
Abstract
Introduction
Influenza remains a leading cause of vaccine-preventable hospitalizations and death.1,2 Current Canadian guidelines recommend universal influenza vaccination, but specifically note the importance of vaccinating certain high-risk groups, including those older than 65 years and those with chronic lung disease. Despite public health campaigns to encourage influenza vaccination, adherence rates remain low. In 2012, only 28.9% of Canadians and 31.1% of Ontarians received the flu shot. 3
Homeless individuals suffer from a disproportionately high burden of respiratory illness and are likely to benefit from influenza vaccination. 4 Because of high rates of smoking, chronic lung disease, poor nutrition, and crowded living conditions, homeless individuals are at increased risk for communicable respiratory diseases, including influenza.4-7 While influenza vaccination rates are known to be particularly low among marginalized urban populations, very little information is available on the rate of influenza vaccination in homeless populations in Canada.8,9 The objective of this study was to determine the rate of documented influenza vaccination in a cohort of homeless adults with mental illness in Toronto. There are more than 5000 homeless people in Toronto on any given night, with an estimated 38% experiencing current mental health problems.10,11 This study was conducted in a subsample of participants in the At Home/Chez Soi Study, a multicity randomized controlled trial investigating the effectiveness of a Housing First intervention for people who are homeless and have mental illness.
Methods
A total of 575 individuals who were homeless and had mental illness were enrolled at the Toronto site of the At Home/Chez Soi Study from October 2009 to July 2011. Details of the research protocol have been previously published. 12 A random sample of 200 study participants was selected for chart review. The research team sought to review primary care medical records for these 200 participants from the year preceding enrollment in the study. Participants were asked to provide information on primary or ambulatory care received in the previous 18 months and consent for release of their medical records.
Charts were sought using physician contact information provided by participants or obtained from the College of Physicians and Surgeons of Ontario Web site. Physicians received a faxed request for information and the participant’s signed consent for release of relevant medical records. Up to 5 follow-up phone calls were placed to request charts. The charts were obtained by various methods, including faxed or mailed copies, review of electronic medical records, and examination of charts at the physician’s office. Data were abstracted using a standardized form to obtain information on diagnoses and preventive care interventions including influenza vaccination. To ensure reliability, a random 5% sample of charts were reviewed independently by 2 researchers.
Results
Of 200 participants, 3 did not consent to have their records released; 10 had not received any medical care or were unable to provide information on where they received care in the past 2 years; and 112 provided information for doctors who could not be located or did not provide primary care (usually a psychiatrist). In total, charts were obtained for 75 of 200 participants (37.5%); some participants had medical charts obtained from multiple primary care sources. Baseline demographic data for these participants are shown Table 1.
Baseline Characteristics.
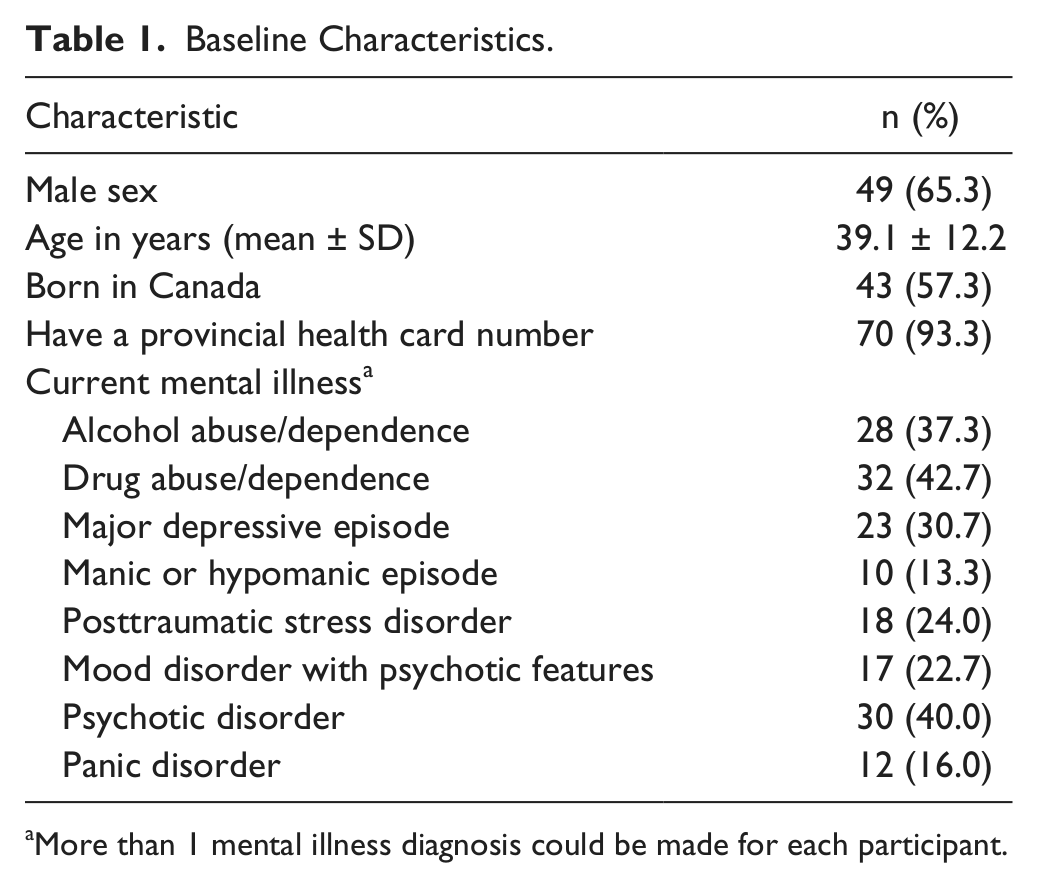
More than 1 mental illness diagnosis could be made for each participant.
Of 75 participants whose charts were reviewed, 5 (6.7%) had documentation indicating receipt of the influenza vaccination in the year prior to study entry. The remaining 70 (93.3%) had no documentation of receiving the influenza vaccination in their primary care chart.
Discussion
Vaccination represents one of the most successful public health interventions at the primary care level; the influenza vaccination is a cost-effective, proven method of decreasing respiratory illness complications and mortality 2 . Results of this study suggest that a very low proportion of homeless adults with mental illness are receiving this intervention. The rate of influenza vaccination (6.7%) in this cohort of homeless adults with mental illness was less than one quarter of the vaccination rate among all Canadians (28.9%). 3
There are certain limitations to this study. The sample size is small, predominantly because of participants’ inability to recall their primary care providers or a lack of contact with a primary care physician. This again highlights the limited access of homeless and mentally ill patients to primary care; in the general homeless population of Toronto, 43% report having a family physician, 13 and the average annual number of primary care visits is 8 and 10 among homeless men and women, respectively. 11 Second, this study includes only homeless adults with mental illness. The negative health consequences of homelessness tend to be more severe and access to primary care more limited in homeless individuals with mental illness when compared with those without mental illness. 13 It is estimated that more than one third of homeless adults suffer from mental illness; thus, these individuals represent a significant proportion of the overall homeless population. 14
Importantly, the chart review methodology may not capture influenza vaccinations received outside the primary care setting, such as at community “flu clinics.” Toronto Public Health operates such clinics on approximately 14 days each year, but most clinics are not located in areas of the city where there are large numbers of homeless people, and in our experience very few homeless individuals report using these clinics. Finally, it is unknown how many patients were offered but declined a flu shot, rather than were not offered it at all. Nonetheless, the results of this study indicate that few of the homeless participants with mental illness successfully received an influenza vaccination from their primary care provider.
Conclusions
The extremely low proportion of homeless individuals in this study who received the influenza vaccination from their primary care provider is concerning given the high risk for morbidity in this group. Our results indicate a rate of vaccination much lower than several other studies done in US homeless populations that observed vaccination rates of between 21% and 35%.15-18 This study represents one of the few estimates of the rate of influenza vaccination among homeless adults in a Canadian population. Receiving the influenza vaccination is determined by many factors, including access to health care and personal views toward vaccination. 8 It cannot be determined from this study what factors may have contributed to the low vaccination rate. Further research into the causes of low influenza vaccination rates among homeless Canadians is needed to generate strategies for increased vaccination delivery. Increased awareness among family physicians of the importance of influenza vaccination for homeless individuals is an important first step in primary prevention of influenza and its sequelae.
Footnotes
Acknowledgements
The authors thank the Toronto site research team, including research coordinators, research assistants, People With Lived Experience group members, service support providers, and participants for their contributions to the ongoing success of this study. The authors would like to acknowledge the national At Home/Chez Soi project team: Jayne Barker, PhD, and Cameron Keller, MHCC National Project Leads; Paula Goering, RN, PhD, Research Lead; approximately 40 investigators from across Canada and the United States; site coordinators in 5 cities; numerous service and housing providers; and persons with lived experience.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research has been made possible through a financial contribution from Health Canada and funded by the Mental Health Commission of Canada.