
Abstract
Objective:
This study aimed to analyze the psychometric properties of a brief scale measuring intention to vaccinate against COVID-19 in a Peruvian sample in the context of the current pandemic.
Methods:
A cross-sectional and instrumental study was carried out. A total of 547 Peruvian citizens selected through non-probability convenience sampling participated. Considering existing theories of vaccination hesitancy, 12 items were proposed that evaluate the intention to vaccinate against COVID-19 and the internal structure was evaluated through exploratory and confirmatory factor analysis. Reliability was analyzed with the ordinal alpha coefficient.
Results:
The exploratory factor analysis yielded a structure of 2 oblique factors that explain 69% of the total variance and the items saturated between 0.52 and 0.97. The confirmatory factor analysis showed that, of 4 models analyzed, the fourth model that was composed of 6 items presented optimal indices of goodness-of-fit (X2 = 11.089, P = .197, CFI = 0.999, TLI = 0.999, RMSEA = 0.034 [IC 90%, 0.000-0.077], SRMR = 0.016). Reliability analysis through the ordinal alpha coefficient yielded that the brief scale of intention to vaccinate against COVID-19 has adequate internal consistency (α = .91).
Conclusions:
The brief scale of intention to vaccinate against COVID-19 presents adequate psychometric properties that demonstrate validity and reliability and can be used in future research and clinical practice.
Introduction
Since the end of 2019, the world has been facing the COVID-19 pandemic caused by SARS-CoV-2 (Severe Acute Respiratory Syndrome-Coronavirus 2), which to date (April 8, 2021) has affected more than 133 million people worldwide and caused more than 3 204 000 deaths. 1 Since the declaration of a global health emergency by the World Health Organization (WHO, situation report-10), in January 2020, 2 followed by the declaration of the global pandemic (WHO, situation report-51) 3 in an unprecedented worldwide scientific effort, 11 vaccines have received emergency use approval or full license. Currently, more than 84 countries are applying some of these vaccines in priority populations. 4 Vaccination against COVID-19 is considered one of the most effective strategies to control this global public health crisis, because it can increase immunity and protect the population from infections that could result in the need for intensive care. 5 Despite the importance of vaccination, some people are reluctant to get vaccinated. In fact, WHO considered vaccine hesitancy as one of the top 10 threats to public health in 2019. 6 The intention to get vaccinated is influenced by factors that modulate confidence in vaccines. Vaccine hesitancy is the result of uncertainty or mistrust in health systems, health professionals, 7 governance and political accountability, 8 and vaccine efficacy against COVID-19.9,10 Uncertainty surrounding the COVID-19 vaccine causes people to question the efficacy and hold negative attitudes toward vaccines, and therefore refuse vaccination.11,12 Reasons for rejection or hesitation become the main barrier to acceptance of receiving the COVID19 vaccine and increases the individual and collective risk of the disease. 13
Various studies were carried out in populations of different countries such as France and Italy, where the majority of respondents (75%) indicated the probability of accepting vaccination against COVID-19. 14 The Chinese population reported probably affirmative intention (54.6%), followed by a definite affirmative intention (28.7%), 15 while almost a third of American adults said they did not intend to accept a vaccine against COVID-19, due to concerns about safety, efficacy, and lack of financial resources. 16 Research has not yet been conducted to determine the intention to receive a vaccine against COVID-19 in the Peruvian population.
Peru is among the countries with the highest global mortality rates from COVID-19, which has led to estimating that life expectancy in this country has decreased during 2020 by more than 2 years. 17 The lack of financial resources, the poor health system, and recent scandals related to the misuse of COVID-19 vaccines 18 favored the progression of the pandemic and may have led to public distrust of COVID-19 vaccines.
Various theoretical models examine the psychological basis of vaccine hesitancy, helping to understand the behavior of the population toward vaccines. The “3 Cs” model highlights 3 categories: (1) complacency, which exists when the perception of disease risk is low and vaccination is not considered a preventive action; (2) convenience, which implies physical availability, affordability, and financial readiness, ability to understand (language and health literacy), geographic accessibility, quality of service, and the extent to which vaccination services are provided; (3) and confidence (a) in the efficacy and safety of vaccines, (b) the system that supplies them (health professionals and services), and (c) the motivations of the policy makers who decide on the necessary vaccines. 19 Additionally, based on the literature, a “4 Cs” model has been proposed, integrating the calculus as a rational degree in which individuals are involved before making a decision. 20 There is another model, that is “5 Cs,” which adds collective responsibility to previous models, such as the will to protect others through vaccination itself through collective immunity. 21 Likewise, the model of determinants of vaccine hesitancy organizes 3 domains: (a) contextual influence; (b) individual and group influence; and (c) vaccine and specific vaccination issues. 22
There are instruments in English versions that assess confidence in vaccination for students, 23 and some measure COVID-19 vaccination intent with the “5Cs” model 24 ; however, they do not report evidence of validity.12,25,26 Therefore, there is a need to develop valid and reliable instruments that measure the intention to vaccinate against COVID-19.
Therefore, the objective of this study is to evaluate the psychometric properties of a short scale that measures the intention to be vaccinated against COVID-19 among the general Peruvian population in the context of the current pandemic.
Materials and Methods
Type of Study
It is a cross-sectional and instrumental Study. 27 The psychometric properties of a short scale on the intention to get vaccinated against COVID-19 were analyzed in a Peruvian sample.
Participants
The study was developed in 2 stages: exploratory and confirmatory. For both stages, the minimum recommended sample size was 200 participants. This calculation was done using the online Statistical software 28 considering an anticipated effect size of 0.3, a statistical power of 0.95, a significance level of .05, 2 latent variables, and 12 observed variables.29,30 However, 207 people participated in the study in the exploratory stage and 340 people participated in the confirmatory stage. In total, there was a sample of 547 participants, all selected through a non-probability sampling for convenience. The sample consisted mostly of male participants (68.9%). There is a greater participation of people who come from the coast (51.9%) and mountains (41%) of Peru. The most frequent educational levels were university (48.3%), postgraduate (24.5%), and technical (16.5%). Regarding the religion professed by the participants, there is a greater participation of Catholics (56.3%) and Protestants (33.8%). More than half of the participants (54.5%) mentioned that they went to work despite the pandemic, while 23.4% used teleworking. The ages ranged from 12 to 75 years, and the average age was 38.1 (SD = 11.6).
Instrument
We considered items available from surveys on scales of attitude or intention to be vaccinated against influenza (H1N1) and swine flu31-33 and an Intention to Vaccinate Scale against COVID-19 (IVS-COV-19). A panel of 3 experts including health professionals evaluated and approved the content of 12 items based on the literature review. The final set (Appendix 1) included 6 positive items semantically organized in factor 1 that evaluate acceptance of the perception of risk (complacency) and availability toward the vaccine (convenience), for example, “I am willing to do anything to vaccinate against Covid-19”; and 6 negative items that semantically correspond to factor 2, which evaluate the risk factors from the point of view of confidence, degree of decision (calculation), and collective responsibility, for example, “I would do everything possible to avoid the vaccine”). The items contain Likert-type response scale options, with a maximum score of 7 points, where 1 = total disagreement and 7 = total agreement. Likewise, a panel of 3 experts evaluated and approved the content of the 12 items. In addition, to avoid ambiguities in the understanding of the items, a focus group was organized with 31 university students. Subsequently, the instrument was corrected and approved for execution by the researchers of this study.
Procedure
The study was approved by the ethics committee of the Universidad Peruana Unión. Participants accessed an online questionnaire elaborated on a Microsoft Forms form and was disseminated through social networks, such as Facebook and WhatsApp. Before answering the questions on the survey home page, the purpose of data collection and the objectives of the study were explained to them. Moreover, the participants were informed about the confidential use of the data collected and of their voluntary withdrawal from the process. Finally, electronic informed consent was obtained from the participants. Those who voluntarily agreed to participate and signed the informed consent were included in the study. It is estimated that the administration time of the questionnaire individually is 10 min. Data were collected during the months of May and June 2021 and were stored in a Microsoft Excel template.
Analysis of Data
The data were analyzed in 2 phases. Phase I consisted of exploratory factor analysis with a sample of 207 participants. Previously, a descriptive evaluation of the items was made through the coefficients of skewness and kurtosis (<1 in absolute value). Furthermore, a correlation analysis of the items with the total scale was made and the reliability of the items was estimated through the ordinal alpha coefficient (>.7). An analysis of the adequacy of the correlation matrix of the items was made through the Kaiser-Meyer-Olkin statistical test (KMO > .8) and Bartlett’s sphericity test (P < .05). Consequently, the exploratory factor analysis was done with a polychoric correlation matrix and it consisted of estimating the number of factors with the parallel analysis method. The factorial estimation of the items was carried out with the unweighted least squares (ULS) method with oblique promax rotation 34 and the items that presented factorial loads lower than 0.4 would be eliminated.
Phase II consisted of confirmatory factor analysis (CFA) using structural equation modeling (SEM). Four factorial models were evaluated; a first one-dimensional model composed of 12 items, a second two-dimensional model of 12 items, a third two-dimensional model of 8 items, and a fourth two-dimensional model of 6 items. These analyzes were performed using the Lavaan package and the R program (version 4.0.3). The weighted least squares estimation method with adjusted mean and variance (WLSMV) was used due to the fact that the items were ordinal and due to the differences in the variances. 35 To evaluate the fit of the structural models, goodness-of-fit indices were considered 36 ; such as the Comparative Fit Index (CFI) and the Tucker-Lewis Index (TLI), standardized root mean squared residual (SRMR) and the parameters for the root mean square error of approximation (RMSEA). In addition, the recommendations of Hu and Bentler 37 were considered, who argue that the value of the CFI and TLI should be greater than 0.95 and the RMSEA ≤ 0.08. The internal consistency of the scale was analyzed using the ordinal alpha coefficient (α > .8) with their respective confidence intervals (90% CI), where values from 0.70 to 0.80 are acceptable and values greater than 0.80 indicate high reliability.
Results
Descriptive Analysis of Items
Descriptive analyzes (Table 1) show that the means of the items fluctuate between 2.47 and 4.90, the ordinal coefficient alpha is high (ordinal α > .7) and the correlation coefficients of the items with the corrected total of the scale are above the acceptable level (>.3). The skewness coefficients are less than 1 in absolute value, however, there are items with kurtosis coefficients above 1, which is evidence that the data corresponding to the items do not present a univariate normal distribution.
Descriptive Scale of Intention to Get Vaccinated Against COVID-19 (12 Items).

Abbreviations: AC, asymmetry coefficient; K, Kurtosis coefficient; M, Mean; r-itc, corrected item-total correlations; SD, standard deviation; α, Ordinal alpha reliability coefficient (polychoric correlation matrix).
n = 207.
Correlational Analysis of the Items
The adequacy analyzes of the correlation matrix show that it is convenient to perform the exploratory factor analysis because the KMO test was higher than the recommended level (>.8) and Bartlett’s sphericity test was significant (P < .001) (Table 2).
Matrix of Polychoric Correlations.

KMO = 0.91, Bartlett’s test = 1846.5, df = 66, P < .001.
Exploratory Factor Analysis
These analyzes yielded a structure of 2 oblique factors that explain 69% of the total variance, where factor 1 and factor 2 explain 38% and 31% of the variance, respectively. The factorial loads of the items range between 0.52 and 0.97 and are higher than the minimum level required in this study (0.4). All items presented communality equal to or greater than 0.3 (Table 3).
Exploratory Factor Analysis of the Intention to Vaccinate Against COVID-19 Scale (12 Items).

Factor 1 = Acceptance, Factor 2 = Risk attitude, h2 = Communalities, u2 = Units, Total variance explained = 0.69 (Factor 1 = 0.38, Factor 2 = 0.31), KMO = 0.91, Bartlett’s test = 1846.545 (df = 66; P < .001).
Confirmatory Factor Analysis
The results of the confirmatory factor analysis of the 4 proposed models were carried out through the structural equation models (Table 4). In the first model, a one-dimensional structure composed of 12 items were proposed and acceptable goodness-of-fit indices were obtained, except for one (RMSEA = 0.193; 90% CI, 0.181-0.206). For the second model, a two-dimensional structure was proposed, where 6 positive items evaluate the first factor, and 6 negative items evaluate the second factor. Like the previous model, one index did not present an acceptable fit (RMSEA = 0.154; 90% CI, 0.141-0.167). A third two-dimensional model of 8 items was evaluated, because items 2 and 3 of factor 1 and items 11 and 12 of factor 2 were eliminated, obtaining adequate goodness-of-fit indices (CFI = 0.997, TLI = 0.996, SRMR = 0.023) and acceptable (RMSEA = 0.066; IC 90%, 0.042-0.090). In these 3 models evaluated, the probability that the difference in results was due to chance was less than the significance level established in the study (P < .05). However, a fourth two-dimensional model composed of 6 items was evaluated, because items 9 and 4 of factors 1 and 2, respectively, were eliminated. Confirmatory factor analysis for this model showed that all goodness-of-fit indices was optimal (X2 = 11.089, P = .197, CFI = 0.999, TLI = 0.999, RMSEA = 0.034 [90% CI, 0.000-0.077], SRMR = 0.016).
Goodness-of-Fit Indices for the Models of the Intention to Vaccinate Scale Against COVID-19.
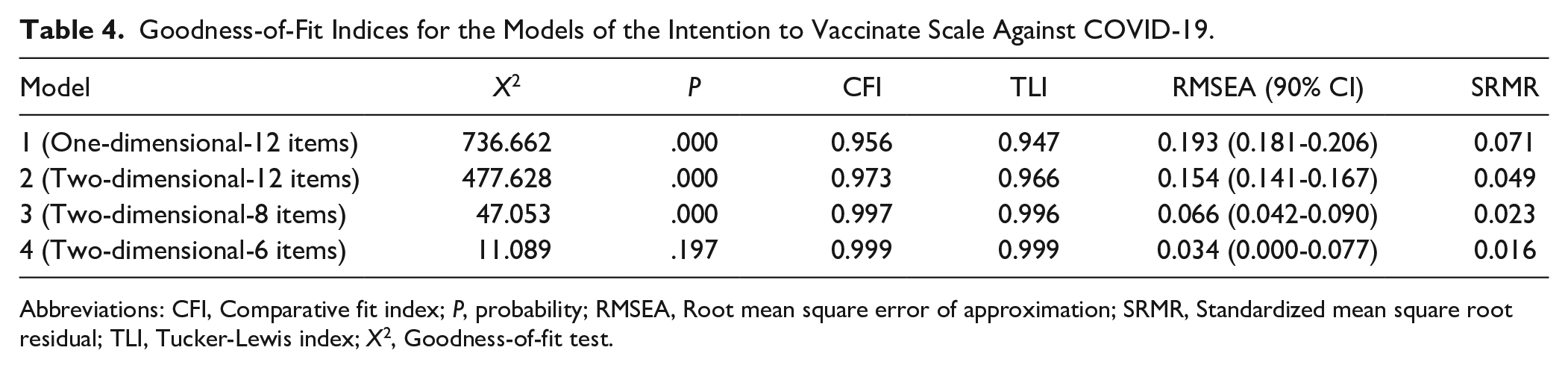
Abbreviations: CFI, Comparative fit index; P, probability; RMSEA, Root mean square error of approximation; SRMR, Standardized mean square root residual; TLI, Tucker-Lewis index; X2, Goodness-of-fit test.
Descriptives of the Intention to Vaccinate Scale Against COVID-19 (IVS-COV-19)
Table 5 presents the 6 valid items of the intention to vaccinate scale against COVID-19 obtained from the confirmatory factor analysis. This scale presents adequate psychometric properties (Figure 1), since the correlations of the items with the total scale are above .3 and the reliability coefficients are above .7 in all items.
Descriptive Scale of Intention to Get Vaccinated Against COVID-19 (6 Items).

Abbreviations: M, Mean; SD, Standard deviation; AC, Asymmetry coefficient; K, Kurtosis coefficient; r-itc, corrected item-total correlations; α, Ordinal alpha reliability coefficient.
n = 340, total α = 0.91, αF1 = 0.88, αF2 = 0.83.

Structural model of the confirmatory factor analysis of the COVID-19 vaccine intention scale (6 items).
Discussion
Vaccination is the appropriate method to prevent infection and reduce mortality, yet countries struggle with vaccine hesitancy. The purpose of this study was to develop a brief measure of intention to get vaccinated against COVID-19. The scale is designed to measure the behavior of acceptance or rejection of the COVID-19 vaccine in the Peruvian population. The results of this study provided initial support for the factor structure and reliability of the IVS-COV-19.
The results of the exploratory factor analysis present a two-dimensional structure: acceptance (6 items) and risk attitude (6 items). However, with confirmatory factor analysis, the scale was reduced to 6 items, preserving the two-factor structure. These results provide significant support for the various theoretical models that examine the psychological basis of vaccine hesitancy. 22 The IVS-COV-19 factors are important because they have connections to the vaccine hesitancy constructs and will allow a move toward a more complete understanding of the construct, primarily by supporting a more systematic study of vaccine intent among its components: compliance and convenience (acceptance factor); trust, calculation, and collective responsibility (risk attitude factor). 20 Although it does not fully encompass this theory, the items are consistent with it in the emphasis on acceptance and rejection of COVID-19 vaccines.
Among the strengths of the study, it is considered that unlike other scales that measure the intention to vaccinate against other diseases, this study developed this instrument considering factorial estimation methods used in psychometric studies, thus demonstrating its precision to measure the construct. On the other hand, the instrument developed in this study has ordinal items with 7 response points. This number of response options does not constitute a weakness in the study, although there is a tendency to develop scales with ordinal items with responses ranging from 4 to 5 points. There are studies that present instruments with measures of 5 to 10 points.23,38
Moreover, it is important to measure the components of vaccine acceptance and risk attitude separately, because it can be used as a tool with other constructs for diagnosis and to support the design and evaluation of clinical interventions. 39 The IVS-COV-19 is the only scale available in Spanish that is validated in the general population, and that can be used in cross-sectional and longitudinal studies.
The IVS-COV-19 may highlight the need for more research to explore why certain countries may experience sudden increases or decreases in confidence and vacillation in vaccines. EBIV-COV-19 factors were significantly correlated and provide support for the 6 items that assess the 2 dimensions related to vaccine intention. The internal consistency estimates for the 2 factors were solid, the total reliability estimates were sufficiently homogeneous (total α = .91), as well as the reliability of its dimensions (α factor 1 = .88, α factor 2 = .83). These results show that IVS-COV-19 is a promising instrument for evaluating vaccination intention.
In conclusion, this study provided initial evidence of good psychometric properties of IVS-COV-19. The instrument was developed as a brief measure of intention to vaccinate against COVID-19 and can be used in community and clinical settings. In addition, it can be used in future research related to the measurement of vaccine intent and its possible related factors.
Footnotes
Appendix
Scale of Intention to Get Vaccinated Against COVID-19.

| Items | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
|---|---|---|---|---|---|---|---|
| 1. I am willing to do anything to get vaccinated against Covid-19 | O | O | O | O | O | O | O |
| 2. I wish to immediately get vaccinated against Covid-19* | O | O | O | O | O | O | O |
| 3. I would do everything possible to get vaccinated against Covid-19* | O | O | O | O | O | O | O |
| 4. I don’t have time to get vaccinated against Covid-19* | O | O | O | O | O | O | O |
| 5. I am determined to get vaccinated against Covid-19 | O | O | O | O | O | O | O |
| 6. I would do my best to avoid the vaccine | O | O | O | O | O | O | O |
| 7. I have seriously thought about receiving the Covid-19 vaccine | O | O | O | O | O | O | O |
| 8. I think the Covid-19 vaccine is not safe | O | O | O | O | O | O | O |
| 9. I want to be vaccinated against Covid-19* | O | O | O | O | O | O | O |
| 10. I prefer to stay at home, rather than get vaccinated against Covid-19 | O | O | O | O | O | O | O |
| 11. I think I do not need to be vaccinated against Covid-19* | O | O | O | O | O | O | O |
| 12. I’m afraid of the Covid-19 vaccine* | O | O | O | O | O | O | O |
Items eliminated in the structural model of the scale by confirmatory factor analysis.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.