
Abstract
Consistent with the Institute for Healthcare Improvement’s Triple Aim initiative, innovative models of healthcare delivery are needed to enhance quality and decrease costs. 1 This concern may be addressed in part by grouping patients with similar needs. 2 Introduced approximately 20 years ago, group visits remain a viable option to foster peer support and to improve efficiency in dissemination of education.3,4 Group visits—outpatient office visits designed for multiple patients with similar health-related needs to receive medical care and self-management training 5 —are meant to serve as an adjunct to routine office visits.
While most group visit research has focused on diabetes, group visits have been implemented for other conditions, including hypertension, pregnancy, and coronary artery disease.6-8 Many studies have demonstrated improvements in disease-oriented outcomes, satisfaction, and cost savings as a result of group visits,9-11 but these results have been inconsistent given the variability in curricula and topics addressed. 12
Additionally, few clinicians have had the opportunity to incorporate group visits into their practices, despite evidence of benefits for patients and clinicians. 13 Group visits may be more common in residency practices, given the time and resources needed to implement them. Because little is known about the modifiable barriers that may preclude incorporating group visits into routine care, the study team sought to identify these obstacles so that strategies to address them may be developed.
Methods
A 10-question survey was developed to assess clinicians’ experience with and barriers to group visits. These questions were developed from prior study of patient-reported barriers in addition to discussions with clinicians with extensive group visit experience, who provided feedback for the survey. Self-reported demographic data, including gender, age, race, and ethnicity were also collected.
The survey (see the appendix) was mailed to a convenience sample of all 246 family medicine and internal medicine clinician members in a practice-based research network (PBRN) of a tertiary care health care network in Pennsylvania. The Lehigh Valley PBRN consists of more than 90 primary care practices, but only family and internal medicine clinicians were eligible for inclusion. Practice model types include hospital-owned practices, a regional practice association, independent small groups, clinics, and solo practitioners. Some practices included resident clinicians.
The mailing included a letter describing the study, the survey tool, a $5 gift card for remuneration, and a stamped return envelope. A reminder letter was sent 1 week following the initial mailing. The survey included an introductory paragraph for clinicians who may have less familiarity with group visits defining them as follows: Group visits consist of two components: (1) a one-on-one visit with a doctor to talk about your diabetes, followed by (2) a class about managing your illness. These visits provide an opportunity to meet other people with similar health problems as well as to share experience and learn from each other. Different topics are presented at each visit; time is allowed for the doctors to answer your questions.
Descriptive analyses were conducted for all survey responses. The interest in and likelihood of conducting group visits questions were answered on a 10-point Likert-type scale. For analytical purposes and based on distribution, scores on these questions from 1 to 3 were categorized as low, from 4 to 6 were categorized as moderate, and from 7 to 10 were categorized as high. Subgroup analysis was performed using chi-square tests to compare responses between those with and without group visit experience. Analyses were conducted with IBM SPSS version 22.0 (IBM Corp, Armonk, NY).
Results
There were 107 responses from the sample for a 44% response rate. Mean age of respondents was 50.6 years (SD = 11.9). Mean number of years in practice was 20.5 (SD = 12.0). Respondents included clinicians practicing in rural, suburban, and semiurban environments with an average of 6.7 clinicians (SD = 6.5) per practice.
Among the respondents, 27 (25%) had organized or participated in a group visit. Only 3 were involved with group visits at the time of the survey. Of the 27 respondents with group visit experience, 15 had exposure to group visits during medical training, 18 had conducted group visits in a practice, and 19 reported adequate training to conduct group visits in the future. Those in practice for 10 or fewer years (n = 23) were significantly more likely to have group visit experience than those in practice for 11 to 20 years (n = 32), χ2(1, n = 55) = 4.50, P = .034, and greater than 20 years (n = 47), χ2(1, n = 70) = 17.02, P < .001.
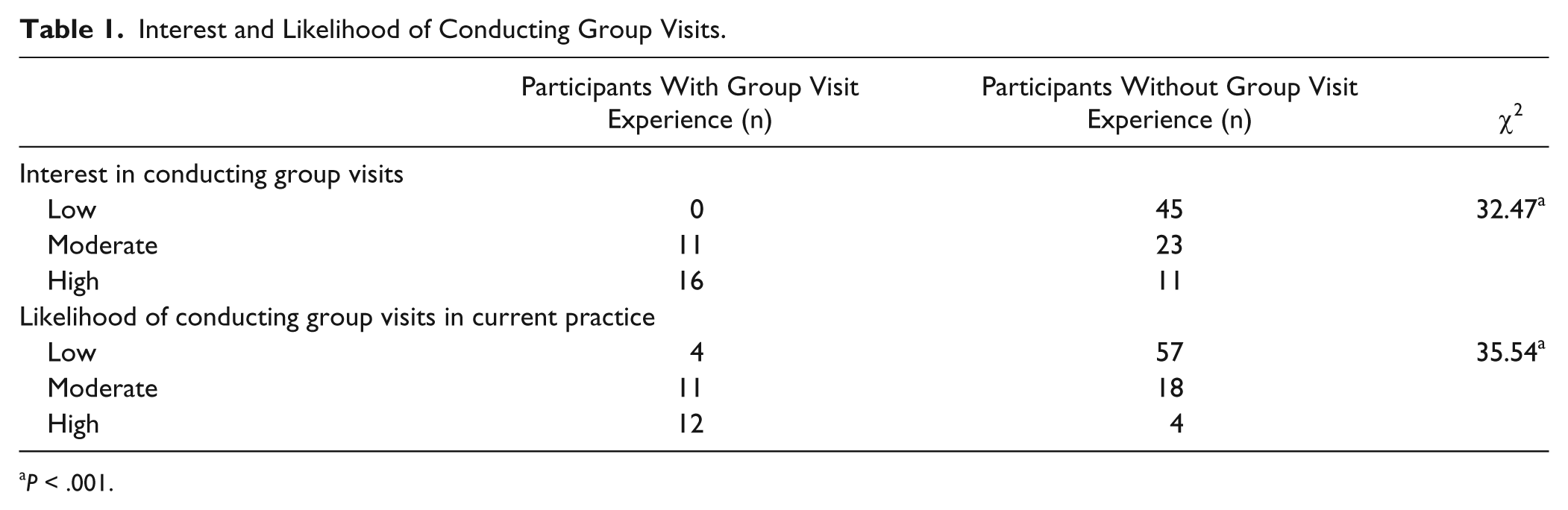
Table 1 displays respondents’ interest in conducting group visits and likelihood of conducting group visits. Chi-square analysis showed that both interest in conducting group visits, χ2(1, n = 106) = 32.47, P < .001, and likelihood of conducting group visits, χ2(1, n = 106) = 35.54, P < .001, were significantly related to prior experience. Overall, those without previous experience with group visits reported low to moderate interest in and likelihood of conducting group visits, while most who had previous experience reported a desire to implement group visits again in the future.
Interest and Likelihood of Conducting Group Visits.
P < .001.
Figure 1 shows the potential barriers to incorporating group visits into practice that respondents endorsed, broken out by past experience. Time and staffing were identified by both groups. Those with group-visit experience also identified recruitment as a barrier while those without experience identified lack of training as a barrier. Those with group visit experience named staffing concerns (n = 16), time (n = 12), and recruitment (n = 12) as the top barriers of group visit implementation. Those without group visit experience named never trained (n = 49), time (n = 47), and staffing concerns (n = 43) as their top barriers.

Factors that prevent clinicians from incorporating group visits in practice.
Respondents also identified resources required to incorporate group visits into their current practices. Both groups identified training on coding and billing (n = 19 vs 57) and training on group visit implementation (n = 16 vs 57) as resources needed to implement group visits. Additional essential resources named by those with group visit experience were time and collaborative partners (n = 16), whereas curriculum was commonly cited by those without experience (n = 45).
Discussion
Only about one-quarter of our PBRN clinicians had prior experience conducting group visits. This experience was significantly related to years in practice; clinicians who were earlier in their careers were more likely to have group visit experience. Those who had been in practice longer may not have received group visit training, which has more recently become a part of many medical school curricula. Because lack of training was a top barrier for those without group visit experience, strategies to increase clinician exposure to conducting group visits may facilitate group visit implementation in their own practices. Prior study has suggested CME as a viable approach to address this gap. 14
In addition to providing opportunities for training regarding group visits, support from practice leadership may help overcome the logistical barriers cited by respondents. All respondents identified time and staffing concerns as potential logistical barriers. Development of curriculum was identified as requiring additional time, though this concern may be addressed with the use of standardized educational materials. While the implementation of any additional program may add to staff burden, physician and practice champions prove vital to the success of program sustainability. Although group visits represent a shift in clinical approach, with strong leadership and infrastructure support, they could increase the productivity of the practice, fitting within the fee-for-service world as well as in value-based practice models and community clinics.
The infrastructure needed to conduct group visits consists primarily of resources to recruit patients, make reminder phone calls, and schedule the visits. Respondents in this study with prior experience were more likely to endorse patient recruitment as a barrier, probably because they had experienced the time-consuming task of recruitment. Further study is needed to identify best practices for recruitment and retention (ie, patient engagement), though a population-based mailing may prove successful in reducing time and resources associated with individualized recruitment methods.
Limitations of this study include use of one PBRN, which limits generalizability. These clinicians operate within one network, increasing the likelihood that they experience similar barriers to implementing group visits. An additional limitation for the analysis was the imbalance of the subgroup size between those with and without group visit experience. Given the recent implementation of group visits into practice, this may be representative of cohorts with similar ranges for years in practice. Additionally, there is potential that some respondents may have been from the same practice and as such had similar experiences. However, the median number of clinicians per practice was 5, making this less likely for most respondents.
Based on what was learned in this study, next steps may include addressing training for clinicians without group visit exposure and for those interested in further education. The modifiable, practice-based barriers named by clinicians should also be compared to the patients’ perspective to explore convergence and divergence between the 2 perspectives.
Conclusions
In a sample of 107 primary care clinicians, interest and likelihood of including group visits in practice were significantly related to prior group visit experience. Time, staff support, and training were frequently cited barriers. Addressing these barriers, particularly training for those without prior experience, may enhance the incorporation of group visits into practice.
Footnotes
Appendix
Acknowledgements
The authors gratefully acknowledge the Dorothy Rider Pool Health Care Trust for funding this work. The authors also thank Jacqueline Grove for assistance with editing and manuscript preparation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the Dorothy Rider Pool Health Care Trust.