
Abstract
Keywords
Introduction
Despite a decline in the unintended pregnancy rates among US adolescents, 1 the US rate remains significantly higher than that in Canada and European countries.2,3 Use of an intrauterine contraceptive device (IUD) is associated with marked reductions in unintended pregnancy among adolescents.4,5 Professional medical guidelines support IUDs as a first-line contraceptive for adolescents.6-9 Yet only 4.5% of contracepting US adolescents have an IUD. 10
Myriad factors, including clinician factors, contribute to US adolescents’ infrequent use of IUDs. US female adolescents are cared for by a mix of primary care provider (PCP) types. Younger adolescents are more likely to see a pediatrician, while adolescents 17 to 20 years old are more likely to see an Obstetrician-Gynecologist (ObGyn). The proportion of outpatient visits by females 13 to 20 years old with family physicians (FPs) remains fairly constant at approximately 35% to 40% throughout adolescence. 11 Though about half of all pediatricians provide some reproductive health care, 12 studies have described gaps in pediatricians’ general contraception knowledge and their interest in additional pregnancy prevention training.13,14
Primary care providers’ attitudes and practices toward IUD counseling for adolescents remains underexplored. 15 In general, pediatricians, FPs, and ObGyns often use unduly restrictive criteria when considering IUD eligibility.16-22 Just 3 published studies concerning IUDs have included generalist pediatricians.16-18 We found no published study explicitly examining frequency of and factors associated with PCPs’ counseling adolescents about IUDs.
In order to address these gaps in the literature we surveyed Bronx pediatricians, FPs, and ObGyns, exploring factors associated with their counseling adolescents about IUDs. The Bronx is the New York State County with the highest adolescent pregnancy rate. 23 We designed our quantitative survey based on our prior qualitative research, which suggested that PCPs’ training, their attitudes about IUDs, and access to a provider in the clinic who inserts IUDs may be associated with increased likelihood of counseling adolescents about IUDs.16,24 We anticipated that, because of training and scope of practice issues, different factors would be associated with pediatricians’ compared with FPs’ and ObGyns’ IUD counseling practices. We aimed to identify those factors. Our overall goal in conducting this study was to inform the development of interventions to increase the proportion of PCPs who counsel adolescents about IUDs.
Methods
Participants and Recruitment
We invited PCPs affiliated with an academic medical center in the Bronx, New York, to complete an anonymous online survey (www.surveymonkey.com). Clinicians from the following departments were sent a recruitment e-mail containing a link to the survey: pediatrics, family and social medicine, and obstetrics and gynecology and women’s health. Eligibility criteria included the following: works at minimum 2 outpatient sessions per week, clinical panel includes female adolescents, and discussed contraception with female adolescent patients in the prior 12 months. Trainees and subspecialists were excluded. Nonresponders were contacted up to 3 times.
Survey Design
Our investigator developed survey was based on results from our qualitative research 16 with input from experts in the field. Prior to implementation we piloted the survey and revised it accordingly. Survey items were organized around capability, opportunity, motivation (COM) implementation science theoretical framework 25 used in our prior work. 16 The COM framework was developed to systematically improve the design of behavior change interventions.
Survey Variables
Our primary outcome—frequency of counseling female adolescents about IUDs—was assessed with the question: “In a typical office visit conversation with a female adolescent about contraception how frequently do you discuss IUDs?” Responses on a 5-point Likert-type scale ranged from “very infrequently” to “very frequently.” Since we aimed to examine associations between those who do and do not frequently counsel, for our analysis responses were dichotomized into “frequently” (responses “very frequently” and “somewhat frequently”) and “not frequently” (all other responses).
The survey included questions about demographics, training, and clinical practice. We assessed IUD insertion experience during training, in the prior 12 months, and for patients 20 years or younger. Those who reported inserting an IUD in the past 12 months were asked if the clinical site stocks IUDs. Noninserters were asked whether anyone at their clinic or office inserts IUDs.
To measure IUD counseling skill we asked clinicians to rate their competency on a 5-point Likert-type scale in the following areas: (a) counseling, (b) answering patient questions, and (c) managing side effects. We combined responses from these separate questions into a single competency scale (Cronbach’s α = .95).
We assessed clinician attitudes and beliefs about how use of prescription contraception (ie, oral contraception or IUD) might affect condom use or risk of a sexually transmitted infection (STI) as well as their perceptions of STIs and unintended pregnancy rates among adolescents in their practice.
Classification of Clinicians
Given our specific interest in learning about pediatricians’ counseling practices, and the a priori likelihood that FPs and ObGyns as compared with pediatricians would identify different factors affecting their counseling, we combined the latter 2 groups for analysis. If we had more ObGyn respondents we would have conducted our analysis with 3 separate groups. In order to assess the FP-ObGyn grouping we conducted χ2 tests on all salient variables. We found that while ObGyns had more IUD insertion experience and higher competency score, there was no statistically significant difference in responses to our primary outcome measure.
Analysis
We examined differences between pediatricians and FP-ObGyns on all our variables. Then we conducted 2 separate analyses stratified by pediatricians or FP-ObGyn grouping in order to examine within-group factors associated with frequently counseling adolescents about IUDs. We used χ2 or Fisher’s exact test and analysis of variance as appropriate to assess bivariate associations. All statistical tests were 2-tailed using α = .05 and were performed with SPSS (PASW Statistics Version 20.0.0 2011, IBM Corporation, Chicago, IL) software.
This study was approved by the institutional review board of the Albert Einstein College of Medicine.
Results
We sent recruitment e-mail(s) to 470 clinicians, of whom 203 responded (43.2% response rate). Of these, 151 were eligible. The most frequent reasons for ineligibility were insufficient number of clinical sessions or not discussing contraception with adolescents (Figure 1).
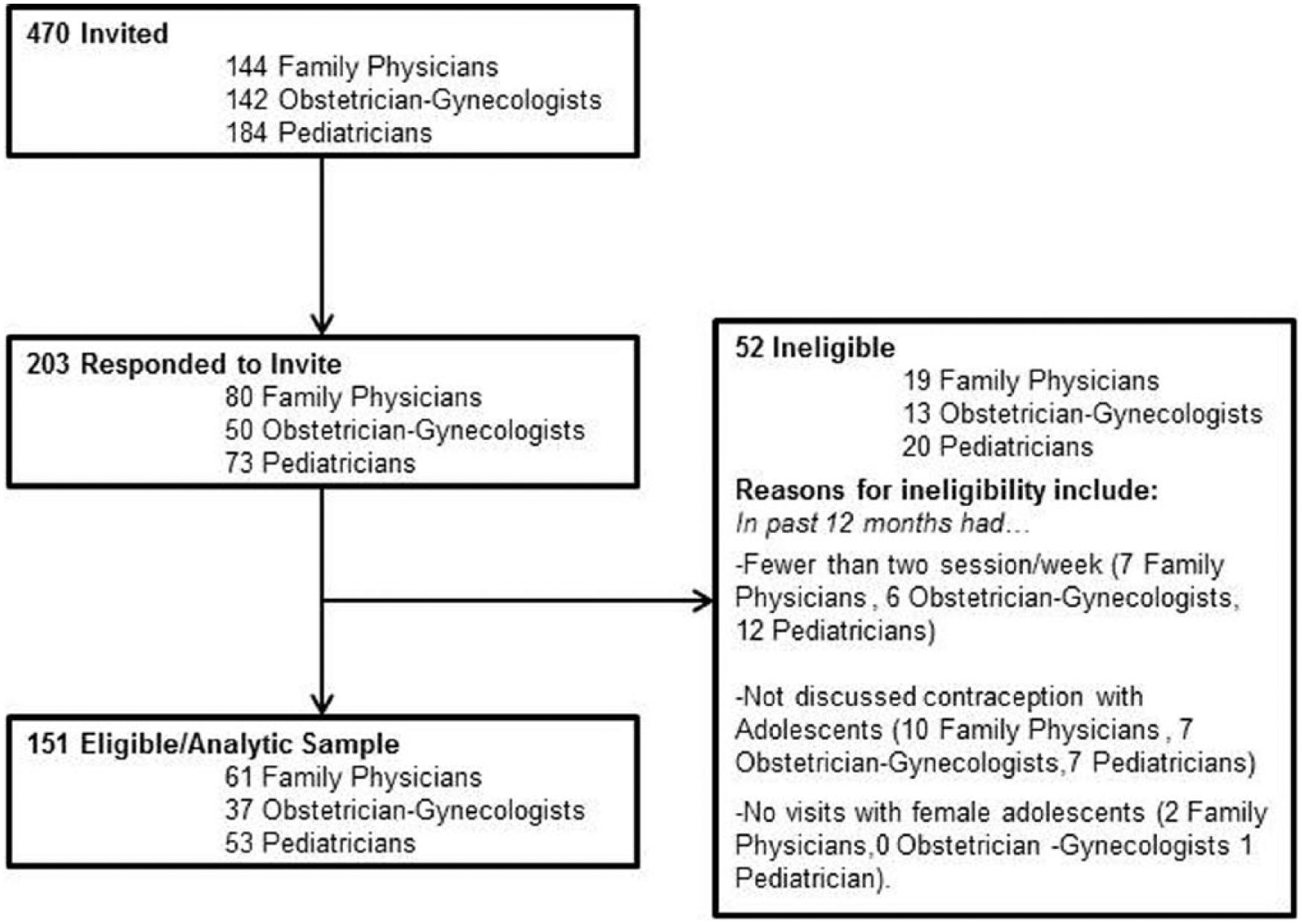
Respondent flowchart.
Comparison of Pediatricians With Family Physicians and Obstetrician-Gynecologists
In terms of their demographics and clinical practice, Pediatricians as compared with FP-ObGyns, work more clinical sessions, have a larger proportion of office visits with female adolescents and were less likely to initiate prescription contraception in the past year (Table 1).
Comparison of Pediatricians with Family Physicians and Obstetrician-Gynecologists Demographic Characteristics, Clinical Practice, Skills, Attitudes, and Beliefs.

Abbreviations: MD, medical doctor; DO, doctor of osteopathic medicine; NP, nurse practitioner; PA, physician assistant; n/a, not applicable; STI, sexually transmitted infection.
Family physician, n = 61; obstetrician-gynecologist, n = 37.
Totals may vary due to missing data.
Refers to how many years ago clinical training was completed.
Refers to how many half days of outpatient care clinicians provide weekly.
Refers to proportion of outpatient office visits with female adolescents.
Fisher’s exact test (2-tailed).
Asked only of those 64 providers who insert IUDs.
Asked of all pediatricians and only of those 35 family physicians and obstetrician-gynecologists who have not inserted an IUD in the past 12 months.
Three-item Competency Scale based on the responses to the following 3 separate questions: Degree to which you feel competent (1) counseling about IUDs, (2) answering patient questions about IUD, and (3) managing expected IUD side effects.
As compared with pediatricians, our primary outcome—frequent counseling of adolescents about IUDs during a contraception-related office visit—was more than twice as common among the FP-ObGyn group (35.8% and 82.6%, respectively).
Clinician groups differed on all knowledge, skill, and practice environment factors, with the exception of “access to an inserter in clinic.” Pediatricians as compared with FP-ObGyns were significantly less aware of professional guidelines about IUDs and adolescents (32% compared with 60%). In the past year, fewer pediatricians had ever discussed IUDs with an adolescent (70% with 89%), no pediatrician had inserted an IUD, whereas 65.3% of FP-ObGyns inserted an IUD for any patient and 39.1% had done so for an adolescent. Pediatricians scored lower on the overall counseling competency scale, as well as on each of its component measures (Figure 2).

Perceived competence to provide intrauterine device (IUD) counseling and management among pediatricians and family physicians and obstetrician-gynecologists.*
Within-Group Factors Associated With “Frequently” Counseling About IUDs, by Provider Group
Among pediatricians, factors associated with frequent IUD counseling included having access to an IUD inserter (P = .04), a higher IUD counseling competency scale score (P < .001), and a belief that adolescents’ use of prescription contraception does not lead to decreased condom use (P = .05) (Table 2).
Factors Associated With Bronx Primary Care Providers Reporting That They Frequently Counsel Female Adolescents About Intrauterine Devices (IUDs) During a Typical Office Visit Conversation About Contraception. a

Totals may vary due to missing data.
Fischer’s exact test (2-sided).
Question was asked only of those respondents who had not inserted an IUD in the past 12 months. This includes all pediatricians, and 34 family physicians and Obstetrician-Gynecologists (21 who frequently discuss, and 13 who do not frequently discuss IUDs).
Three-item Competency Scale based on the responses to the following 3 separate questions: Degree to which you feel competent (1) counseling about IUDs, (2) answering patient questions about IUD, and (3) managing expected IUD side effects.
Among FP-ObGyns, factors significantly associated with our counseling outcome included the following: awareness of professional guidelines (P = .005), currently inserting IUDs (P < .001), a higher competency scale score (P < .001), belief that adolescents’ use of prescription contraception does not lead to decreased condom use (P = .03), belief that adolescents’ use of an IUD as compared with oral contraceptive pills does not decreases condom use (P < .001), and strong disagreement that prescribing contraception for adolescents increases STI risk (P = .003).
Discussion
Primary care providers often provide reproductive health services, including contraception counseling and prescription for adolescents. Yet little is known about the frequency and factors associated with such practices for IUDs—a safe, highly effective contraceptive shown to decrease adolescent pregnancy.4,5 Ours is one of the first studies to examine this issue. In our survey of primary care pediatricians, FPs, and ObGyns, we found differences by PCP grouping both in the frequency with which IUDs are discussed and with factors associated with frequent counseling. Overall, we found that our pediatrician respondents worked more clinical sessions and reported a larger proportion of visits with female adolescents, yet they counseled less frequently, and felt less competent with counseling. Among our FP-ObGyns respondents, counseling competency as well as attitudes and beliefs about STIs and condom use were associated with IUD counseling frequency. For both groups, inserting IUDs or having access to an IUD inserter is also essential. Our results suggest that in order to increase IUD counseling for adolescents in primary care, we should consider interventions that strengthen PCPs’ competency and address systems issues to improve access to inserters.
Pediatricians’ less frequent and lower perceived competence in counseling compared to FP-ObGyns aligns with the literature. Other than our previous qualitative work, 16 the only published IUD study we found comparing these PCP types involved adolescent-medicine focused PCPs and focused on IUD provision, not counseling. Residency training in FP or ObGyn (rather than pediatrics or internal medicine) was the strongest predictor of providing IUDs. 26 Massachusetts pediatricians reported that lack of training and limited experience were barriers to their IUD counseling. 17 Taken together, it appears that interventions aimed at specifically increasing Pediatricians’ competency in counseling about the IUD and managing expected side effects appears to be “low hanging fruit.” These interventions may occur as an integrated part of clinical training as well as through point-of-care support tools, continuing medical education and connections with colleagues. Consistent with our findings, others have found that counseling frequency is increased by being an IUD inserter oneself 20 or having in-clinic access to one. 27 Thus, establishing systems to ensure availability of IUD inserters at all primary care sites, including pediatrician-staffed sites and/or establishing a strong referral network also appears likely to be key to increasing access.
Contrary to what we anticipated with regard to training, in our sample, inserting an IUD during training is not associated with frequently counseling. Possible reasons for this include lack of statistical power and/or insufficient sensitivity in question phrasing. Future studies might explore whether there is a “threshold” number of insertions that is associated with frequent counseling posttraining and/or posttraining insertion.
Our exploratory study has a number of limitations. This convenience sample from one institution is not representative of the US PCP population. Our modest sample size limits our power, does not allow us to assess ObGyns separately from FPs and it precludes multivariable analyses. Additionally our response rate, while not unusually low for a clinician survey, likely results in some selection bias.
Notwithstanding these limitations, this study of PCPs in one high-risk urban area provides new insights into why some PCPs are more likely than others to counsel adolescents about IUDs. We suggest that in order to increase counseling competency for all PCP groups, training in full-scope contraception counseling including IUD counseling (separate from procedural training in IUD insertion) should occur during residency training. Recent guidelines supporting adolescents’ use of IUDs,6,7 including the 2014 American Academy of Pediatrics’ Policy Statement on Contraception for Adolescents, 9 which encourages discussion of the most effective contraceptives such as IUDs as a first line option may begin to change training. For PCPs post-training, disseminating tools such as the Centers for Disease Control and Prevention’s Medical Eligibility Criteria for Contraception Use 8 and Selected Practice Recommendations for Contraceptive Use 28 as well as improved access to colleagues knowledgeable in IUD management may increase competency. It also appears important for all PCP types to insert IUDs themselves or have access to an inserter, either on-site or through an established, reliable referral system. Changing erroneous attitudes and belief will be more challenging. Our finding that correlates of frequent counseling vary by PCP type, suggests that optimal interventions designed to increase counseling would need to be tailored to meet the respective specific and distinct needs of Pediatricians and FPs and ObGyns. If successful, these interventions could increase access to IUDs for adolescents in primary care practices.
Footnotes
Acknowledgements
We would like to thank Giselle Campos for her assistance with data collection and Josephine Barnett with her help on data analysis and manuscript preparation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project is funded through NIH NICHD K23HD067247-01 (Rubin).