. However, there was flexibility within the program for practices to modify their approach. Practice education and support in motivational interviewing was seen as particularly useful, as was the “opportunity to identify existing barriers.” It was “a good opportunity to discuss how we are currently doing things” and it provided an opportunity to share ideas about barriers and possible ways to overcome them.
Staff responsible for implementation were chosen by individual practices. Predominantly practice staff interviewed identified GPs as responsible “motivating and identifying participants”; the doctors “make the decision about who should join the program and then the nurses ran it,” the nurses did “the on-ground stuff.” The practice nurses were also seen as being able to “encourage involvement” and to have time to allow patients to “feel a bit more comfortable” in discussing difficult issues. There was perceived value in having the continuity of 1 person dedicated to the program to allow building of trust and rapport.
The practice staff interviewed considered rural workforce shortages, meaning that GPs were “time poor,” as a challenge to implementation of the program. They also identified variable support from individual practice staff, some skeptical about potential for success of weight management programs. Getting the program up and running was initially quite labor intensive, a potential barrier that improved with staff familiarity with the program. As 1 practice nurse said: “the challenges have again been primarily in time, specifically nursing time. Particularly because of patient contact time. But as the process becomes more embedded I think that it will become easier.” Time was seen as an issue in several ways; nursing time, competing clinical roles, the time-intensive nature of the individual sessions and the capacity of the practice to manage the program within a busy workload. There was some “discomfort and reluctance” among staff, “who were a bit embarrassed doing waist circumference or having to weigh patients” particularly in staff who were over the recommended weight themselves. Barriers to weight loss, while not the primary focus of the interviews, were also raised. These included the increasingly sedentary population, TV advertising, and the need for flexible weight loss programs.
Discussion
Almost a third of participants in this program had lost at least 5% of their initial weight with an average weight loss of 3.2 kg for those who completed the program. A 5% to 10% reduction in weight can have substantial health benefits, improving cardiovascular disease risk factors 15 and diabetes risk. 16 Results from this study were similar to previous lifestyle interventions in primary care promoting behavioral change, 17 diet, and exercise. 18
Measures of functional status of participants significantly improved between the initial and 3-month visits, which suggested that the MLWMP had a positive impact on wellbeing, reinforcing the value of the program. Obesity has a negative impact on an individual’s health and wellbeing with healthcare complications, lower quality and length of life, and mental wellness issues. 19 Other research has found that despite some weight gain improvements in physical functioning, vitality and mental health can be maintained for at least 24 months after a 6-month intervention program. 20 These results highlight the importance of looking at functional status measures and not just weight loss when evaluating the success of lifestyle interventions.
This intervention encouraged the measurement of waist circumference, as well as BMI in general practice. In conjunction with BMI, waist circumference can indicate a person’s potential risk of developing chronic diseases such as heart disease and type 2 diabetes 3 and as such is a useful tool in general practice. In the current study, 4% of men and 2% of women had a waist circumference that fit within the World Health Organization guidelines of <102 cm in men and <88 cm in women. Higher measurements are associated with type 2 diabetes, high blood pressure and heart disease. 21 Half of the male participants and 55% of the female participants had an initial waist circumference that was ≥20 cm above this threshold. Upon completion of the program, the proportion of participants who were at least 20 cm above the threshold was reduced to 40% of male and 41% of female participants.
General practice is well-placed to be the first point of call in the health system for obesity management as they see 85% of the population, however more resources are needed to better support this role. 22 This program involved practice education and a structured weight management program, an approach that gives GPs more confidence when initiating conversations with patients. 23 The use of the wellness wheel and the COOP-WONCA charts were found to be helpful in assisting this structure. However, the resource-intensive nature of this intervention, which was supported by a practice grant from the PHN, was raised as a concern during practice staff interviews. For the program to be sustainable into the future funding models need to be considered.
Although the program did not collect data on co-morbidities, the high mean waist circumference in the study population suggests that it is likely that many participants in the MLWMP had co-morbidities. Some program costs could be covered by a GP Management Plan for a chronic condition (care plan) and a Team Care Arrangement. One challenge in relation to this is that those with obesity without a co-morbidity such as diabetes might not be eligible for a care plan. Even in the absence of co-morbidities, it is estimated that the health needs of obese patients are greater than non-obese patients. Using data from the Australian Diabetes, Obesity and Lifestyle study, it has been estimated that the annual total excess cost compared with normal weight people without diabetes was 26% for obesity alone and 46% for those with obesity and diabetes. 24 It has also been suggested that dieticians do not believe that 5 allied health appointments per year is adequate “to provide optimum care” for patients with this chronic condition and that Medicare rebates allowed insufficient time for initial consultation counseling. 25
While there were clear benefits in terms of mental and physical health for participants who completed the program, one limitation of this study in terms of measuring its transferability was patient selection. The general practices chose participants, possibly leading to a group more motivated to engage than the general population. Another limitation was the focus on individual behavior and not the obesogenic environment that supports high-energy intake and sedentary behavior. 26 In addition to motivating individual behavioral change, health professionals, may need to develop partnerships with professionals in other sections of society. 27 Finally, only 36.9% of participants completed the program. The characteristics of completers and non-completers were compared and it was found that fewer First Nations participants had completed the program (25%) versus non-First Nations participants (37.7%, P = .047). In addition, a greater proportion of participants who had concession cards completed the program (41.5% of concession card holders vs 33.5% of non-concession card holders, P = .005). On average, participants who completed the program were older than participants who did not complete (55.6 years vs 51.9 years, P < .001). Although there were some differences in characteristics of completers versus non-completers, none of these characteristics was associated with weight loss outcomes of those who completed the program.
While there is limited published research on rural weight loss programs, the results from the current study are consistent with those from the WellingTonne weight loss project based in rural NSW. Mean weight loss in this 12-week, all of community, population-based strategy was 3 kg, with only 23% of participants attending the final weigh-in, 28 which is comparable with the MLWMP. Both the MLWMP and the WellingTonne project reported that, although there was modest weight reduction, the changes in diet and physical activity, if sustained, could lead to significant health benefits. In contrast to the community-based program, general practice can provide ongoing support to patients and this setting may help make weight loss sustainable.
Conclusion
The MLWMP, implemented in general practices within rural and regional Australia, had positive effects on both practices and individual participants demonstrating the value of intervention programs in primary care. There was a trend toward improved recording of BMI and waist circumference over the course of the program in participating practices. In addition, there was a modest reduction in BMI, waist circumference, and weight comparable with other lifestyle-based weight management interventions. Upon completion of the program, almost one-third of participants had lost at least 5% of their initial weight and 40% had reduced their waist circumference by at least 5 cm. In addition, overall health and functional status measures were significantly higher at completion of the program, regardless of the level of weight loss participants achieved during the program. There was a strong sense that the program needed funding support to be sustainable. Those with obesity and comorbidities were covered by Medicare Chronic Disease GP Management Plan and Team Care arrangements. There was a need to treat obesity prior to development of co-morbidities. There was a suggestion that value needs to be placed on health promotion and payment for health promotion activities would allow such projects to self-fund. Further work is needed to determine the longer-term success of the program.
Footnotes
Acknowledgements
Implementation of this program and its evaluation has been made possible by funding from the Murrumbidgee Primary Health Network through the Australian governments’ PHN program. We would also like to acknowledge the contribution of LiveBettter Services, who helped co-design and implement the MLWMP, and Medicoach, the health coaching expert who upskilled the general practice terms, to the success of this program. Lastly, we would like to thank Dr Dianne Jonasson, Dr Georgina MacDonald, and Dr Jane Anderson-Wurf for conducting some of the interviews for this evaluation.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Although Narelle Mills is employed by the MPHN, she had no part in the data collation and analysis.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Implementation of this program and its evaluation has been made possible by funding from the Murrumbidgee Primary Health Network through the Australian governments’ PHN program.