
Abstract
Objectives:
Patients experiencing homelessness (PEH) with serious mental illness (SMI) have poor satisfaction with primary care. We assessed if primary care teams tailored for homeless patients (Homeless-Patient Aligned Care Teams (H-PACTs)) provide this population with superior experiences than mainstream primary care and explored whether integrated behavioral health and social services were associated with favorable experiences.
Methods:
We surveyed VA PEH with SMI (n = 1095) to capture the valence of their primary care experiences in 4 domains (Access/Coordination, Patient-Clinician Relationships, Cooperation, and Homeless-Specific Needs). We surveyed clinicians (n = 52) from 29 H-PACTs to elucidate if their clinics had embedded mental health, addiction, social work, and/or housing services. We counted these services in each H-PACT (0-4) and classified H-PACTs as having high (3-4) versus low (0-2) service integration. We controlled for demographics, housing history, and needs in comparing H-PACT versus mainstream experiences; and experiences in high versus low integration H-PACTs.
Results:
Among respondents, 969 (91%) had complete data and 626 (62%) were in H-PACTs. After covariate adjustment, compared to mainstream respondents, H-PACT respondents were more likely (P < .01) to report favorable experiences (AORs = 1.7-2.1) and less likely to report unfavorable experiences (AORs = 0.5-0.6) in all 4 domains. Of 29 H-PACTs, 27.6% had high integration. High integration H-PACT respondents were twice as likely as low integration H-PACT respondents to report favorable access/coordination experiences (AOR = 1.7).
Conclusions:
Homeless-tailored clinics with highly-integrated services were associated with better care experiences among PEH with SMI. These observational data suggest that tailored primary care with integrated services may improve care perceptions among complex patients.
Introduction
Patients with serious mental illness (SMI, including psychotic disorders and bipolar disorders) are 10 to 20 times more likely to experience homelessness than the general population. 1 Unfortunately, patients experiencing homelessness (PEH) with SMI have high rates of chronic disease, increased morbidity/mortality, fragmented service use, poor primary care experiences, and social isolation.2-10 Regardless of housing status, patients with SMI often struggle to navigate medical care2,7; they may report dissatisfaction with access to primary care and the coordination of services received. 11 In light of perceived discrimination reported by PEH in primary care,12,13 and the central role of primary care in addressing the mortality gap for persons with SMI, 14 there is a pressing need to identify clinic paradigms that optimize care experiences for PEH with SMI.
There are several reasons why primary care experiences are critical for these patients. First, these experiences are associated with medication adherence.15-17 Second, negative primary care perceptions often contribute to suboptimal service engagement, 18 leading to increased Emergency Department utilization and hospitalizations. Third, positive primary care experiences are linked to improved outcomes for some chronic conditions.2,6,7 As such, healthcare systems have increasingly embraced patient experience as a key indicator of quality of care.2,19,20
Though some programs could optimize primary care experiences for PEH with SMI, doing so requires identifying and implementing relevant service design features. For example, the Health Care for the Homeless program 21 has run for >3 decades; some of these programs deliver homeless-tailored services while others do not. To date, some surveys support the value of tailored primary care for PEH.6,22-24 However, research to understand which service design features influence patient experience is limited; this resource-intensive work requires collecting patient- and staff-level information from large numbers of clinics that vary in meaningful ways.
The Veterans Administration (VA) provides one opportunity to fill this gap. In 2012, the VA implemented Homeless-Patient Aligned Care Teams (H-PACTs), patient-centered medical homes tailored for PEH. 25 These teams operate at >60 VAs; dependent on the site, “tailored” care may include service delivery in non-traditional locations (eg, streets), practices that increase access (eg, walk-in services), tangible services (eg, clothing), and various levels of integration of social services and behavioral health care. 25 Ultimately, H-PACTs were developed to engage the VA’s most vulnerable PEH, including those with SMI.
This paper examines primary care experiences reported by PEH with SMI. First, using patient surveys, we assessed if H-PACTs provide this population with superior care experiences than mainstream primary care. Then, adding data from a survey of clinic staff, we examined whether one aspect of service design—having behavioral health and social services embedded within primary care—contributes to superior H-PACT experiences. Ultimately, this study aimed to inform primary care paradigms that enhance care experiences for PEH with SMI.
Methods
These analyses are part of the Primary Care Homeless Services Tailoring study, 26 a national survey of PEH who receive primary care at 26 VAs with both H-PACTs and mainstream primary care (“mainstream”), with the goal of offering an observational comparison of care experiences in these 2 settings. Study procedures were approved by VA’s Central Institutional Review Board.
Setting
The VA is an integrated healthcare system that offers primary care, mental health services, and specialty medical and surgical care. VA primary care is delivered in patient-centered medical homes,27,28 with patients assigned to primary care providers embedded in teams with nurse care managers and ancillary staff. All primary care teams (PACTs) aim to deliver patient-centered and comprehensive primary care, including screening and preventive services. 29 Some PEHs receive primary care in mainstream PACTs while others receive care in H-PACTs, which are designed to address social determinants of health and facilitate housing. 24
Participants
Survey recruitment is detailed elsewhere. 26 VA patients were eligible if they: (a) received ≥2 primary care visits at a study site; (b) had evidence of homelessness between May 2015 and November 2017 30 (ICD-9/ICD-10 diagnoses of homelessness or VA-specific indicators of receipt of homeless services) in VA’s national electronic medical record (EMR) and c) were assigned to a single primary care team. Among eligible patients (n = 57 220), sampling was stratified by facility and type of primary care (H-PACT vs mainstream); 14 340 patients (derived from projected response rates and power calculations) were randomly selected at a 2:1 H-PACT to mainstream ratio. Participants were excluded if they had no available contact information or were deceased prior to the start of the survey. A professional survey organization, Strategic Research Group of Columbus, Ohio, conducted recruitment and survey collection in 4 waves of 4 to 6 weeks/each between March and October 2018, cross-referencing patients’ VA contact information with data from a commercial address verification database (MelissaData). Each wave included a pre-notification letter, a survey with $1 pre-incentive, a reminder postcard, and a second survey for non-responders. The survey organization called non-responders up to 5 times during a 1-month period with the option to complete the survey by telephone. PEH who completed the survey (n = 5766, 40.2%) received $10. Next, using VA administrative data, we identified respondents who had at least 1 ICD-9/ICD-10 code for schizophrenia spectrum disorders, bipolar spectrum disorders, or other psychotic disorders (Supplemental Material Online) 31 in VA’s national EMR between May 2015 and November 2017 (n = 1095, 19% of respondents).
We also conducted telephone-based surveys with the lead nurse and prescriber (primary care physician or physician extender) at participating H-PACTs; 52 of 58 (89.7%) lead nurses and prescribers from 29 H-PACTs were surveyed.
Conceptual Framework
This study was guided by the Behavioral Model for Vulnerable Populations, 32 which models health care use among vulnerable populations and is widely used with PEH33,34 and persons with SMI.35,36 This framework identifies factors that predispose individuals to access services (demographics, homelessness chronicity), which interact with enabling factors (primary care clinic type, clinic characteristics) and needs for services to influence behaviors (service use) and outcomes (patient experience). 32
Measures
Covariates
To adjust for measurable differences among respondents’ who received care in H-PACT versus mainstream primary care, the patient survey assessed factors that predispose patients to use services, including demographics (age, race, ethnicity, marital status, educational attainment), housing history (≥1 night in the past 6 months spent outside or in a place not meant for sleeping), and chronic homelessness (≥4 episodes of homelessness in the past 3 years or ≥1 episode of homelessness of ≥1 year). 37 Patients’ need for primary care was captured with a self-reported count of 8 medical conditions administered in the survey (diabetes, hypertension, coronary artery disease, myocardial infarction, stroke, asthma, emphysema, arthritis, derived from the Medical Expenditure Panel Survey’s satisfaction studies) 38 and SMI diagnoses were identified using VA EMR data. The presence of current alcohol or drug problems was assessed via survey with the Two-Item Conjoint Screening test. 39
Enabling characteristics
We also examined factors that enable or impede service use. Our key comparison was care experiences in H-PACT versus mainstream clinics, determined from VA’s national EMR.
The clinician survey assessed clinic characteristics that could contribute to differences in patient experience by primary care setting. These analyses focused on the presence or absence of mental health, addiction treatment, social work, and housing services within the H-PACTs. We asked clinicians to identify if each of the 4 types of services were provided: within H-PACT; outside H-PACT but within brief walking distance; or not provided within H-PACT or within brief walking distance. We classified responses as within or outside H-PACT, as services outside H-PACT but within walking distance seemed substantively different than services within the H-PACT. As surveys were conducted with 2 clinicians per H-PACT, we cross-checked responses by facility. If different responses were provided by the nurse and prescriber, we assigned the more conservative response (ie, outside H-PACT).
To capture the contributions of service integration on care experiences, we counted the number of services in each H-PACT (0-4), then classified H-PACTs as having high (3-4) or low (0-2) service integration based on the number of embedded services.
Outcome
Primary care experience was assessed in the patient survey, using the Primary Care Quality-Homeless (PCQ-H) questionnaire, 40 a 33-item instrument developed and validated for PEH. The PCQ-H is detailed elsewhere 40 ; it uses Likert scales (1-4) to capture primary care experience in 4 domains: access/coordination; patient-clinician relationship; perceived cooperation among clinicians; and homeless-specific needs. In each domain, the PCQ-H offers a categorical indicator for favorable experiences based on the top tertile of respondents and a categorical indicator for unfavorable experiences based on the lowest tertile of respondents.
Analyses
The sample consisted of PEH with SMI and complete data on study variables (n = 969, 91%). Analyses were performed in Stata version 15.1. First, we compared respondents assigned to H-PACT (626, 64.6%) versus mainstream (343, 35.4%). We used chi-square and analysis of variance tests to assess between-group differences in predisposing, enabling, and need factors, then the outcome of favorable and unfavorable primary care experiences.
Next, we used multivariable logistic regressions to test for differences between H-PACT versus mainstream respondents in favorable and unfavorable experiences. These models controlled for study covariates and were weighted for non-response (the inverse probability of response, modeled from VA clinical records data).
To explore whether service integration was a factor in primary care experience, we reran the multiple logistic regression models comparing respondents from 3 groups: high integration H-PACTs (3-4 embedded services); low integration H-PACTs (0-2 embedded services); or mainstream. We used Wald tests to assess pairwise clinic differences (eg, high integration H-PACTs vs low integration H-PACTs) in favorable and unfavorable experiences.
Sensitivity analyses
We assessed if study patterns persisted with alternate definitions of service integration. Focused on the subsample of H-PACT respondents (n = 626), we first used mixed effect logistic regressions to test for associations between the count of embedded services (0-4) with favorable and unfavorable experiences. The models included fixed effects for number of embedded services and respondent covariates, and a random effect for site. Second, we tested whether specific embedded services were associated with favorable and unfavorable experiences. The models included a fixed effect indicator for the embedded service and respondent covariates, and a random effect for site.
Results
Table 1 describes H-PACT versus mainstream respondents across predisposing and need factors. H-PACT respondents differed from their mainstream counterparts (P < .05) in several ways. Specifically, H-PACT respondents were younger (12.1%/25.1% were ≥65 years), less likely to be female (6.9%/15.5%), and less likely to be married (13.1%/19.8%). More H-PACT versus mainstream respondents had a history of chronic homelessness (27.6%/12.5%) and self-reported drug problems (21.7%/16.3%). About one-third of respondents (37.6%) had diagnoses of psychotic disorders; 56.0% had bipolar illness. There were no significant between-group differences in the self-reported number of chronic medical conditions; fewer (P < .05) H-PACT respondents self-reported diabetes than their mainstream counterparts (22.4%/28.6%).
Characteristics of Homeless-Experienced Respondents with Serious Mental Illness Who are Assigned to H-PACT vs VA Mainstream Clinics.

P < .05, P-values obtained from chi-square tests of differences between patients in H-PACT and mainstream clinics.
SMI diagnoses reflect diagnoses in the administrative data associated with visits in the 24 months preceding May 2015 to November 2017; participants may have ≥1 associated SMI diagnosis.
Table 2 presents the outcome of primary care experiences by PCQ-H domain and clinic type. Compared to mainstream respondents, H-PACT respondents had higher rates of favorable primary care experiences and lower rates of unfavorable experiences in all 4 PCQ-H domains (P < .05). Differences in rates of favorable experiences were particularly pronounced in access/coordination (45.3%/28.4%), followed by homeless-specific needs (39.9%/25.1%), the patient-clinician relationship (45.2%/33.8%), and cooperation (38.0%/30.9%). Differences in rates of unfavorable experiences were largest in homeless-specific needs (42.7%/59.3%), followed by the patient-clinician relationships (28.9%/38.9%), access/coordination (27.7%/37.5%), then cooperation (27.9%/37.3%).
Primary Care Experiences Among Homeless-Experienced Respondents with Serious Mental Illness Assigned to H-PACT vs Mainstream Clinics.
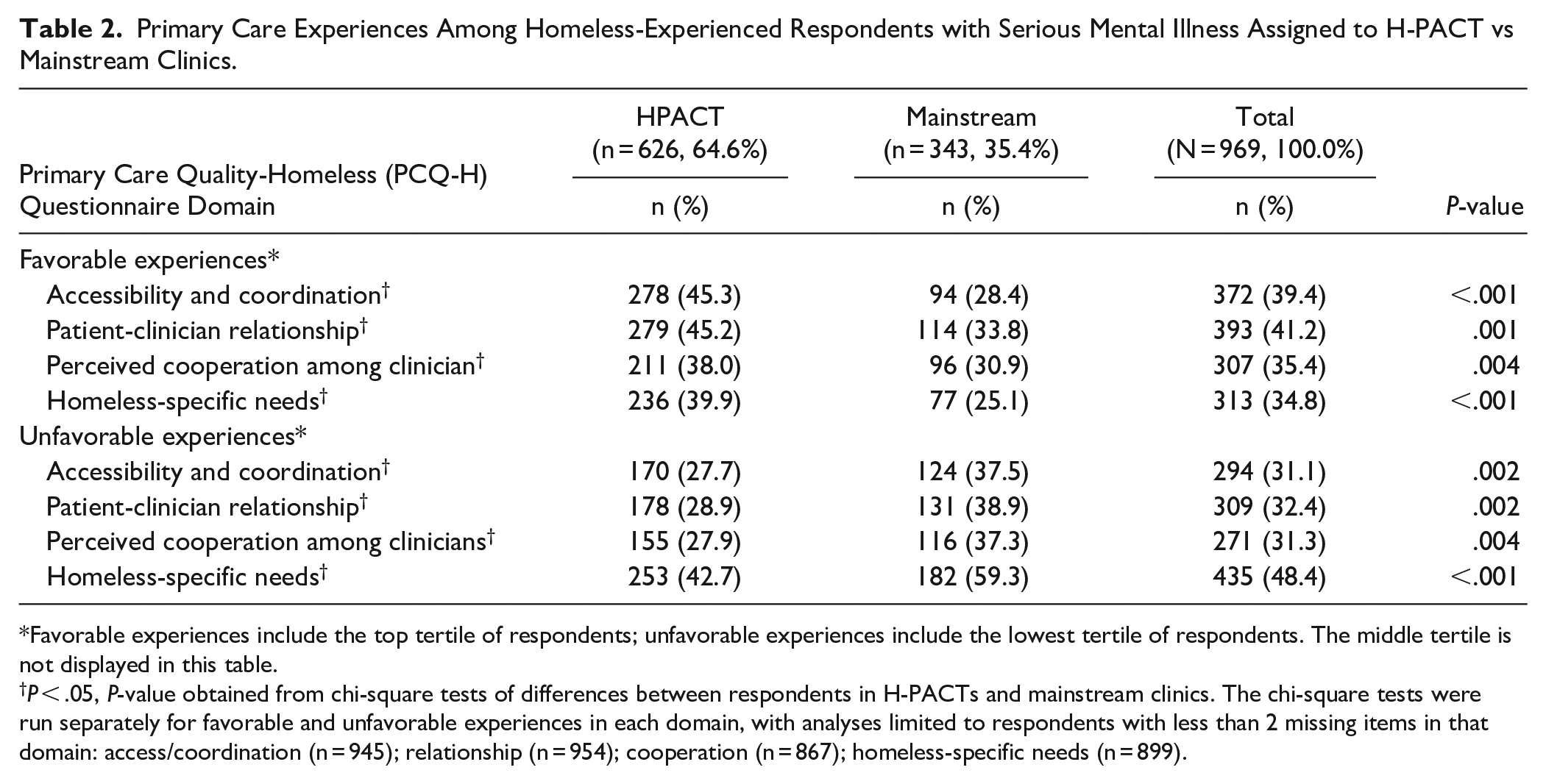
Favorable experiences include the top tertile of respondents; unfavorable experiences include the lowest tertile of respondents. The middle tertile is not displayed in this table.
P < .05, P-value obtained from chi-square tests of differences between respondents in H-PACTs and mainstream clinics. The chi-square tests were run separately for favorable and unfavorable experiences in each domain, with analyses limited to respondents with less than 2 missing items in that domain: access/coordination (n = 945); relationship (n = 954); cooperation (n = 867); homeless-specific needs (n = 899).
Table 3 displays these data adjusted for predisposing characteristics (age, gender, race, ethnicity, marital status, educational attainment, and housing history) and need (count of self-reported medical problems and presence of current alcohol/drug problems). Compared to the mainstream group, H-PACT respondents were more than twice as likely to report favorable experiences in access/coordination and homeless-specific needs (adjusted odds ratios (AOR) = 2.2/2.1); and nearly twice as likely to report favorable patient-clinician relationships and cooperation (AOR = 1.9/1.7). Similarly, compared to their mainstream peers, H-PACT respondents were about half as likely (AOR 0.5-0.6) to have unfavorable experiences in each PCQ-H domain.
Logistic Regression of Primary Care Experiences among Homeless-Experienced Respondents with Serious Mental Illness in H-PACT vs Mainstream Clinics.

Logistic regression models, run separately for each domain, were weighted for non-response (calculated as inverse probability of response) and controlled for predisposing characteristics (age, gender, race, ethnicity, marital status, educational attainment, housing history) and need (count of 8 self-reported medical conditions and presence of current alcohol or drug problems). The adjusted percentages are model-derived predicted probabilities, holding covariates at their mean values. All AORs were statistically significant at P < .05.
Favorable experiences include the top tertile of respondents; unfavorable experiences include the lowest tertile of respondents. The middle tertile is not displayed in this table.
Considering respondents from high integration H-PACTs, low integration H-PACTs, and mainstream, Table 4 presents pairwise differences in favorable and unfavorable experiences. High integration H-PACT respondents were 1.7 times as likely to have favorable access/coordination (P < .05) than low integration H-PACT respondents. No other statistically significant findings were revealed in comparing high versus low integration H-PACT respondents. In all 4 domains, high integration H-PACT respondents were significantly (P < .05) more likely than their mainstream peers to report favorable and/or less likely to report unfavorable experiences. For example, high integration H-PACT respondents were 3.5 times as likely to report favorable access/coordination and 2.1 times as likely to report favorable homeless-specific needs than mainstream respondents. Even low integration H-PACT respondents were about 2 times as likely (AOR = 1.8-2.1) as mainstream respondents to have favorable experiences in all 4 domains (P < .05).
Logistic Regression of Primary Care Experiences among Homeless-Experienced Respondents with Serious Mental Illness in High Integration H-PACTs vs Low Integration H-PACTs vs Mainstream Clinics.
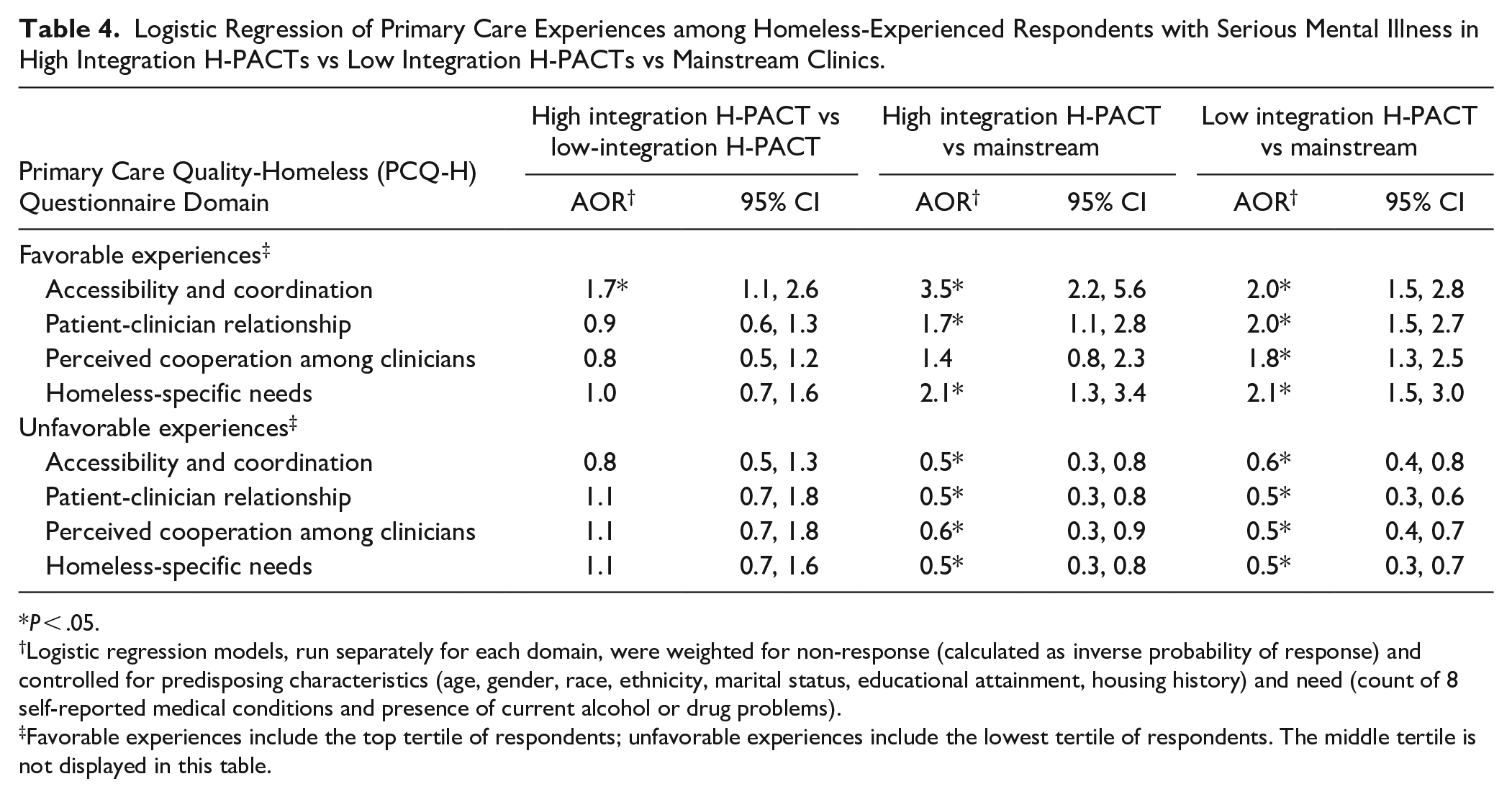
P < .05.
Logistic regression models, run separately for each domain, were weighted for non-response (calculated as inverse probability of response) and controlled for predisposing characteristics (age, gender, race, ethnicity, marital status, educational attainment, housing history) and need (count of 8 self-reported medical conditions and presence of current alcohol or drug problems).
Favorable experiences include the top tertile of respondents; unfavorable experiences include the lowest tertile of respondents. The middle tertile is not displayed in this table.
Regarding service integration in H-PACTs, surveys with nurses and prescribers revealed that most clinics had embedded social work (n = 22, 75.9%) and mental health care (n = 17, 58.6%). Fewer clinics had integrated housing (n = 8, 27.6%) and addiction treatment (n = 3, 10.3%) services. Just over a quarter (27.6%) of participating H-PACTs had high service integration (3-4 embedded services); most (72.4%) had low service integration (0-2 embedded services).
Table 5 depicts our sensitivity analyses. In analyses that considered the count of embedded services, the number of services integrated into H-PACTs was positively associated with favorable experiences in access/coordination (AOR = 1.4). When specific embedded services were examined, only housing services were significantly associated (P < .05) with respondent experiences within H-PACTs. Specifically, respondents receiving services in H-PACTs with embedded housing services were more than 2 times (AOR = 2.4) as likely as respondents in H-PACTs lacking embedded housing services to report favorable experiences with access/coordination. None of the other embedded services (mental health, social work, addiction) were statistically associated with favorable/unfavorable care experiences in any domain.
Sensitivity Analyses Testing Associations of Number of Services, then Specific Embedded Services, with Favorable and Unfavorable Primary Care Experiences among Homeless-Experienced Respondents with Serious Mental Illness in H-PACTs.

P < .005.
Estimates derived from mixed effect logistic regressions. Each model included fixed effects for number of embedded services (0-4) and patient predisposing characteristics (age, gender, race, ethnicity, marital status, educational attainment, housing history) and need (count of 8 self-reported medical conditions and presence of current alcohol or drug problems), and site random effects.
Estimates derived from mixed effect logistic regressions. Each model included fixed effects indicator for the embedded service and patient predisposing characteristics (age, gender, race, ethnicity, marital status, educational attainment, housing history) and need (count of 8 self-reported medical conditions and presence of current alcohol or drug problems), and site random effects.
Favorable experiences include the top tertile of respondents; unfavorable experiences include the lowest tertile of respondents. The middle tertile is not displayed in this table.
Discussion
In this national survey of PEH with SMI receiving VA primary care, we found that assignment to primary care clinics tailored for homeless patients was associated with more favorable experiences than mainstream primary care. For PEH with SMI who received homeless-tailored primary care, the presence of specific behavioral health services was not associated with the valence of experiences. Rather, having more embedded services, that is, highly integrated clinics, was associated with favorable perceptions of clinic access/coordination.
While some prior studies have examined primary care tailoring for PEH, little attention has been given to primary care approaches for PEH with SMI. In this sample, PEH with SMI who received homeless-tailored primary care overwhelmingly endorsed better care experiences than their peers who received mainstream primary care. Tailoring features (eg, small panels, longer appointments) may be particularly important for vulnerable PEH, including those with SMI.
However, to serve this population with 2 vulnerabilities—SMI and homelessness—some may question the relative value of primary care tailored for PEH versus integration of primary care into mental health clinics.41,42 To this end, though SMI diagnoses predispose patients to homeless experiences,43–46 only a minority of patients with SMI become homeless. However, PEH with SMI have incredibly high needs and health disparities.2–10 Little is known about similarities and differences in pathways to homelessness for patients with and without psychiatric illness. One study suggests that PEH with mental illness have similar pathways to homelessness as their peers without psychiatric problems. 44 That is, homeless patients as a unified cohort may have more in common, regardless of diagnoses, than homeless versus housed patients with SMI. This idea supports the use of homeless-tailored primary care for PEH with SMI.
We were surprised that the presence of integrated behavioral health care (eg, addiction services) was not associated with more favorable experiences. One possibility is that the logistic demands of PEH dictate that the number of services available at a single site is more important than the types of services offered; this finding is buttressed by our models. Also, despite common enthusiasm for colocation or integration of primary and mental health care, 47 patients with SMI likely have a diversity of preferences. Some patients with SMI value specialty mental health care in ways that requires its identification as distinct from primary care. 48
Our finding that high-integration H-PACTs were associated with more favorable access/coordination experiences may have service design implications, particularly as it relates to implementing case management in primary care.49,50 From its inception, H-PACT was described as a one-stop model of care, where multiple and sometimes competing needs could be addressed in a single setting. 51 Our data suggest that PEH with SMI who receive primary care in “one-stop shops” with highly integrated services 52 —extending beyond the basics of primary care-mental health integration 53 to encompass social services—may have better care experiences. A recent study showed that enhancing case management in VA primary care was related to decreased Emergency Department utilization 54 ; our findings echo the benefits of amplifying this role within primary care to manage care coordination for complex patients. At the same time, managers have to determine if the benefits of implementing these services exceed the costs incurred.
This study had limitations. First, the VA has robust medical, psychiatric, and social services for PEH; extrapolating these findings to other settings and populations requires caution. However, these findings could prove useful for the Health Care for the Homeless program 21 or other settings that serve complex patients. Second, though our data derive from the largest survey of PEH to date, with a response rate (40.2%) that is about double what is reported for this population in VA’s standard patient experience methodology, 55 our survey respondents reflect a population that is engaged in care, with potentially fewer social vulnerabilities than other PEH with SMI. Third, these data reflect an observational study of PEH with SMI utilizing homeless-tailored versus mainstream primary care, as opposed to a randomized controlled trial that assigned PEH with SMI to homeless-tailored primary care services versus treatment as usual. The survey measures attempted to control a wide range of variables associated with patient-reported experience, but unmeasured confounders are not controlled. Fourth, in identifying relevant service design features, we focused on integration of behavioral health and social services; additional clinic features (eg, staffing, field-based services) are worthy of study. Last, though patient experience is associated with important outcomes for PEH with SMI, a central treatment goal for patients with SMI is to improve community functioning56–58; the relationships between patient experience and functioning are unexplored.
Conclusions
Experiences of homelessness and SMI diagnoses convey synergistic risks for morbidity and mortality. To address health disparities faced by PEH with SMI, we must identify and scale viable primary care models that are well-received by this population. This study suggests that, at least within the VA, PEH with SMI who receive care in homeless-tailored primary care clinics had more favorable care experiences than their peers who received primary care in mainstream settings. More favorable patient experiences do favor continued care engagement, but whether optimal health outcomes result from such engagement remains to be seen. Further research could explore other features of and adaptations to H-PACT that optimize care for PEH with SMI, moving beyond patient experience to explore additional important outcomes, including medication adherence, substance use disorder outcomes, and functioning.
Supplemental Material
sj-pdf-1-jpc-10.1177_2150132721993654 – Supplemental material for Enhancing Primary Care Experiences for Homeless Patients with Serious Mental Illness: Results from a National Survey
Supplemental material, sj-pdf-1-jpc-10.1177_2150132721993654 for Enhancing Primary Care Experiences for Homeless Patients with Serious Mental Illness: Results from a National Survey by Sonya Gabrielian, Audrey L. Jones, April E. Hoge, Aerin J. deRussy, Young-il Kim, Ann Elizabeth Montgomery, John R. Blosnich, Adam J. Gordon, Lillian Gelberg, Erika L. Austin, David Pollio, Sally K. Holmes, Allyson L. Varley and Stefan G. Kertesz in Journal of Primary Care & Community Health
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by VA HSR&D IIR 15-095-2 (PI: Kertesz). Dr. Gabrielian is supported in part by VA HSR&D Career Development Award 15-074. Dr. Jones is supported by the National Center for Advancing Translational Sciences of the National Institutes of Health under (award numbers UL1TR002538 and KL2TR002539). The views expressed in this article are those of the authors alone and do not represent the views of the United States Department of Veterans Affairs, the National Institutes of Health, or the United States Government.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.