
Abstract
Introduction
Decades of conflict in Somalia have produced one of the largest refugee populations in the world. 1 Somali refugees to the United States have been susceptible to limited health care access, 2 low health literacy, 3 and limited English proficiency. Furthermore, beliefs about health and disease may place the role of health care only in the realm of treatment. 4 As a result, Somali patients are less likely to participate in preventive health services than the general population, 5 and chronic disease management is suboptimal. 6
Barriers to effective navigation of US health care systems may be especially significant for Somali women. 7 Even among Somali women with adequate health insurance, health care access may be compromised, reflecting a feeling of isolation and the lack of skills to effectively access more complex health care systems. 4 Somali women have expressed frustration regarding the care they experience related to a perceived lack of understanding of their cultural beliefs by health care providers.3,4
Patient–provider gender discordance has been described as a barrier to health-seeking behaviors and effective communication by Somali women in qualitative work as it relates to reproductive health care, 8 pregnancy and birth, 9 performance of cervical cancer screening, 3 and discussion of gynecological concerns. 10 This body of work suggests that the most problematic feature of gender discordance involves the physical examination (touch/physical contact). Among non-Somali women, patient–provider gender concordance is associated with important clinical outcomes, including provision of gender-specific preventive health measures.11-13 Previous work has also shown that Somali women in a primary care setting are more likely to undergo cervical cancer screening when seeing a female physician, despite more frequent visits to male physicians. 14
The major interface between Somali women and the health care system is in primary care, yet perceived barriers to patient–provider gender discordance among Somali women in a primary care setting have not been previously explored. Furthermore, past work among patients with limited English proficiency demonstrated that patient–interpreter gender concordance may mitigate discomfort with patient–provider gender discordance. 15 Interpreter preferences have not previously been elucidated among Somali patients. Finally, minority populations in general describe strong preferences for patient–provider racial concordance, but these preferences have not been explored among Somali patients. 16 Since these perceptions may be linked to clinical outcomes, it is important to understand them so that primary care systems may more effectively address health disparities among Somali women. Therefore, we conducted a survey of Somali women who are empanelled to a large primary care practice in order to understand their comfort with different components of the physical examinaiton by providers and interpreters of different genders and races.
Methods
Study Setting and Study Sample
This study was conducted in the Primary Care Internal Medicine clinics at an academic ambulatory practice that provides primary care to approximately 70 000 adult patients in a medium-sized city in the Midwest United States. Adult women who were empanelled to this practice and met the following inclusion criteria were sequentially enrolled in the study: (a) self-reported to be born in Somalia and (b) self-identified need for a Somali-speaking medical interpreter. Consent, enrollment, and survey administration took place during a single visit to their health care provider. Study procedures were approved by the institutional review board.
Survey Design and Implementation
A survey instrument was created through an iterative process involving the institutional Media Services Department, study investigators, and Somali women who were representative of the study population but who did not participate in the study. A pictorial survey design was chosen to elucidate preferences of Somali women for providers of different genders and race. Photographs of a replicate clinical encounter were taken of a physician sitting in an examination room with a female Somali patient and a female Somali medical interpreter. Each photo included the same patient and interpreter, but a different physician. The physician in each of the 5 photos differed by race or gender, but not generation (approximate age): black male, white male, black female, white female, Asian female. To avoid carryover effects, the ordering of the 5 picture scenarios in each survey was randomized based on a Latin square design.
Study participant comfort level with different parts of the body being examined by the pictured physician was measured on a 3-point Likert-type scale of acceptability (“no problem,” “sometimes a problem,” “definitely a problem”). As a confirmatory measure of provider preference, participants ranked each of the 5 providers according to their preferences for performing the physical examination. To elucidate the role of patient–interpreter gender concordance, the same Likert-type scale was used to assess acceptability with various portions of the physical examination in the presence of a male versus female Somali medical interpreter.
The survey was pilot tested with two patients and refined prior to study implementation. The survey was conducted in the Somali language by one of the Somali-speaking authors (MFHS) or a Somali-speaking study coordinator.
Data Analysis
Descriptive statistics were used to summarize comfort ratings. Paired ratings of discomfort (between 2 providers of the same gender but different race, or vice versa) were measured for agreement using the weighted kappa statistic, and assessed for statistical differences using Bowker’s test of symmetry. For each type of provider (eg, black male), an aggregate score was calculated by summing each of the 3-point Likert-type scales across all 6 components (score range = 0-12). Simple linear regression was used to test the association between this aggregate measure of discomfort and demographic characteristics (age, years lived in the United States, education level, employment status, marital status). A P value <.05 was considered statistically significant. All analyses were performed using the statistical software package SAS, version 9.2 (SAS Institute, Cary, NC).
Results
Fifty Somali-speaking female patients were enrolled in the study from April to May 2012. The baseline characteristics are presented in Table 1. Participants were primarily Muslim women who immigrated to the United States, generally for refugee resettlement. All patients had access to medical care and were empanelled to a primary care practice.
Demographics of the Study Population.
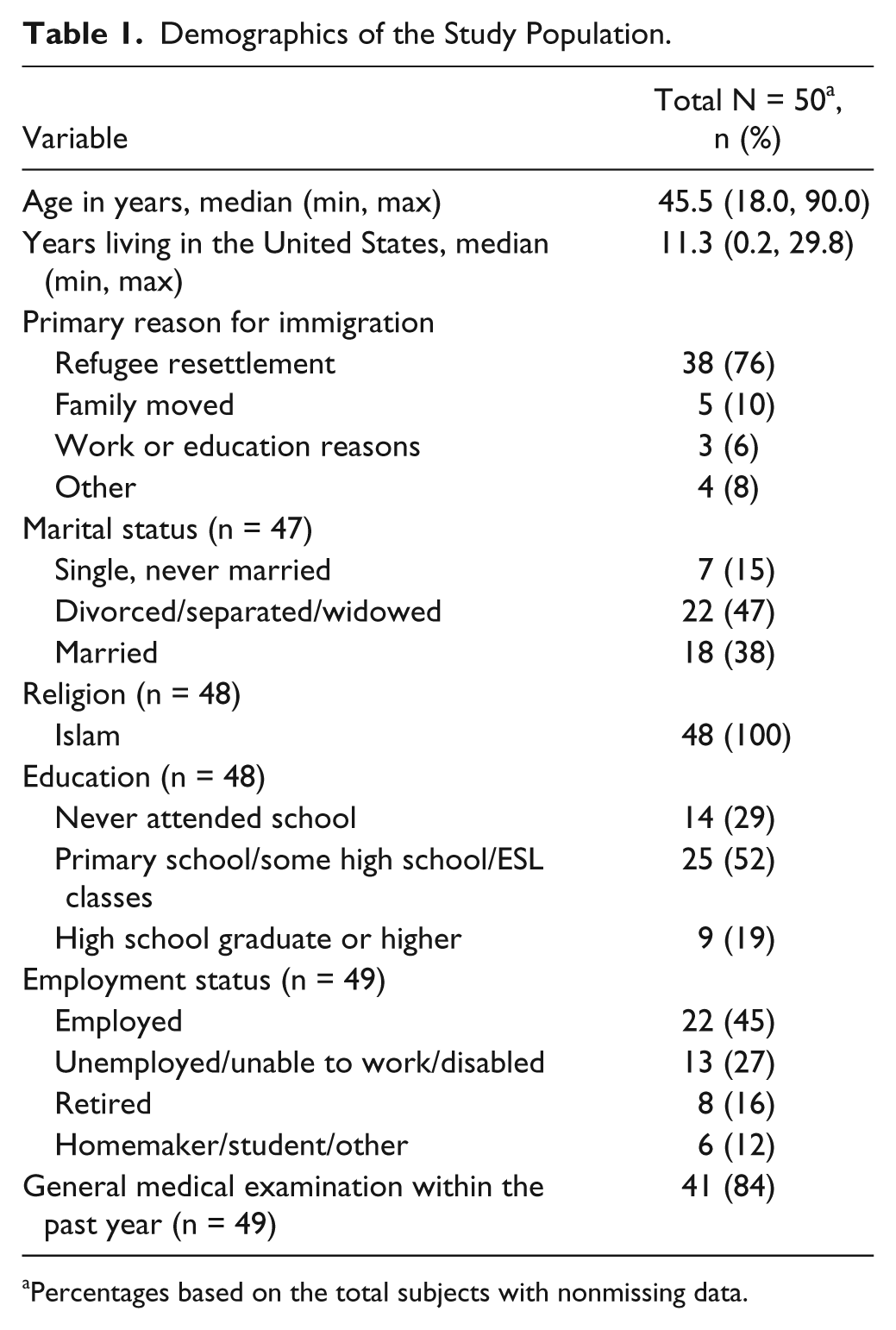
Percentages based on the total subjects with nonmissing data.
Most participants (49 of 50) reported “no problem” to each component of the physical examination performed by a female provider. In contrast, the majority of women reported that performance of the genitalia/pelvic examination (82%), breast examination (81%), and abdominal examination (71%) by male providers was “definitely a problem.” A minority of women reported that performance of the chest/back examination (29%), extremity examination (28%), and head/neck examination (25%) by male providers was “definitely a problem” (Figure 1). Univariable analysis showed that discomfort with a male provider was marginally to significantly elevated in participants who were older (P = .058), unemployed (P = .058), and formerly married (P = .046), and was not associated with education level (P = .306) or duration of residence in the United States (P = .184).

Perceived comfort with components of the physical examination among 50 Somali women by provider race and gender.
For each portion of the examination, the reported levels of discomfort with a black versus white male provider were highly concordant (kappa statistic for agreement, range = .76-.96) and not significantly different (P value range = .26-1.0). When asked to rank each of the 5 providers according to preference for conducting the physical examination, the majority of participants (78%) ranked all 3 female providers (white, black, Asian) higher than the 2 male providers (white, black).
All participants reported “no problem” with the presence of a female Somali interpreter for each portion of the physical examination. In contrast, the majority of women reported that the presence of a male Somali interpreter for the genitalia/pelvic examination (71%), breast examination (67%), and abdominal examination (64%) was “definitely a problem.” A minority of women reported that the presence of a male Somali interpreter for the chest/back examination (23%), extremity examination (22%), and head/neck examination (22%) was “definitely a problem” (Figure 2). Each portion of the examination reflected responses of significantly higher discomfort with the presence of a male Somali interpreter compared with a female (P < .01 for each).

Perceived comfort with components of the physical examination among 50 Somali women by interpreter gender.
Discussion
In this survey study, we found that Somali women generally prefer a female provider for conducting the physical examination. This confirms conclusions from past qualitative work,3,8-10 while extending this finding to a primary care setting and by demonstrating that discomfort with the physical examination is most significant for sensitive components, namely the pelvic, breast, and abdominal examinations. This study further adds to the literature by showing no preference for patient–provider racial concordance among Somali women and that these patients strongly prefer Somali female interpreters to their male counterparts to be present for the physical examination.
These results suggest that patient discomfort with patient–provider gender discordance may contribute to the known disparities in adherence with preventive health screening among Somali women, particularly for sensitive procedures (eg, breast and cervical cancer screening). This may magnify the well-documented positive effect of patient–provider gender concordance on the provision of gender-specific preventive health measures among women in general.11-13 These collective findings imply that Somali women should be provided with the opportunity to request a female provider for sensitive portions of the physical examination and preventive services.
While Somali women clearly identified a preference for female providers during sensitive portions of the physical examination, this discomfort was less pronounced for the remainder of the examination. Therefore, a takeaway from this study should not be that Somali women should only see female providers. Our study measured preferences in relation to hypothetical scenarios with providers they did not know personally. Past work suggests that a longitudinal caring relationship with a primary care provider is an important facilitator of effective health care among Somali women, regardless of provider gender. 10 Further work is needed to explore the relative impact of these and other factors on health-seeking behaviors and health disparities among Somali women in primary care settings.
Reasons for gender concordant preferences among Somali women were not explored in this study, but past work suggests that religious and cultural norms may dictate this practice and preference. 10 Interpretation of Islamic tenets may influence these preferences, though these tenets do not preclude examination by a physician of the opposite gender. 17 Furthermore, these preferences are likely heterogeneous among Somali women. Since large-scale Somali emigration is relatively recent (mid-1990s) and continues today, generational heterogeneity in culture and practice will become more pronounced over time. Practitioners should be aware of these potential differences, and avoid interventions that lump all Somali women in the same category. As a second generation of Somali immigrants age into adulthood, future work should explore intergenerational differences in perceptions of provider demographics among Somali women, and their impact on health care utilization.
We found no preferences among participants for patient–provider racial concordance, which is in contrast to findings among minority populations in general. 16 This contrast may highlight the difference between racial and ethnic concordance. The black physicians pictured in our survey were not Somali, thereby imposing the same linguistic and cultural discordance as white physicians. This concept of “social concordance” has been shown to be an important mediator of patient satisfaction. 18 In one focus group study, Somali women agreed that more Somali health care providers are needed in the United States to help address this discordance. 10
Participants reported significant discomfort with patient-interpreter gender discordance, which may magnify discomfort with patient–provider gender discordance. 15 This has implications for health care organizations who use in-person interpreting services for Somali patients. These organizations should strive to achieve patient–interpreter gender concordance for clinical encounters that are most likely to involve a physical examination of sensitive areas (eg, obstetrics, gynecology, primary care). These interventions should be tested to assess resultant health-seeking behaviors among Somali women (eg, missed appointments, completion of preventive services, etc).
This study has limitations. Participants were from a single community, with implications for generalizability. Though this was not the intent of the study, the lack of a control group precludes comparison with non-Somali women. Finally, this study was not designed to explore the link between discomfort with patient–provider gender discordance and health-seeking behaviors. Future work should determine whether these concerns are substantial enough to alter Somali women’s interaction with the health care system in a way that meaningfully contributes to suboptimal outcomes and health disparities.
Conclusions
In conclusion, we found that Somali women generally preferred a female provider for conducting the physical examination, particularly for the pelvic, breast, and abdominal examinations. Likewise, Somali women strongly preferred female interpreters to be present during the physical examination. There was no stated preference for patient–provider racial concordance. These findings have implications for structural health care changes aimed at delivering culturally sensitive and effective primary care to Somali patients.
Footnotes
Acknowledgements
The authors wish to thank Jane Hughes, Katie Grobe, Debra Melton, and Shannon Blegen from the Mayo Clinic Language Department for their assistance in recruitment of study participants. They would also like to thank Nasra Giama for her review of the survey instrument, Matthew Schneider for help with survey graphic design, and Fatuma Omer for her work conducting interviews.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by the Mayo Clinic Department of Medicine 2012 Edward C. Rosenow Endowed Professorship Residency Research Award.