
Abstract
Background
Cardiovascular disease is the leading cause of death in the United States, and hypertension is a primary contributing factor.1-3 Risk factors for hypertension are well known and include modifiable behaviors (eg, physical inactivity, unhealthy diet, overweight and obesity, excess alcohol consumption, smoking) and nonmodifiable factors (eg, family history of hypertension, age, gender, race/ethnicity). 4 Current guidelines for the primary prevention of hypertension target modifiable risk behaviors. 5 The most common places clinical care services are provided are primary care provider (PCP) offices. 6 In the United States, PCP visits account for more than half of all ambulatory care visits. For example, 62% of the 1.1 billion ambulatory visits were made to primary care sites in 2008. 7 This frequent interaction of patients and PCPs creates ongoing opportunities to promote the prevention of hypertension to a large population. Advice from PCPs has been shown to influence behaviors8,9 and to motivate patients to adopt healthy behaviors.10-12 We sought to assess the prevalence of PCPs’ recommendations to prevent hypertension and the factors that influence them to make such recommendations.
Methods
DocStyles is a Web-based panel survey conducted by Porter Novelli. The survey participants were family and general physicians, internists, and nurse practitioners. In 2012, DocStyles was conducted from June to July, and participants were eligible if they had been in clinical practice for a minimum of 3 years; worked at an individual, group, or hospital practice in the United States; and saw at least 10 patients per week. Physicians and nurse practitioners were selected from separate volunteer panels. Physicians were randomly selected from the Epocrates Honors Panel (n ≥ 275 000) and matched to the American Medical Association master file proportions for age, sex, and region. Nurse practitioners were randomly selected from the Epocrates’ Allied Health Panel (n ≥ 78 000). Quotas were set to reach 1000 PCPs and 250 nurse practitioners. Physicians and nurse practitioners from both panels were invited to participate by e-mail. Participation was voluntary, and respondents could exit the survey at any time. Those who completed the survey received an honorarium of $20 to $85, which varied depending on the skip patterns and length of the survey. The overall response rates were calculated using a formula that included total sample contacted, surveys completed, incomplete surveys, respondents not meeting screening criteria, nonresponse, and respondents removed from the eligible sample because quotas were filled.
The survey asked about PCPs’ demographic characteristics (age, sex, race/ethnicity) and medical practice (specialty, setting, years in practice, teaching hospital privileges, financial situation of the majority of their patients). Questions about health-related behaviors included fruit or vegetable consumption (days per week consuming ≥5 cups of fruits or vegetables), current smoking (days per week smoking cigarettes, cigars, or pipes), and physical activity (days per week doing ≥30 minutes of physical activity). Respondents also reported height and weight, which were used to calculate body mass index (units of kg/m2).
Primary care providers’ hypertension prevention recommendations were assessed with the question, “What types of advice do you give adult patients about preventing high blood pressure?” Available responses were “Eat a healthy diet,” “Cut down on salt,” “Attain or maintain a healthy weight,” “Get enough sleep each night,” “Limit the use of alcohol,” “Be physically active,” “Smoking cessation,” “Take nutritional supplements,” “Try relaxation methods,” “Get intellectual stimulation,” and “None of these.”
Statistical Analyses
Recommendations in agreement with current guidelines for hypertension prevention 5 were selected for analysis: eat healthy diet, reduce salt intake, attain or maintain a healthy weight, limit alcohol use, be physically active, and smoking cessation. We measured the prevalence of PCPs’ reported hypertension prevention recommendations independently and collectively (ie, all 6 healthy behavior recommendations).
The differences in PCP characteristics by specialty (family physician, internist, and nurse practitioner) were assessed with chi-square tests for categorical variables and analysis of variance tests for continuous variables. The association of PCPs’ demographic characteristics and their recommendations for hypertension prevention were assessed with chi-square tests. The odds of providing all 6 healthy behavior recommendations, adjusting for demographic characteristics (age, sex, race/ethnicity) and specialty, were assessed by logistic regression models. Other variables (eg, physical activity, fruit or vegetable intake, years in practice, practice setting) were added into the models if the P was less than .2 in univariate analysis. All analyses were conducted using SAS software (version 9.3, SAS Institute, Inc, Cary, NC).
Results
A total of 1253 PCPs completed the survey (537 family physicians, 464 internists, and 252 nurse practitioners). The response rate was 52.2% (physicians = 49.9%, nurse practitioners = 65.4%). We found significant differences by PCP specialty for demographic characteristics (gender, race/ethnicity), adequate fruit and vegetable consumption, and practice characteristics (years in practice and practice setting) (Table 1).
Demographic Characteristics, Health Behaviors, and Practice Characteristics of Respondents to the DocStyles 2012 Survey, by Primary Care Physician Specialty.
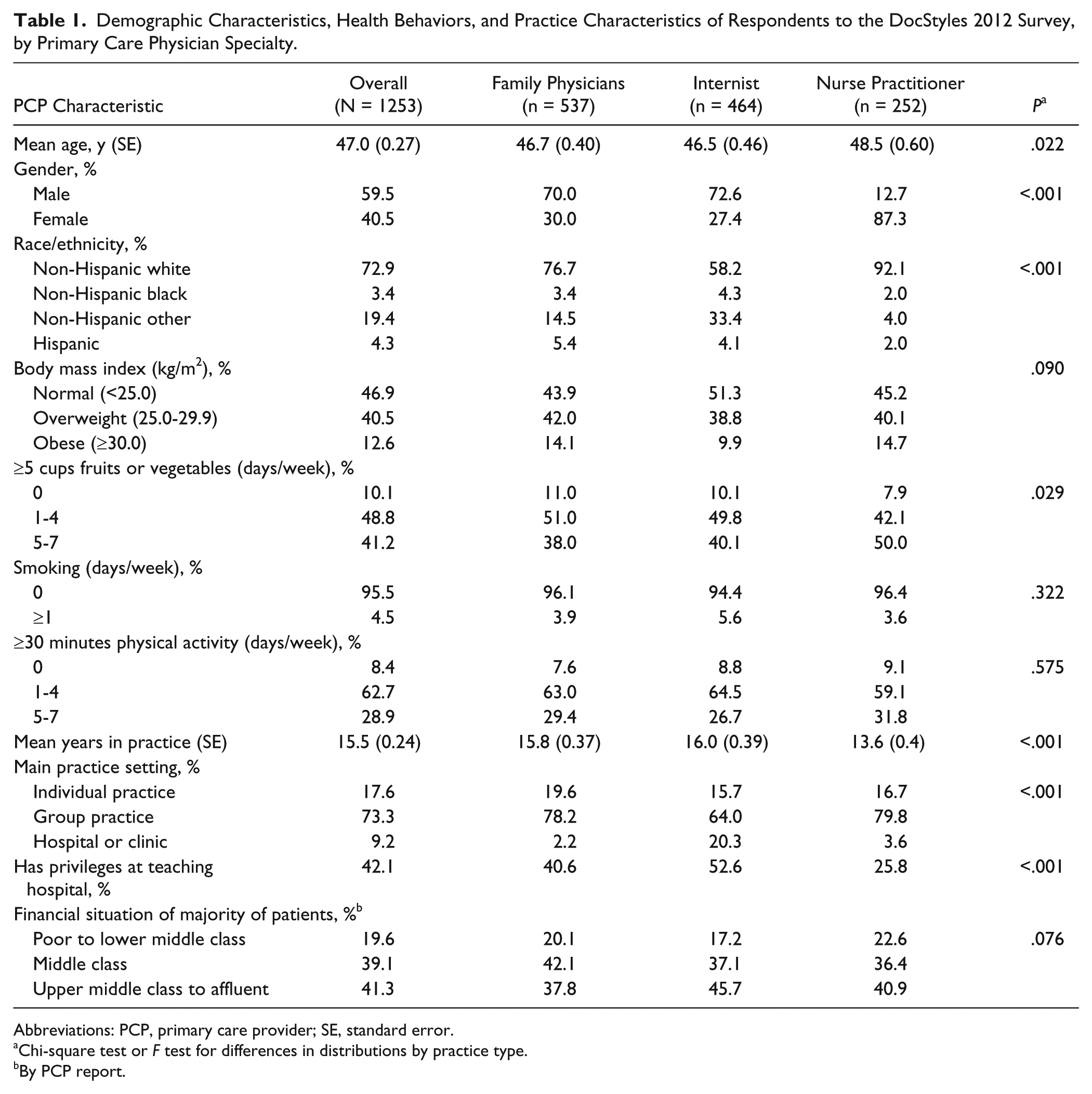
Abbreviations: PCP, primary care provider; SE, standard error.
Chi-square test or F test for differences in distributions by practice type.
By PCP report.
A high percentage of PCPs recommended most hypertension prevention measures (Table 2). Overall, 89.4% recommended eating a healthy diet, 89.9% recommended reducing salt intake, 90.3% recommended attaining or maintaining a healthy weight, 95.1% recommended physical activity, and 90.4% recommended smoking cessation to their patients who smoked. However, only 69.4% recommended limiting alcohol intake. In general, the prevalence of recommending these behaviors was higher among PCPs who were older, classified as a nurse practitioner, who reported adequate fruit or vegetable intake, and who did not smoke.
Prevalence of Making Select Hypertension Prevention Recommendations Among Respondents to the DocStyles 2012 Survey, by Primary Care Provider (PCP) Characteristics.

Abbreviation: PCP, primary care provider.
P < .05 using chi-square test comparing differences in recommending the activity.
By PCP report.
Overall, 56.1% of PCPs reported that they made all 6 hypertension prevention recommendations. After adjustment, there were no significant differences in making all 6 recommendations by PCP age, sex, race/ethnicity, body mass index, smoking status, specialty, or practice setting. However, making all 6 recommendations was more likely among PCPs who reported consuming the recommended amount of fruits or vegetables and among those who engaged in the recommended amount of physical activity compared with those who did not (Table 3).
Prevalence and Odd Ratios of Making All 6 Healthy Behavior a Recommendations, Among Respondents to the DocStyles 2012 Survey, by Primary Care Provider Characteristics.
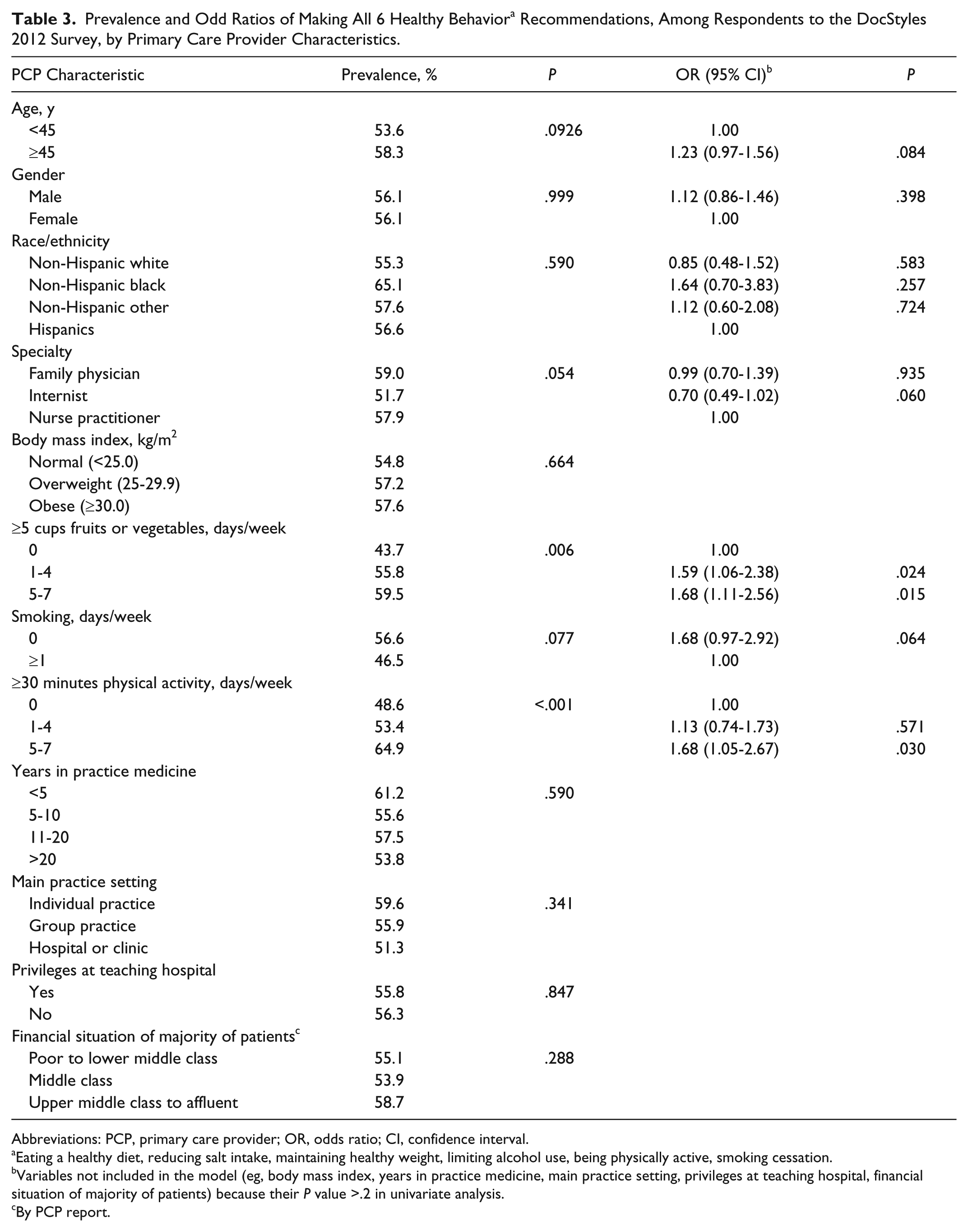
Abbreviations: PCP, primary care provider; OR, odds ratio; CI, confidence interval.
Eating a healthy diet, reducing salt intake, maintaining healthy weight, limiting alcohol use, being physically active, smoking cessation.
Variables not included in the model (eg, body mass index, years in practice medicine, main practice setting, privileges at teaching hospital, financial situation of majority of patients) because their P value >.2 in univariate analysis.
By PCP report.
Discussion
The principal findings of current study is that most PCPs, according to their self-reported statement, provided evidenced-based hypertension prevention recommendations to their adult patients that align with current guidelines: eating a healthy diet, reducing dietary salt intake, attaining or maintaining a healthy weight, being physically active, and quitting smoking (for their patients who smoke). 5 However, only 69.4% of PCPs recommended limiting alcohol intake to prevent hypertension. Overall, 56.1% of PCPs said they recommended all 6 healthy behaviors to reduce the risk of hypertension for their adult patients. Furthermore, we found that PCPs who consumed the recommended amount of fruits or vegetables and participated in the recommended amount of physical activity were significantly more likely to recommend all 6 healthy behaviors.
Hypertension prevention recommendations recognize a number of modifiable risk factors, including an unhealthy diet, excess sodium intake, obesity, excess alcohol consumption, physical inactivity, and smoking. 5 National health data have shown considerable room for improvement in these lifestyle behaviors and conditions. For example, only 32.5% of US adults were consuming the recommended amount of fruits or vegetables in 2000-2009, 13 less than 10% consumed <2300 mg sodium per day in 2003-2008, 14 only 32.5% of adults were with classified as normal weight in 2005-2010, 15 binge drinking prevalence was 17.1% in 2010, 16 20.6% of adults met both aerobic and muscle-strengthening physical activity guidelines in 2011, 17 and about 19.0% were current smokers in 2011. 18
Primary care providers can influence patients’ decisions to participate in healthy lifestyle behaviors. A randomized controlled trial showed that patients who received counseling on physical activity from general practitioners or family physicians increased their level of physical activity significantly compared with those who did not receive counseling.10,11 A complementary study found that patients who received advice from their provider to quit smoking or exercise more were more likely to report that they attempted these actions. 9 The study also showed that health care provider’s advice on physical activity was the most effective way to improve patients’ physical activity. The health care providers can maximize the success of increasing patients’ physical activity level by repetition of the message. 19
We found that PCPs’ healthy behaviors, such as getting the recommended amount of physical activity and consuming the recommended amount of fruits or vegetables, were associated with recommending behaviors to prevent high blood pressure, regardless of PCP demographic and clinical practice characteristics. This report is consistent with an earlier report that PCPs’ healthy behaviors are related to their recommendations for healthy lifestyle behavior management among patients with hypertension. 20 Other studies have also found that health care providers with healthier lifestyle behaviors were more likely to counsel patients to stop smoking, exercise, manage their weight, and reduce their alcohol intake.21-23
Our results should be interpreted in the context of potential selection and reporting biases. First, this report was to assess the intent of the health care provider, rather than to assess the actual advice provided to patients. What the health care providers said they did could be different from what they really did. The social desirability of saying “Yes” (i.e., that they did make these recommendations) would overestimate the percentage reported compared with what actually happened in clinical practice. Second, the survey only asked about recommendations in general. Thus, it is not clear how often PCPs made the recommendations, or with what degree of enthusiasm, or if the advice varied by comorbid conditions. To assess whether and how the PCPs made the recommendations, we would need to use a combination of medical chart review and clinician reports. Third, the survey was not a nationally representative sample of physicians or nurse practitioners, and thus the results may not be generalizable. Finally, as a Web-based survey, the survey requires internet access and a basic familiarity with internet-based surveys. While limitations do exist when using this survey platform, DocStyles is a large, national survey conducted annually among a diverse group of PCPs, and allows for the collection of current information on health care provider attitudes and behaviors.
In this study, most PCPs stated that they provided evidenced-based hypertension prevention recommendations to their patients, and just more than half stated that they provide all 6 healthy behavior recommendations for hypertension prevention to their adult patients. Ideally, each of the recommendations would be provided to patients regularly, especially those at the highest risk, 5 but PCPs are constantly faced with clinical time constraints and patients who have multiple comorbid conditions or urgent care needs. 24 Alternate channels for hypertension prevention recommendations are available. For example, team-based care, or the use of multidisciplinary professionals, inside and outside the clinical setting, has been used to promote health and manage health conditions. This structure is ideally suited for prevention messages, especially those for common serious conditions such as hypertension. 25
In 2011, the US Department of Health and Human Services launched the Million Hearts initiative. By bringing communities, health systems, nonprofit organizations, federal agencies, and private sector partners together, Million Hearts focuses on implementing evidence-based strategies in the clinical and community environments to collectively prevent 1 million heart attacks and strokes over a 5-year period (2012-2017). 26 Preventing and controlling hypertension is essential to achieving this objective, and requires a diverse range of activities, from changing the context and supports for a healthy lifestyle to individual interventions in the clinical setting. In each of these settings, evidence-based interventions should be used when available. Resources such as the Guide for Community Preventive Services (http://www.thecommunityguide.org) and the US Preventive Services Task Force (http://www.uspreventiveservicestaskforce.org) recommendations are available for practitioners in diverse settings.
In the clinical setting, PCPs are a trusted source of health information who interact with the general population. We found that PCPs were more likely to recommend healthy lifestyle behaviors if they themselves participated in healthy behaviors. Hypertension prevention is multifactorial and will require coordinated care and programs in the clinical setting coupled with effective community-based supports for healthy behaviors.
Footnotes
Authors’ Note
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.