
Abstract
Keywords
Introduction
The hospitalist movement in the United States has risen in prominence over the past 2 decades.1,2 In the United States, hospitalists are physicians who specialize in the delivery of comprehensive medical care to hospitalized patients. This is in contrast to the traditional model of care where many family physicians and general internists cared for their patients in both the hospital and outpatient settings. The ability to follow patients across settings allows for continuity of care, which ideally improves care coordination, transitions of care, and cost-effectiveness. With rising numbers of hospitalists, many primary care physicians (PCPs) are choosing to concentrate their clinical activities in either the inpatient or outpatient setting. PCPs providing care in fewer settings may erode 2 central tenants of primary care, continuity and comprehensiveness. 3 Studies demonstrate comparable quality of care between hospitalists and the patient’s PCP in the provision of hospital-based care, but the effects of hospitalist care on the overall patient experience remain unknown.4,5 For example, a Dutch study showed that patients value contact with their PCP when they are hospitalized. 6 In another study, 87% of patients had a PCP but only 33% of these had contact with their PCP in the hospital. 7 Respondents were satisfied with their contact with their PCP during hospitalization, but about half wished to receive news about medical/surgical treatment options and serious diagnoses from their PCP. Despite this, previous research has demonstrated that patients are not seeing their PCP while hospitalized as regularly as they used to. For example, an analysis of Medicare data found that the proportion of patients seeing a physician in the hospital whom they have seen before as an outpatient declined from 50.5% to 39.8% from 1996 to 2006. 8
While past research has documented increasing numbers of physicians working as hospitalists, or compared the quality of care between PCPs and hospitalists, to our knowledge no study has estimated the proportion of PCPs who use hospitalist services or continue to manage hospitalized patients themselves. Understanding these practice parameters may inform where family physicians face patient continuity or communication issues regarding inpatient care. Better insight into these types of practice arrangements may also suggest ways to improve any perceived deficits. Therefore, the objective of our study was to determine the percentage of family physicians that use hospitalist services, manage their own hospitalized patients, or manage hospitalized patients in conjunction with their partners.
Methods
Data and Sample
We used data from a 2-week long survey conducted by the American Board of Family Medicine (ABFM) in 2011. During the survey, any physician accessing their online physician portfolio was redirected to a brief questionnaire before they could continue, yielding an effective 100% response rate. We linked the survey data to demographic data from the ABFM database, as well as county level data from the 2011 Area Resource File. 9 The physician’s address was geocoded to determine their county of residence. In order to determine associations between scope of practice and practice organization with hospital care, we only included physicians who had demographic information available. The ABFM collects demographic information from its diplomates as part of the application for the Maintenance of Certification for Family Physicians examination, which is usually taken every 7 to 10 years after initial certification.
Variables
For our outcome variable, we used an item from the questionnaire asking “When one of your adult patients is admitted to the hospital for a medical condition, which of the following best describes your typical role in managing the patient in the hospital.” We created 3 variables indicating if the respondent answered yes to “A hospitalist group manages the patient,” “You manage the patient personally,” or “One of your partners manages the patient.”
The ABFM demographic data included age at the time of survey administration, gender, degree type (MD or DO), international medical graduate status, and if they were ABFM certified at the time of the survey. We also included a variable for practice organization, which we operationalized as group/partnership, educator, health maintenance organization, solo practitioner, or other. We included other practice characteristics likely to be associated with a physician providing hospital care: performs obstetrical deliveries, takes care of newborn infants, has admitting privileges to a hospital, and reports doing major surgery.
The availability of hospitalists and the demand for inpatient care are likely to be associated with use of hospitalist services. We created county level variables from the 2011 Area Resource File to test these associations. First, we created variables from data elements in the Area Resource File indicating the percentage of short-term general hospitals with a hospitalist program, and numbers of full-time and part-time hospitalists per short-term general hospital. We theorize these variables will represent availability of hospitalist services and would be associated with higher use of hospitalist services. Second, we created a variable indicating the number of general short-term hospital days per 10 000 county residents (in thousands of days) to account for the demand of physicians providing hospital care. We used only short-term general hospitals as these are the hospitals where community physicians are most likely to hold admitting privileges as opposed to long term care, federal, specialty, or psychiatric hospitals. We did not include children’s hospitals as the main outcome variable specifically asked about adult patients. We modeled rural/urban differences with the Rural Urban Continuum Codes and classified counties as metropolitan, nonmetropolitan, and completely rural. 10
Statistical Analysis
Descriptive statistics were used to characterize the survey and demographic data. We stratified the analysis by the respondents’ method of managing hospitalized patients to determine associations between the method and physician and county characteristics. Next, we determined the distribution of physician characteristics by each method. Then, we performed 3 multilevel logistic regressions to study the adjusted associations between the different methods of managing inpatients and physician and county characteristics. Multilevel modeling accounts for nesting of physicians within counties, which violates the assumption of independence in ordinary least squares regression. We performed separate regressions for each of the management methods (hospitalist group manages the patient, you manage the patient, and one of your partners manages the patient). All demographic and county-level variables were included in each regression model. For the analysis, age was broken into those 52 years and younger and those older than 52 years based on the mean. Newly graduated physicians were excluded from analysis since demographic data were not available and only 4.4% of the sample were younger than 40 years. Because of the skewed distribution, the percentage of hospitals with hospitalists per county was divided into 4 groups for analysis: 0%, between 0% and 50%, between 50% and 100%, and 100%, using 0% as the reference group. We used “other” as the reference group for group practice type and metropolitan as the reference group for rurality. SAS version 9.3 (Cary, NC) was used for all analyses. This study was approved as exempt research by the American Academy of Family Physicians Institutional Review Board.
Results
Of the 5818 physicians who completed the survey, we excluded those not residing in the United States and those without demographic information, leaving a final sample of 3857 (66%). Compared with other family physicians in the ABFM database who have taken the Maintenance of Certification for Family Physicians Examination (n = 55 457), physicians in our sample were slightly older (40.9% vs 37.9% ≥55 years, P < .01), more likely to be female (35.3% vs 31.1%, P < .01), and more likely to be part of a group/partnership practice (71.7% vs 69.5%, P < .01) than those not in the sample (data not shown).
Overall, respondents in our sample had a mean age of 52.0 years (standard deviation = 7.8) and were more likely to be male (64.7%), practice in a metropolitan county (80.8%), and take care of newborn infants (62.4%). A large majority (74.2%) reported having admitting privileges to a hospital (Table 1). The average percentage of short-term general hospitals with hospitalist programs in counties where respondents lived was 54.8%. In 26.6% of counties, all short-term general hospitals had a hospitalist program. The mean (standard deviation) number of full-time and part-time hospitalists per short-term general hospital was 4.5 (6.1) and 1.6 (2.5) respectively.
Physician- and County-Level Characteristics of the Sample.

In terms of management strategies for inpatient care, the majority of respondents use a hospitalist group (54.0%), with 18.2% managing their patients personally and 8.2% having one of their partners manage the patient (Table 2). In all, 14.4% answered not applicable and 5.3% answered other.
Management Strategy of Family Physicians When Their Patients Require Inpatient Care.

In descriptive analysis, we found differences between physician characteristics and each management strategy (Table 3). Not surprisingly, practice organization varied considerably between the management strategies. Respondents who managed their own patients were represented more heavily in solo practice than groups or other arrangements (26.3% vs 58.7% vs 9.9%) respectively, and those who used hospitalists were more likely to be in groups than solo practice or other arrangements (63.9% vs 14.8% vs 15.9%) respectively. As expected, respondents who performed obstetrical deliveries, provided inpatient care or had admitting privileges to the hospital were more likely to either take care of the patient themselves or have a partner manage the patient. Use of hospitalist services decreased from 84.9% in metropolitan counties to 1.0% in completely rural counties.
Physician- and County-Level Characteristics by Role in Managing Patients in the Hospital.

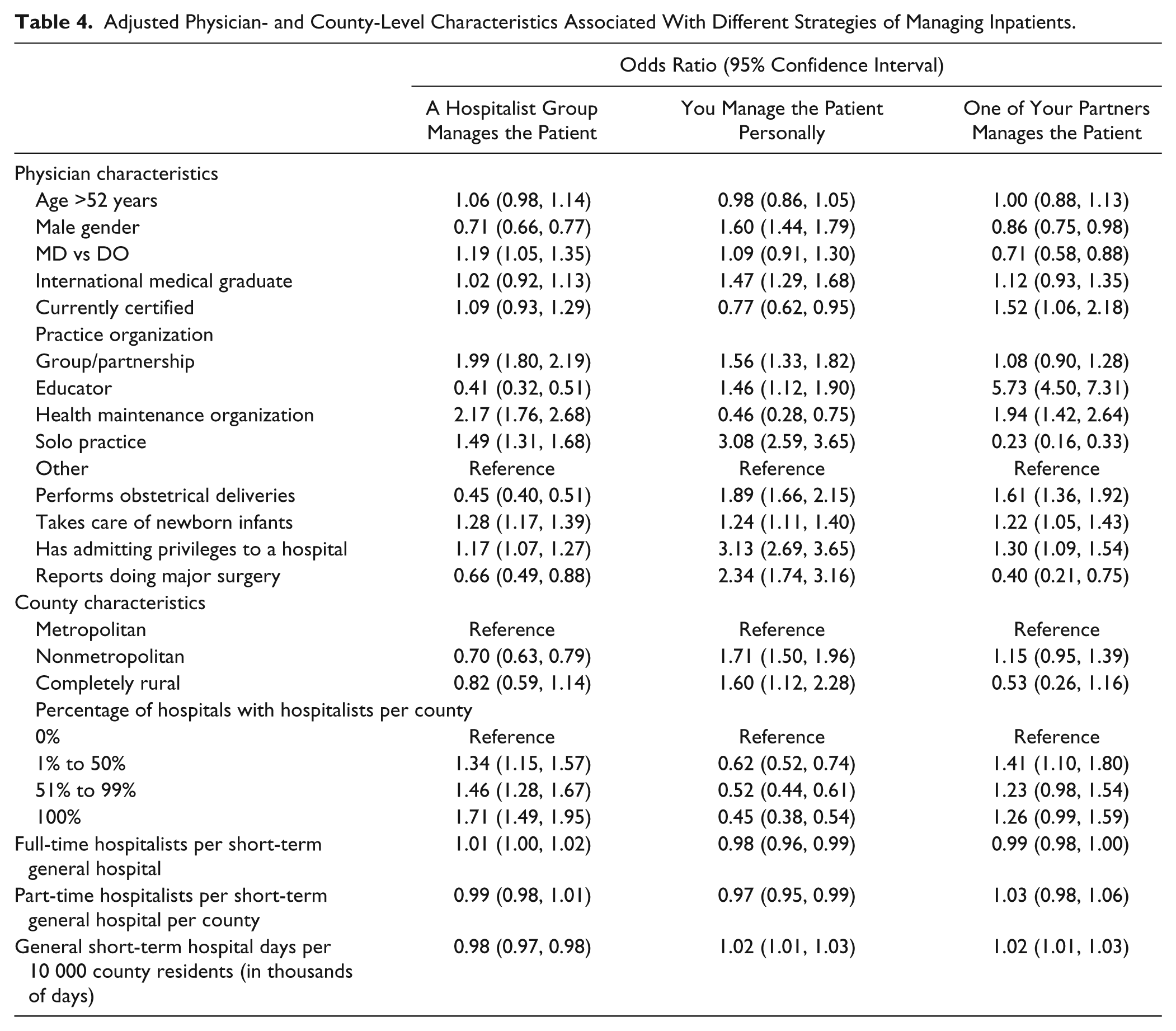
In multilevel logistic regression, practice organization remained strongly associated with different management strategies. For example, educators are far less likely to use hospitalists (odds ratio [OR] = 0.41; 95% confidence interval [CI] = 0.32-0.51) and much more likely to have a partner manage their patients (OR = 5.73; 95% CI = 4.50-7.31; Table 4). Respondents in solo practice were both more likely to use hospitalists (OR = 1.49; 95% CI = 1.31-1.68) and manage the patient personally (OR = 3.08; 95% CI = 2.59-3.65). Having admitting privileges to a hospital was positively associated with every strategy. Performing obstetrical deliveries was positively associated with both managing the patient personally and having a partner managing the patient and negatively associated with using a hospitalist group (OR = 0.45; 95% CI = 0.40-0.51). Respondents in nonmetropolitan counties were less likely to use a hospitalist group (OR = 0.70; 95% CI = 0.63-0.79) and more likely to manage the patient themselves (OR = 1.71; 95% CI = 1.50-1.96) compared with urban physicians. Increasing percentages of short-term hospitals with hospitalists was associated in a dose–response relationship with both increasing likelihood of using hospitalist services (OR = 1.34 to OR = 1.71) and decreasing likelihood of managing the patient personally (OR = 0.62 to OR = 0.45). Fit statistics for the regression models indicated good explanatory power with χ2/degrees of freedom ratios ranging from 0.85 to 0.93.
Adjusted Physician- and County-Level Characteristics Associated With Different Strategies of Managing Inpatients.
Discussion
Our main finding that more than half of family physicians in this sample use hospitalists is consistent with research showing increasing hospitalist utilization.1,2 The finding that urban physicians use hospitalists more is not surprising given the availability of medical specialists and tertiary services in such settings. Rural physicians and those who provide a wider range of services like deliveries and major surgeries that occur in the inpatient setting may be more likely to see their own hospitalized patients than those who do not provide such services. Educators and academic physicians may focus on particular areas of practice, so it is not surprising that some have partners managing their hospitalized patients.
Some suggest that the hospitalist movement may improve length of stay and decrease hospital costs modestly compared with management by a PCP without affecting readmission or death rates. 4 Others argue that care by hospitalists may in fact cost more and have longer lengths of stay than management by a PCP.11,12 A tremendous diversity of practice arrangements exists between hospitalist groups and this can make analyses of key quality parameters less generalizable. 13
Our results have implications for the physician workforce and health care access. Firstly, our results suggest that increasing availability of hospitalist services is associated with PCPs providing a narrower scope of practice. This suggests that family physicians may be concentrating their services in the ambulatory setting or moving to new career opportunities as hospitalists. With expected increases in patient demand for health care because of aging of the population and insurance expansion, such division of the workforce may worsen projected shortages of PCPs. Second, previous work has shown an association between robust primary care and lower health care costs and better population health; 3 if family physicians are not providing care in multiple settings these benefits may not be realized.
We found important associations between other elements of practice and whether a family physician provides inpatient care. Physicians who also provide care that generally requires the patient be in the hospital, obstetrical deliveries and major surgery for example, are more likely to manage their own patients. These physicians may be more likely to practice the traditional, wide scope of practice model of family medicine rather than concentrate on a specific care delivery setting. Physicians with academic appointments were less likely to use hospitalists and more likely to have their partner manage hospitalized patients. This likely reflects the traditional academic roles of teaching across multiple settings and role modeling a fuller scope of practice. Finally, rural location was strongly associated with personally managing hospitalized patients. This finding is not surprising as hospitalist services were much less frequent in rural counties.
Our study is subject to multiple limitations. First, our data were cross sectional, and we cannot make any assertions about causality between performance of other services and providing inpatient care. Nor can we draw conclusions about whether the use of hospitalist services was caused by increasing numbers of hospitalists or if demand for hospitalist care lead to high numbers of hospitalists. Second, our data were collected from a sample of family physicians who may not be representative of family physicians as a whole. However, few differences were discernable between the characteristics of our sample and other family physicians with demographic information available. Additionally, certification is a voluntary process and our findings may not be representative of those few physicians who choose not to certify.
With rising numbers of hospitalists, it is not surprising that most family physicians are now using their services instead of providing inpatient care themselves. Some may argue that the quality of both inpatient and outpatient care may improve as physicians focus their efforts in their respective settings. However, the potential effects of loss of continuity for the patient and comprehensiveness for the provider remain unknown.
Footnotes
Authors’ Note
Results of this study were presented as a poster at the AAMC Workforce Conference in Alexandria, Virginia in May 2013.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.