
Abstract
Introduction
Consanguinity is a term that is derived from 2 Latin words “con” meaning common and “sanguineus” meaning blood, referring to a relationship between 2 biologically related individuals. In clinical genetics, a consanguineous marriage means union between couples who are related as second cousins or closer. Chances of inheritance of a mutant allele at the same locus is increased as both parents have a common ancestor. The closeness in relationship between the parents determines the extent of common genetic inheritance. Brothers and sisters share commonly 50% of their genetic make-up, uncle and niece share 25%, and first cousins 12.5% of their inherited genetic material. 1 Children of such a marriage therefore are at a greater risk of being homozygous for a harmful gene and consequently suffer from autosomal recessive genetic disorders. This leads to increased risk of infant deaths as reported by studies done in different parts of India. 2
In the background of declining mortality and morbidity due to infectious disease seen in India, recessive genetic disorders will progressively gain greater prominence in the days to come. 2
As per the national family health survey report there has been only a modest reduction in the prevalence of consanguineous marriages over the years. 2 This supports the fact that such marriages form an integral part of cultural and social life in India and southern states in particular have witnessed a high frequency of such marriages. Therefore attempts to discourage it may be inappropriate and undesirable for many. But considering its role as a critical predictor of adverse fetal outcomes, birth defects, morbidity, and mortality in children contributed by recessively inherited disorders, it is essential to create awareness regarding its adverse effects so as to avoid such marriages taking place in future. 3
Very few studies have been done before in this field from this region. Also none of these available studies could establish an association with congenital anomalies. Moreover, these studies have not comprehensively analyzed the association of sociodemographic variables but for religion and caste with history of consanguinity.4,5 Hence it was essential for us to address these inadequacies so as to plan appropriate preventive strategies among identified risk groups. Another drawback of previously done studies in this field elsewhere in India was that majority were hospital based. As people visit hospitals from any geographical area, the true magnitude of this social problem and pattern of resulting congenital anomalies in a particular community cannot be estimated from such studies. Moreover, as hospitals have no defined catchment area, it is not possible for authorities to plan appropriate remedial measures based on the findings of such studies. This community based study was hence done to find out the awareness of people regarding the ill effects of consanguinity, to determine the prevalence (magnitude) and type of consanguineous marriages, and to study its association with various sociodemographic variables and complications among children in South Canara district of Karnataka state in south India.
Methods
The present study was conducted in 2 urban areas, namely Shiva Nagar and Jeppinamogaru, and 1 rural area, namely Ullal, the field practice areas of Department of Community Medicine, Kasturba Medical College, Mangalore. The study was done in January 2013 among all the married permanent residents residing in the study area. A sample size of 178 respondents was chosen from as many houses, considering the expected prevalence of consanguineous marriages to be 36% from the findings of another study done in Karnataka state 4 and keeping the power at 80% with 95% confidence intervals. To balance the selection in number of houses among the 3 areas, 40% were targeted from the rural area and 30% each from the 2 urban areas. These houses were chosen by systematic random sampling method in which every 10th house (starting from the first house chosen simple randomly) in a randomly chosen lane was surveyed. In case the house was locked or members were ineligible for inclusion in this study or were nonconsenting, the adjacent house was selected. The investigators then interviewed either of the spouse present at the time of visit using a predesigned structured interview schedule. In case both parents were present, the women were preferred to get more accurate details on maternal and child health outcomes. Written informed consent was obtained for participation after explaining to them the nature and purpose of the study. Left thumb impression was taken for obtaining consent from illiterates. Family pedigree was constructed up to fifth-degree relatives to study the type of consanguineous relationship in marriage. Birth weight and diagnosis of neonatal complications were verified from the medical records available with the respondents. In case of disparity between information given in medical records and as told by the participants, the information given in medical records was taken as final. If medical records were unavailable, then history given by the participant was recorded as final. Awareness regarding adverse effects of consanguineous marriage and its outcomes in children were assessed among participants by asking open-ended questions. Socioeconomic status was assessed using modified Kuppuswamy’s classification of 2012. 6 Data entry and analysis were done using SPSS version 16 (SPSS Inc, Chicago, IL). Chi-square test was used to test association. P ≤ .05 was taken as statistically significant association.
Results
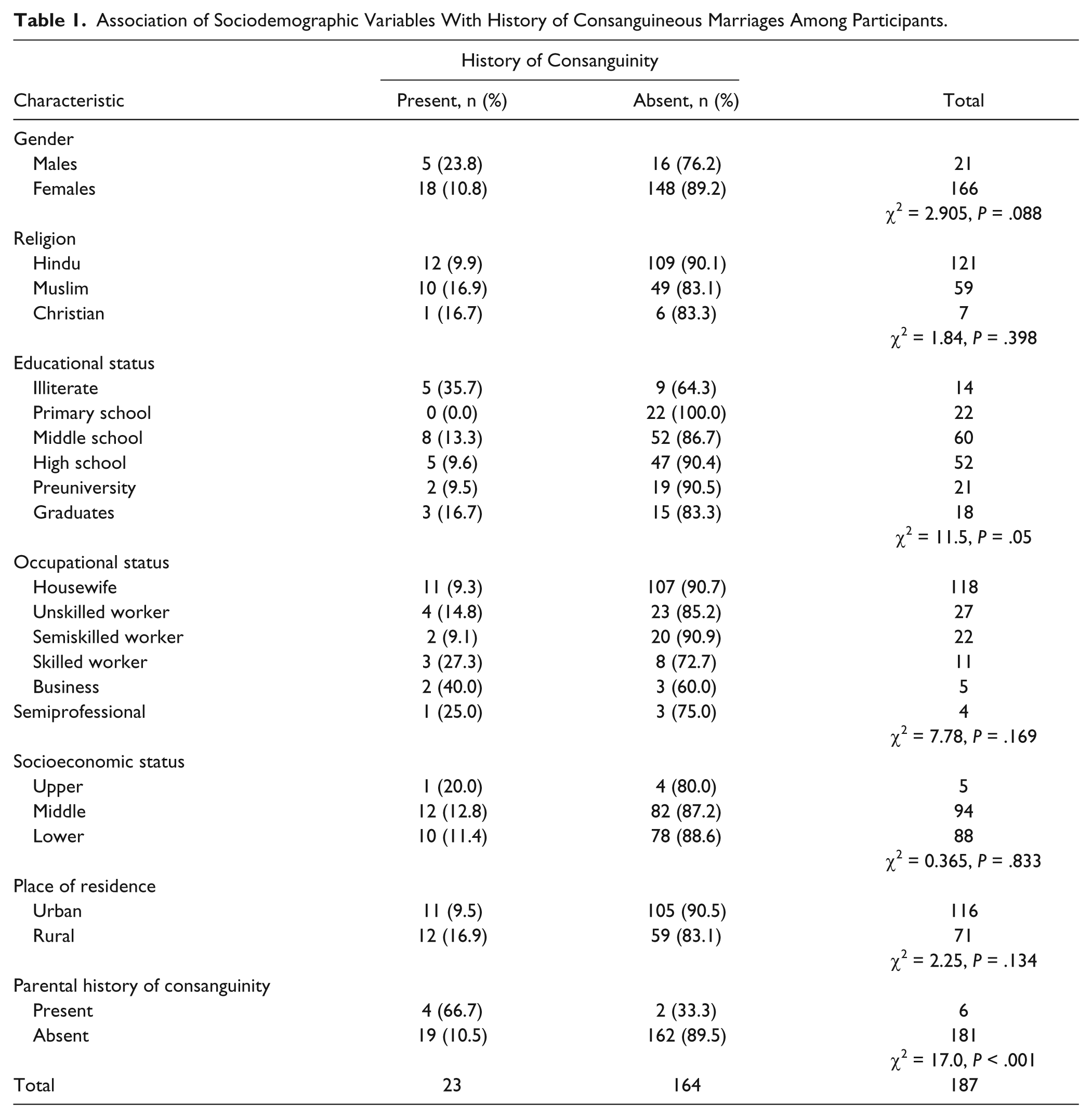
Majority of the 187 participants, 59 (31.6%) were of the age group 30 to 39 years followed by 55 (29.4%) of the age group 20 to 29 years, 44 (23.5%) of the age group 40 to 49 years, 23 (12.3%) of the age group 50 to 59 years, and rest were aged 60 years or older. Mean age of participants was 38.8 ± 10.9 years. Most participants were females 166 (88.8%) and housewives by occupation, 118 (63.1%). Hindus constituted 121 (64.7%) and 94 (50.3%) participants were of the middle socioeconomic status. Majority 60 (32.1%) were educated up to middle school and majority were from urban areas 116 (62%) (Table 1).
Association of Sociodemographic Variables With History of Consanguineous Marriages Among Participants.
Among male participants, 2 (9.5%) were illiterate, 15 (71.4%) were educated till school level, 3 (14.3%) were educated till college level, and 1 was a graduate. Occupational distribution among males showed 8 (38.1%) as unskilled workers, 10 (47.6%) as semiskilled workers, 2 (9.5%) as businessmen, and 1 as a semiprofessional.
Only 35 (18.7%) were aware of the health hazards associated with consanguineous marriages. This included awareness about physical handicap, mental retardation, and congenital anomalies among offspring stated by 17, 3, and 4 participants, respectively.
However, 57 (30.5%) has a misconception that no hazards were associated while the remaining 95 (50.8%) participants were not sure. Only 1 participant in the consanguineously married group was aware of these hazards before marriage.
Source of information was relatives or friends in 19 (54.3%) participants, newspaper articles and television in 4 each, and from medical personnel in 2 participants. Of the total participants, 23 (12.3%) have history of consanguineous marriages. Marriages between first cousins were the commonest type of consanguineous marriages observed, 15 (65.2%), followed by second-cousins marriages, 6 (26.1%), and the rest 2 were uncle–niece marriages. Reasons for preferring consanguineous marriages were stated by 20 participants. Twelve (60%) stated previous acquaintance while 7 (35%) stated pressure from family members and 1 participant said that it was a traditional practice in their family.
History of consanguineous marriage was seen significantly more among illiterates (P = .05) and participants with parental history of consanguinity (P < .001) (Table 1). The mean age at marriage of women in the consanguineous marriage group was found to be 19.8 ± 3.5 years and in the nonconsanguineous marriage group was found to be 21.7 ± 4.3 years (t = 1.948, P = .05).
Congenital anomalies (P = .02) and low birth weight (birth weight <2.5 kg) (P = .05) were seen significantly more among children of parents with history of consanguineous marriages (Table 2).
Association Between History of Consanguineous Marriage and Presence of Obstetric/Neonatal Complications (n = 187).

Various congenital anomalies among children of the participants with history of consanguineous marriages were ocular diseases in 3 cases, craniofacial anomalies in 2 cases, and cardiac disease, renal disease, mental retardation, and epilepsy in 1 case each. The mean number of children among parents with history of consanguineous marriages was 2.6 ± 1.9 compared with 2.2 ± 1.5 among the rest (t = 1.36, P = .175).
Infant mortality was observed in 1 (4.3%) child born out of consanguineous marriage while it was in 3 (1.8%) children born out of nonconsanguineous marriages (χ2 = 0.611, P = .434).
Discussion
Consanguineous marriages are witnessed even in the current era owing to its benefits like greater marital and family stability in a culturally rich heritage settings. This study setting found history of consanguineous marriages among 12.3% of participants. The prevalence of consanguineous marriages in studies done in other parts of the world shows a wide variation from 20.1% to 56.8% due to influence of varied social and cultural factors.7-11 The decreased rate recorded in this study could be attributed to high female literacy, better socioeconomic status, and decrease in parental influences in decisions in marriages in this region. 5
Majority of the consanguineous marriages in this study were between first cousins, which was similar to findings of several other studies.4,5,8,10,11
Awareness of health hazards associated with consanguineous marriages in this study was lower than the observations made by other studies where it ranged from 55.4% to 83.5%.8,9 In another study done in Mumbai, India, 2.1% respondents agreed to consanguineous marriages in spite of being aware of its ill effects before marriage, which was similar to our findings. 12 The above observations support the need for large-scale awareness campaign about the health hazards associated with consanguinity in this region. This can be made effective by interpersonal communication involving health workers and volunteers supported by the fact that friends were the source of information in more than half of the respondents in this study.
No association with religion was observed even though this practice was highest among Muslim population in this study similar to the observations of Nath et al. 4 However, another regional study reported a significant association of consanguineous marriages with Muslim community. 5
An important finding in the present study was that practice of consanguinity was seen significantly more among illiterate people, which was similar to the observations made in several other studies.3,8,13 This aspect was not researched in the previously done regional studies.4,5 This observation further strengthens the role of education, particularly among womenfolk, in making right decisions in life. This will help them to implement their choices without yielding to pressure from other family members. Only the study by Bhole et al 12 reported no association of education with consanguineous marriages. Their finding, however, has limited relevance and social implication as theirs was a hospital-based study and not a community-based one like ours.
No association of occupational status of the participant was noticed with history of consanguinity in this study, which was different from the inverse association noticed in a study done in Yemen. 13
Consanguineous marriages were not associated with economic status of the couple in the study done at Mumbai, India 12 and Lebanon, 11 which was similar to our observations. However, Kuntla et al 3 reported a significant association of low socioeconomic status with consanguinity.
The present study found parental history of consanguineous marriages to be significantly associated with its presence among the respondents similar to observations made in another study done in Iran. 8 Family history of consanguinity also showed significant association in the study done by Bhole et al. 12 This proves the fact that such marriages are associated with social traditions and one successful consanguineous marriage fosters the faith in the system of consanguineous marriages. 12
From the analysis of various sociodemographic variables in relation to consanguineous marriages in this study, it proves that only education and awareness generation can play a role in preventing such practices in the community.
Age at marriage among women being lesser in consanguineous marriages was similar to the observations made in studies done in Mumbai, India, 12 and Yemen. 13 Early age at marriage though has a multifactorial etiology, consanguinity by means of prior acquaintance could have played an influential role here.
The prevalence of consanguinity was higher in rural areas but this was not statistically significant similar to findings of a study done in Yemen. 13 But Sedehi et al 8 found a significant association of consanguineous marriages with rural areas. The higher rates of the consanguineous marriages in the rural areas could be because of the low educational status added to greater cultural influences from parents’ and relatives in favor of consanguinity in comparison with urban areas. 8
Another reason could be that in rural areas the marriage pool is smaller (fewer people to choose from) especially when staying within the same geographical region and community of shared cultural and social values leading to predominance of consanguineous marriages.
The commonest reason for preferring consanguinity in this study was previous acquaintance, which was similar to findings of the study done in Iran. 9 This could have influenced early age at marriage among the participants in this study as discussed earlier. The various reasons stated in studies done in different parts of the world were traditional influence, easy adjustment for the bride, more care by in-laws, more security for the bride, low expectations of partners and families, to strengthen family relations, and easy settlement of marital conflict because of common relatives.9,10 The wide variations in preferences again reveals influence of varying cultural practices in different geographical regions in the world.
Although the proportion of mothers with history of abortion was slightly higher in the consanguineous marriage group in the present study, it was not statistically significant as observed by Nath et al. 4
There were no significant differences in rates of stillbirth between consanguineous and nonconsanguineous marriages observed in other studies,4,9 which was similar to our findings but was in contrast to the findings of other studies where a significant association was noticed.3,14
The association between low birth weight and consanguinity, which was found to be significant in this study, was also supported by another study done in Iran. 15 But a multihospital study done in Jerusalem found no such association probably because of various biases associated with hospital-based studies. 16 Congenital malformations were found significantly more in the present study among consanguineous marriages as also found in several other studies.7,9,15,17-19 This being the first regional study to reveal this observation should prompt researchers to plan more such studies in this region to substantiate these facts. Accordingly interventions like educational awareness programmes should follow so as to minimize congenital anomalies and disabilities in children as a consequence of consanguineous marriages.
Common congenital malformations observed out of consanguineous marriages in various studies in the world were blindness, mental retardation, physical retardation, bilateral cleft lip and cleft palate, cystic fibrosis, cardiac malformations, polycystic kidney, polydactyly, deafness, and epilepsy.4,7,11,13,17,20,21
In unrelated mating, the probability of producing a child with a serious birth defect or mental retardation is 3% to 4%. This figure was found to double in first-cousin mating and treble in uncle–niece and aunt–nephew marriages. 22 Since first-cousin marriages formed the major type of consanguineous relationship in our study setting, this explains the significant proportion of congenital malformations as observed here. In another regional study, no significant association of congenital malformations with history of consanguineous marriages was observed although it was higher in the families with positive history of consanguinity. 4 However, the finding in the former study with respect to no association of neonatal deaths with consanguineous marriage was similar to our findings. 4 A Turkish study, in contrast, found a significant risk of mortality during infancy attributed to deleterious recessive genes and multigene complexes inherited. 14
A review of studies done by Bittles 2 found that the mean number of live births was higher in the consanguineous unions when compared with marriages between nonconsanguineous couples, which was also observed in this study even though it was not a significant observation. The reason for higher fertility among consanguineous couples may be their earlier age at marriage as observed in this study.
Conclusions
Prevalence of consanguineous marriages in this study was found to be 12.3% of which first-cousin marriages were the commonest. Parental history of consanguinity was found to significantly influence consanguineous marriages among children suggesting role of traditional values. This practice was seen less commonly among well-educated participants. The overall awareness regarding problems associated with consanguinity was very low among most participants. Hence there is a need to create public awareness regarding the ill effects of this social problem. The commonest source of information of ill effects of consanguinity was friends. This supports the effectiveness of interpersonal communication for educating people. The adverse consequences of consanguineous marriages observed in this study were early age at marriage among women and congenital anomalies and low birth weight among their children. Premarital counseling for couples with a family history of anomalies to avoid consanguinity and preconception genetic counseling for those with consanguineous marriage to avoid genetic disorders will facilitate informed family planning. Enquiring of history of consanguinity should also be made a routine practice for all antenatal mothers presenting for obstetric examinations.
Strengths of This Study
This was a community-based study done in both urban and rural areas. It analyzed the role of sociodemographic variables comprehensively in association with history of consanguineous marriage.
Limitations
In few of the house surveyed, medical records were not available and outcomes in pregnancy and child birth was recorded as told by the parents and hence could not be verified.
Footnotes
Acknowledgements
The authors would like to thank Dr Maria Nelliyanil, Assistant Professor, Department of Community Medicine, A. J. Institute of Medical Sciences, Mangalore and Dr Suresh Lankeshwar, Professor and Head of Department, Department of Community Medicine, AIMS, Belur, India for their guidance and support throughout the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.