
Abstract
Identification of barriers to cancer screening among female migrant farmworkers is needed to inform intervention development and healthcare policy. Thus, our purpose was to systematically review and summarize findings from prior studies of barriers faced by Latinx migrant farmworkers in accessing cervical and breast cancer screenings in the US. Medline and Embase were used to identify literature through October 2021 using the search terms “migrant farmworkers AND. . .cancer; healthcare access; breast; cervical; federally qualified health centers,” and “migrant cancer screening” and “migrant farmworker cancer screening.” Snowball sampling by reviewing citations in each selected article was also used. Exclusion criteria included those articles that focused on specific types of cancer other than breast or cervical, those not within the US, not referencing Latinx migrants, not referencing cancer screening, or those focused on pediatric populations. Data was synthesized by 3 authors and selected articles were assessed for common themes. Nineteen articles met inclusion criteria. Common themes about barriers to cancer screening included: lack of cancer knowledge, cost/inability to pay, lack of health insurance coverage, cultural perceptions, fear, language difficulties, and transportation and time constraints. Findings suggest that barriers to cancer screening among migrant farmworkers may be addressed by providing education about cancer screening and treatment, addressing fear, language, and cultural barriers, and providing transportation and health insurance coverage. Consideration of these barriers is necessary to effectively address cancer disparities in this vulnerable population of female farmworkers.
Introduction
In 2014, 2.4 million migrant and seasonal farmworkers were employed in the United States (US). 1 While the migratory nature of seasonal farmworkers’ employment and lack of official US government data on many undocumented migrant farmworkers make researching the health of this population difficult, a 2003 literature review suggested that two-thirds of US migrant farmworkers were living in poverty. 2 Furthermore, only 5% to 11% received health insurance from an employer, and only 7% to 11% had Medicaid (Medicaid is a publicly funded health insurance program in the US that provides health coverage to eligible low-income adults, children, pregnant women, elderly adults, and people with disabilities. Medicaid is administered by US states, according to US federal requirements.) coverage, leading to limited healthcare utilization. 2 Regional studies from both the eastern and western US coasts (New Jersey, 2008 and California, 2010, respectively) found that migrant and seasonal farmworkers face a difficult combination of poverty and working conditions that promote increased rates of illness and reduced access to care.3,4 As migrant and seasonal farmworkers provide vital workforce to the US agricultural industry and have the basic human right to healthcare as set forth in the international human rights conventions, understanding and addressing barriers and facilitators to healthcare access in this population is critical. 5
Female migrant farmworkers face the double burden of economic disparity combined with the societal disparity associated with being female and warrant a strong presence in growing dialogs surrounding intersectionality. Female Latinx farmworkers are particularly vulnerable and in greater need of financial, political, and academic support. US incidence rates of breast cancer and cervical cancer—2 cancer types specifically affecting females—have been decreasing in most population subgroups.6,7 At the same time, recent data show annual rates of more than 250 000 new cases of invasive breast cancer with 40 000 deaths 6 and more than 12 000 new cases of cervical cancer with 4000 deaths, 8 while disparities by race/ethnicity and region persist. 9 Importantly, cancer outcomes are greatly improved by early detection and comprehensive screening programs are essential to reducing cancer burden. Since the year 2000 the National Breast and Cervical Cancer Early Detection Program (NBCCEDP) has provided free breast and cervical cancer screening to low-income women in all 50 United States, 10 including undocumented immigrants in the state of Michigan. 11 Because cervical and breast cancer screenings are preventative, rather than reactive, such screenings could serve as an entry point to routine medical care. The NBCCEDP program alone is estimated to have added 1608 quality adjusted life years per 100 000 women nationally at the time of the 2000 article publication. 10 Elucidating common barriers to screening among female migrant farmworkers may provide insight into healthcare practices and inform policymakers and researchers about barriers that need addressing. Thus, our purpose was to systematically review and summarize findings from prior research on barriers faced by female Latinx migrant farmworkers in accessing cervical and breast cancer screenings in the US.
Methods
Study Design
A literature review, guided by the Preferred Reporting Items for Systematic Reviews, 12 was conducted to identify and summarize existing research about barriers faced by female Latinx migrant farmworkers in accessing cervical and breast cancer screenings in the US.
Study Selection
Using the MEDLINE and Embase databases, a literature search was conducted to identify relevant literature with publication dates through October 24, 2021 using the keywords:
“migrant farmworkers AND cancer” (n = 95)
“migrant farmworkers AND healthcare access” (n = 130)
“migrant farmworkers AND breast” (n = 15)
“migrant farmworkers AND cervical” (n = 25)
“migrant farmworkers AND federally qualified health centers” (n = 15)
“migrant cancer screening” (n = 558)
“migrant farmworker cancer screening” (n = 18).
Additional identification resulted from snowball sampling by reviewing citations in each selected article. See Figure 1 for additional details regarding the search strategy.

Flow diagram of research process and search strategy.
Inclusion Criteria
Articles were included if they focused on barriers to breast or cervical cancer screening among Latinx migrant farm workers in the United States. Articles published prior to October 24, 2021 were assessed for inclusion. From the articles aggregated using the above keywords, articles that focused on specific types of cancer other than breast or cervical cancer, those not referencing the migrant farmworker population within the United States, not referencing Latinx migrants, not referencing cancer screening, not specifically discussing barriers to cancer screening, or those focused on pediatric populations were excluded. Literature reviews were also excluded (although the primary articles in the reviews were assessed for eligibility and were found to overlap with those identified by keyword search). Article language was restricted to English.
Data Extraction
Included studies were reviewed by 3 authors to assess for common themes (AP, CR, and JK). Each researcher separately evaluated the articles for mention of specific barriers to breast and cervical cancer screening. Results were compared between researchers and discrepancies were resolved through further discussion and analysis.
Results
Article Selection and Thematic Identification
Table 1 provides details of the final articles that were included (n = 19). There were more observational (n = 13) than interventional (n = 6) studies included. Barriers reported included: Cancer Knowledge (noted as a barrier in 15 articles); Cost and Insurance (noted as a barrier cited in 12 articles); Culture and/or Language (noted as a barrier in 12 articles); Transportation and/or Time Constraints (noted as a barrier in 4 articles); and Fear (noted as a barrier in 3 articles). Figure 2 illustrates the geographic locations of the included studies which spanned 13 US states (Alabama, California, Georgia, Florida, Maryland, Michigan, Nebraska, New Jersey, New Mexico, North Carolina, Texas, Washington, and Wisconsin).
Summary Study Characteristics (Listed in Order of Publication Year).

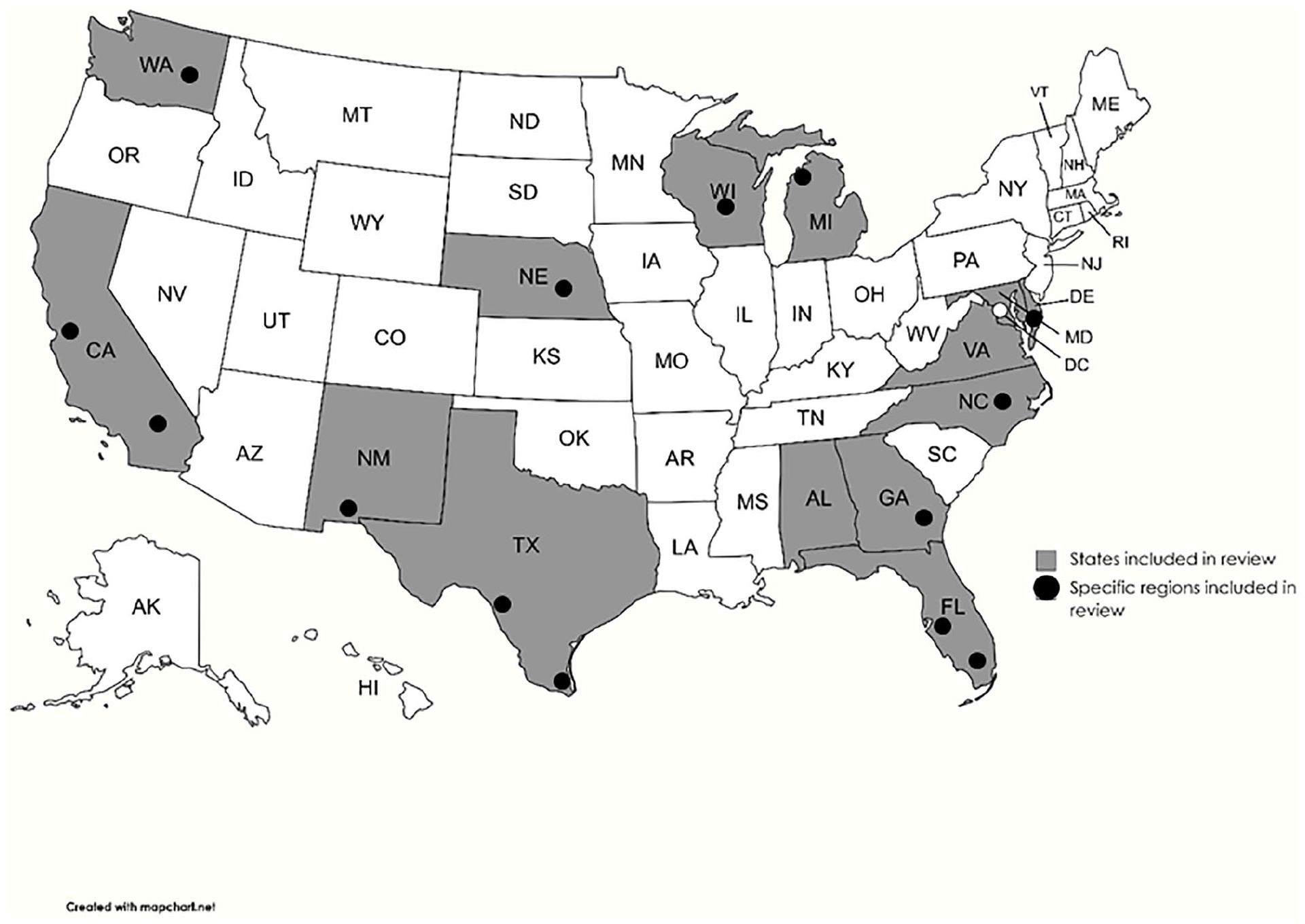
Geographic locations of regions sampled in reviewed articles.
Discussion
Cancer Knowledge
Misinformation and lack of accurate knowledge about cancer was the most common barrier discussed in the selected publications. Nearly all (15 of the 19) noted this barrier in publication years ranging from 1994 to 2019 suggesting the persistence of misinformation over time and across regions.13-27 A 1994 observational study conducted in peer discussion format amongst Latina farm workers revealed that injury and birth control use were strongly believed to be associated with the development of cancer. 13 In the same article, a belief that cancer and infection are one and the same was described. 13 A 2019 study designed specifically to assess cancer knowledge among farmworker and non-farmworker Mexican immigrants, found low to moderate knowledge of breast cancer in both groups. 14 Other research examined breast cancer knowledge through the nuanced lens of Latina migratory farm workers vs. Latina permanent residents and found that, compared to permanent residents, migrant farmworkers demonstrated significantly lower breast cancer knowledge. 15 There is a dearth of research on the breast health behaviors of migratory farm workers. This research used focus group methodology to compare the breast cancer beliefs and barriers of Latina women working as migratory farmers (n = 33) and permanent residents (n = 31). In comparison to their permanent resident counterparts, migrant farmers had low knowledge about the causes of breast cancer, and experienced significant barriers to care. Many barriers were cultural-specific, including culturally based gender roles. These findings have significant implications for designing culturally-relevant interventions to improve access to care among this population. 15 Among migrant and seasonal farmworkers in rural Michigan in 2013 “only 35% of the participants had knowledge of any cervical cancer risk factors.” 16 Prior to this study, in 2005, it was concluded that an increase in self-efficacy surrounding use of mammography and a better understanding of how early detection is associated with better outcomes could improve screening rates amongst Hispanic farmworkers in the Lower Rio Grande Valley. 17 An older study—published in 1996 when breast self-exams were still a widely recommended practice—found that women who performed breast self-exams were more likely to have adhered to mammogram testing guidelines, and that those who performed breast self-exams had been taught about the procedure and importance of such a practice. 18
In 2 farmworker communities in Texas, researchers investigated the results of an educational intervention through the use of lay health workers. 19 This intervention, specifically addressing breast and cervical cancer screening rates, involved one-on-one sessions that took place in the homes of the participants, and subsequent follow-up via phone. 19 The primary result of this intervention was the increased perception of benefit of such screening amongst these women, and the subsequent increased rate of decision to get screened amongst low-income Hispanic women in these farmworker communities. 19 Educational campaigns have been shown to be effective in increasing screening rates by reducing psychosocial barriers. These campaigns, however, must be provided with culturally sensitive, language-appropriate methods.
Cost and Insurance
While health insurance is a hotly discussed topic in contemporary American society, it is also necessary to consider the impact of noncontinuous income when considering the migrant farmworker. In a 1994 study, female seasonal farmworkers in Texas reported that they could not afford healthcare and tried to primarily use whatever free services were available at the migrant clinic, during the season that they were working near a migrant clinic. 13 Two years later a 1996 study documented the magnitude of cost barriers in obtaining a mammogram stating that “women who reported a ‘low concern’ for cost were seven times more likely. . .to have ever received a mammogram than those reporting a ‘high concern’ for cost.” 18 A 2005 study found that having health insurance was significantly positively associated with obtaining recommended mammograms in the seasonal and migrant farmworker population in the lower Rio Grande Valley. 17 In 2012 Castañeda et al 28 found that having health insurance was one of the top 3 “correlates of recent cervical cancer screening among Midwest Latina farmworkers” and in 2015 focus groups conducted by Schlehofer and Brown-Reid, 15 immigrants cited cost and lack of insurance as key barriers to completing mammogram screenings. Both cost of healthcare and lack of health insurance are barriers to healthcare use. Seasonal or inconsistent incomes held by farmworkers exacerbate the prohibitive influence of cost on obtaining preventative healthcare. Furthermore, it is probable that expensive healthcare costs would be reserved for symptomatic treatment rather than regular screenings despite lack of symptoms.
Culture
Cultural barriers to breast and cervical screenings are important to consider but should also be cautiously applied as cultural experiences of seasonal and migrant farmworkers may vary across the United States. One study conducted amongst Latina migrants concluded that there were various cultural barriers to preventative breast health measures. 15 First, there seemed to be anxiety and aversion surrounding the possibility of having a male healthcare provider involved in performing a mammogram. 15 Second, women stated that many in their community would not obtain mammograms because their husbands discouraged such behavior; it was proposed that this may be because of husbands’ hesitancy for women to expose their breasts to others. 15 Third, women mentioned shame when performing self-breast exams. 15 Finally, the study also revealed that the women in the interviewed communities often prioritized their family’s health above their own, therefore not taking the time to learn about breast cancer and go to screenings and other healthcare visits. 15 In contrast to this study’s inverse association between a husband’s influence and screening rates, a 1996 study found that women who were married were significantly more likely to have completed recommended cervical cancer screenings. 18 Women who had resided in the United States longer were also more likely to have completed recommended cervical cancer screenings. 18 Feelings of shame or embarrassment mentioned in the 2005 study matched sentiments from women in the 1994 study in which women expressed shame and embarrassment, particularly around having a male clinician perform cervical cancer screens. 13 In 2012 a study conducted in the rural Midwest found that acculturation was associated with increased rates of both breast cancer and cervical cancer screening. 28 For individual practitioners and larger healthcare clinics and systems alike it is important to consider the various ways that cultural perception of cervical cancer and breast cancer screenings might prevent patients from completing these important preventative measures, and to care for patients in a way that acknowledges, and is sensitive toward, these concerns.
Language
One of the most obvious topics of discussion when it comes to barriers to care amongst migrant populations is that of language barriers. Interestingly, amongst the studies that met our inclusion criteria, only 7 of the 19 articles described language barriers as a major factor contributing to reduced cervical and breast cancer screening rates among Latinx migrant farmworkers in the United States, perhaps indicating societal improvements in reduction of language barriers.14,17,28
One article examining determinants of breast cancer and cervical cancer screening use amongst rural Latin migrant farmworkers in Michigan found that English language proficiency was related to higher screening rates. 28 Furthermore, breast self-exams and having health insurance were also significantly correlated to getting screened for breast and cervical cancers. 28 Thus, the article suggests that education (on topics such as breast self-exams) and outreach (perhaps in obtaining health insurance) in the patients’ native languages could help patients participate in these key components that were shown to be related to higher screening rates. 28
Two articles that did not cite language barriers as a determining factor of breast and cervical cancer screening amongst the studied population did conduct surveys about other barriers entirely in Spanish, therefore suggesting language to be an important factor.14,17
Transportation and Time Constraints
All 4 articles that noted transportation and/or time constraints framed these barriers as logistical factors that decrease access to services.23,24,29,30 In the 2016 article conducted by Ramos et al 24 in Nebraska, a direct quote from a focus group participant summed up the barrier and provided suggestions: “scheduling and hours are important. Use the schools, churches, and all of those centers where a lot of people go.” Similarly, women interviewed in a 2015 study in California, specific recommendations to increase cancer screening by addressing these barriers included holding a screening event in a local community setting, conducting door-to-door outreach, advertising on the radio, and providing small incentives for completing the screening. 23
Fear
In all 3 articles that noted fear as a barrier to preventive screening for cancer, the fear described was of the medical system,21,23,30 but not further specified in 2 of the 3 articles.21,30 The 2015 study in California of women from the Mixtec and Zapotec communities by Maxwell et al describe that women were fearful about going to the doctor because they did not know what to expect and heard negative experiences. These fears appeared to be related to the concept that going to the doctor was associated with sickness and receipt of bills; whereas preventive services were not a well-understood concept. 23
Summary of Findings
In this literature review of publications identifying barriers to breast or cervical cancer screening among US female Latinx migrant farmworkers, 19 articles met inclusion criteria. Common themes about barriers to cancer screening included: lack of cancer knowledge, cost/inability to pay, lack of health insurance coverage, cultural perceptions, language difficulties, fear, transportation and time constraints.
Strengths and Limitations
The strength of this study is that we limited our focus to a specific topic and found representation in publications describing research from various regions across the US. A limitation is that any insights from the included studies may not be representative of the larger migrant farmworker population because results are restricted to existing published research which was only available in selected communities. Fewer studies included in this review used interventional designs; future interventional programs addressing the identified specific needs and barriers to obtaining cervical and breast cancer screening among female migrant farmworkers should be explored.
Future Studies
While understanding the barriers and resources of a specific community are vital to the success of an interventional program, the work already completed in this area, as discussed in this paper, should provide a catalyst for the development of more interventional work. When developing interventional programs for a specific community it can be presumed that there is a high likelihood the above barriers will impact the community, albeit some more impactful than others. Therefore, pre-intervention work should focus on resources the community already has in place, as well as additional barriers that may be very specific to that community.
As reflected by the limited number of studies found on this subject, it is important that more work be done to investigate barriers within specific communities. These studies should include geographical areas not included in the current set of studies so that further literature review and meta analyses can provide a more generalizable result.
Additionally, while it is important to parse out barriers that may make it challenging to deliver this care to this patient population, it is also important to make note of facilitators of breast and cervical cancer screening for seasonal and migrant farmworkers. This information could be dually useful to investigators designing an intervention which aims to reduce barriers and amplify facilitators of this care.
The results of this review might also contribute to the development of advocacy tools to aid in the development of healthcare and migrant policy, as well as inform the declaration of government fiscal resources, be it local, state, or federal. While Michigan’s NBCCEDP program, known as Breast and Cervical Cancer Control Navigation Program (BC3NP), does provide initial screening and diagnostic workup for migrant farmworkers and undocumented immigrants, it does not cover the cost of treatment for disease diagnosed in the process. 11 While the BC3NP program increases access to preventative screening, the program will only positively affect life years of the patient population if the patient can subsequently access early treatment. 11
Public Health Implications
Findings from this systematic review suggest that lack of cancer knowledge, cost/inability to pay, lack of health insurance coverage, cultural perceptions, and language difficulties are significant barriers to cervical and/or breast cancer screening among female Latinx seasonal and migrant farmworkers in the United States. Consideration of these barriers may be addressed by providing education about cancer screening and treatment, addressing language and cultural barriers, and providing health insurance coverage. Attention to these barriers is necessary to effectively address cancer disparities in this vulnerable population of female farmworkers. Local, state, regional, and national level efforts are likely needed to address these barriers in both political and non-political spheres.
Footnotes
Acknowledgements
The authors would like to thank Abe Wheeler for his direction and assistance with literature searching and the team who obtained and implemented the training grant that supported this project designed to promote Research to Reduce Disparities in Disease (R2D2) including Drs. Harold (Woody) Neighbors, Jamil Scott, Mieka Smart, and Todd Lucas.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by the National Institutes of Health Training Grant R25HL140319 (Pariser A, Trainee). The funding source had no involvement in the study design, collection, analysis, interpretation, writing, or decision to submit this article for publication.