
Abstract
Introduction
Multiple chronic conditions (ie, concurrent chronic medical conditions or multimorbidity) and their related health care costs have been studied in older adults,1-3 but such studies are relatively limited in children.4,5 Recent studies have shown that the number of children with chronic health conditions has increased dramatically in the past few decades. 6 Many factors may contribute to this increased prevalence of childhood morbidity. In addition to the improved medical treatment for pediatric conditions, particularly the increases in survival of very low birth weight, premature infants and infants with life-threatening congenital disease and defects; other factors, such as dietary changes, air pollution, sedentary behaviors, and changes in socioeconomic status also contribute to the increasing prevalence of chronic conditions in childhood. 6 Improvement in morbidity diagnosis, such as greater recognition of behavioral disorders such as attention deficit hyperactivity disorder, may also affect the increased prevalence of comorbid conditions in childhood. Along with the increased prevalence of disease, there has also been an increase in childhood medical complexity. Data from the Nationwide Inpatient Sample showed that hospitalization rates of children with more than one complex chronic condition have doubled over the past 15 years. 7 The increasing prevalence of multiple chronic conditions will contribute to increased health care utilization and increasing costs.8,9 However, most of these studies are based on cross-sectional data. In this study, we describe the prevalence and persistence of high health care expenditures of multiple chronic conditions in a pediatric population with continuous health benefit coverage from 2004 to 2007.
Methods
Study Sample
All dependents of Mayo Clinic employees in Rochester, Minnesota, aged 0 to 17 years on January 1, 2004, with continuous health benefit coverage through December 31, 2007 were included (n = 14 727). This represents 70.6% of those with coverage in the initial year (n = 20 873). Health benefit coverage was determined from benefit enrollment records for the 4-year time frame. To avoid potential bias, enrollees who died during the timeframe (n = 6) were included.
Measures
Data on chronic conditions, health care utilization, and expenditures were obtained from medical and pharmacy claims, including mental health services. We have provided a description of our approach for defining 56 chronic conditions, definitions of Hwang et al, 10 in an article on working-age adults. 11 In short, chronic conditions were defined as conditions that had lasted or were expected to last 12 or more months and resulted in functional limitations and/or the need for ongoing medical care. Hwang et al 10 used a panel of 10 physicians (5 pediatricians and 5 internists) to classify diagnoses as chronic or not. These diagnoses were then summarized into groups using Agency for Healthcare Research and Quality (AHRQ) Clinical Classifications Software for International Classification of Diseases, Ninth Revision (ICD-9), Clinical Modification (http://www.hcup-us.ahrq.gov/toolssoftware/ccs/ccs.jsp). In our study, medical conditions were assessed from health care claims for all hospital and outpatient services from January 1, 2004 through December 31, 2007. ICD-9 diagnosis codes with a chronic indicator according to the AHRQ Clinical Classification System not grouped into the Hwang subgroups were assessed for classification individually by a panel composed of the study team (JMN and DMF).
Expenditures were estimated by adding the total payments made by any insurance plus any patient deductibles, coinsurance, and copayments. Expenditures were calculated as annual payments over the 2004-2007 timeframe. The consumer price index (http://www.gpoaccess.gov/eop/2007/b60.oxs) was used to adjust expenditures over time and expenditures reflect 2007 US dollars.
Analysis
The prevalence of each of the chronic conditions over the 4-year time frame was estimated by dividing the number of children affected by the total number of children and multiplying by 100. The total expenditure for a particular chronic condition was calculated as the sum of all payments for all services for patients with that condition. For example, the expenditures for a patient with both asthma and depression were included under each condition. However, when we examined the combined expenditures among patients with multiple conditions, the payments for a single patient were only counted once. Expenditures were examined overall, within age-groups, in expense categories and by number and type of condition. Age-groups were defined based on the child’s age in 2004. The persistence of staying in the top 10th percentile of expenditures was also analyzed with a transition matrix to examine year-to-year persistence over the 4 years.
Results
Prevalence of and Expenditures for Chronic Conditions
Overall, 5964 (40.5%) of the children had at least 1 chronic condition. The 20 most prevalent conditions in this population are shown in Table 1. The most prevalent chronic condition was asthma/chronic obstructive pulmonary disease (COPD), which had a relatively stable prevalence across all age-groups. Girls had a lower prevalence of asthma/COPD at younger ages but had a similar prevalence to boys when older. Some chronic conditions, such as behavior problems, anxiety, and depression increased sharply with age. For example, the prevalence of behavior problems was 4.2% in the group of 0- to 4-year-olds, and then jumped to 10.3% in the group of 5- to 12-year-olds. Boys had a higher prevalence of behavior problems than girls, while older girls had a higher prevalence of depression and anxiety problems than boys. Boys and girls had a similar prevalence of obesity.
Overall, sex-, and age-specific prevalence (per 100 children) of the 20 most common conditions in the population.

We calculated the total expenditures for each chronic condition and found that the most costly conditions in the population differed slightly from the most prevalent conditions in the population (Table 2). For example, congenital anomalies affected only 5.7% of the population, while asthma affected 12.0% of the population. However, the overall payment for treating children with congenital anomalies was $9602 per person per year, compared with $4334 for treating those with asthma. Therefore, congenital anomalies were the most costly chronic disease category in this population (Table 2).
Age-specific and mean annual total costs ($) for the 20 most costly conditions in the population.

Prevalence of and Expenditures for Multiple Chronic Conditions
Multiple conditions were prevalent in this population, as 2509 (17%) of the children had 2 or more chronic conditions. The annual health care payments per child increased substantially with an increasing number of chronic conditions (Table 3). For example, the expenditures for children with 5 conditions were nearly 12 times higher than expenditures for children with one condition. Only 1% of children had 5 or more chronic conditions; however, approximately 13% of the total overall payments were accounted for by this group. Inpatient payments increased with the number of chronic conditions, and accounted for more than 50% of the expenditures in children with 5 or more conditions, while outpatient and pharmacy expenditures accounted for more than 50% of the payments in children with 1 chronic condition (Figure 1).
Total number and percent of children with multiple chronic conditions, and the mean annual costs per child ($) attributable to children with multiple chronic conditions.
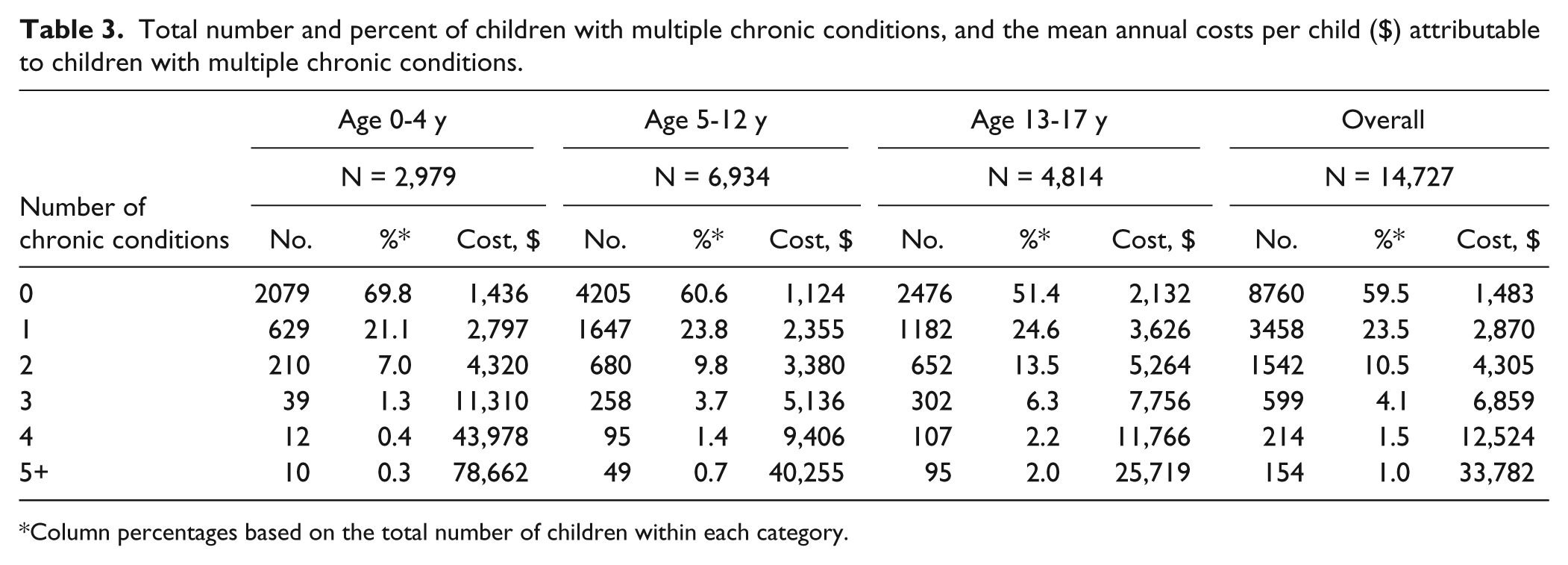
Column percentages based on the total number of children within each category.

Distribution of costs by service among children with 0, 1, 2, 3, 4, or 5+ chronic conditions.
Persistence of Expenditures Over Time
We examined the probability that children who were in the top 10th percentile of expenditures in the first year would remain in the top 10th percentile 1, 2, and 3 years later. Among those in the top 10th percentile of expenditures at baseline, a small proportion of them (0.9%) had no chronic conditions, and these children had a 12% probability of remaining in the top cost category in the following year. In contrast, children with 5 or more chronic conditions comprised a higher proportion of all children in the top 10th percentile (9.1%), and these children had a greater than 75% chance of remaining in the top 10th cost percentile in the following year (Figure 2).

Transition probability for remaining in the highest cost category (top 10th percentile) among children with 0, 1, 2, 3, 4, or 5+ chronic conditions at 1, 2, and 3 years after baseline.
Discussion
In this study, we found that asthma/COPD, allergic rhinitis, and behavior problems were the most prevalent conditions in this pediatric population. However, congenital anomalies, asthma, and behavior problems were the most costly conditions in this group. Additionally, we found that 2 out of 5 children in this population had at least 1 chronic condition, and 42% of these children had multiple (≥2) chronic conditions. The overall expenditures increased substantially with the increasing number of conditions. The proportion of inpatient payments also increased with the number of chronic conditions. These results are consistent with previous studies, as both Simon et al 12 and Burns et al 7 saw increased hospitalization rates among children with multiple chronic conditions. In addition, children with multiple chronic conditions were more likely to persist in the top 10th percentile of expenditures in year-to-year spending.
Using the definition of Hwang et al, 10 the study of Medical Expenditure Panel Survey (MEPS) 2005 reported a much lower prevalence of chronic conditions among children aged 0 to 19 years than our study (21.4% vs 40.5%). 13 Compared with MEPS, our study had a longer time frame (4 years vs 1 year), and we included a few conditions that were not classified by the definition of Hwang et al. Furthermore, it is possible that more diagnoses are captured by the predominately local providers than the national sample. MEPS captures up to 4 diagnosis codes for each office or hospital visit. Our source allowed for up to 15 diagnosis codes for inpatient stays. Our study findings, however, were similar to results from the 2007 National Survey of Children’s Health (NSCH), which estimated that 43% of US children (aged 0-17 years) had at least 1 chronic condition, and among them, 45% had multiple (≥2) chronic conditions. 14 The NSCH study measured chronic health conditions from 20 prespecified conditions, which was not as comprehensive as our study. Barnett et al 15 found a very low prevalence of multimorbidities (<2% among children in Scotland) compared with our overall rate of 42%. The differences between our studies can be attributed to differences in the specific conditions studied. Barnett et al 15 chose to examine 40 morbidities that are highly prevalent in aging populations (heart failure, stroke, diabetes, hypertension, etc) but may not be good measures of chronic disease in children. In our study, we examined conditions that are likely to be long lasting, are prevalent in children, but may not cause the same degree of morbidity as chronic diseases in adults (eg, allergic rhinitis). Therefore, we included conditions that may not cause severe functional limitations but can contribute significantly to increased health care utilization and expenditures. In the future, consensus about the conceptual and operational definitions of chronic health conditions in childhood is needed for better comparison between studies.
Chronic condition patterns were different in children than in adults. In our study, the top three chronic conditions were asthma, allergic rhinitis, and behavior problems among children, while hyperlipidemia, hypertension, and depression have been noted as the top chronic conditions in adults. 11 Furthermore, as expected, some chronic conditions, such as behavior problems, anxiety, and depression increased sharply with the age of the child. Exposure to more structured social interactions (eg, school classrooms) may lead to more problems or may just lead to a higher level of diagnoses. The prevalence of asthma in our study (12.0%) was similar to the prevalence of national publicly insured children in 2009 (12.4%) 14 and was higher than the estimated prevalence for Minnesota during 2001-2005 (4.4% to 7.8%) by the National Health Interview Survey (http://www.cdc.gov/nchs/data/ad/ad381.pdf).
However, the patterns of spending in this population were very similar to those seen in adults, as a large proportion of expenditures were consumed by a small portion of individuals with multiple chronic conditions. These results are similar to previous studies. A study of enrollees in the Medicaid and the Children’s Health Insurance Program (CHIP) reported that 10% of pediatric enrollees accounted for 72% of the total spending. 8 The NSCH reported that the top 10% of children accounted for 54% of all costs. 14 Similarly, in our study, 6.5% of the children (those with 3 to 5 chronic conditions) accounted for 29% of the total expenditures. Additionally, we found that the expenditures increased sharply with the number of chronic conditions among children, as the expenditures for children with 5+ conditions was 23 times higher than for children without any chronic conditions.
Finally, we found that children with multiple chronic conditions who were in the top 10th percentile of expenditures had a significant probability of remaining in the top 10th percentile of spenders 3 years later. Few studies have examined the persistence of health care costs in children. Liptak et al 9 analyzed data from MEPS 2001-2002, and reported that 49% of the children in the top decile in 2001 persisted in the top decile in 2002. Having health insurance, having special health care needs, or functional limitations were risk factors predicting the persistence. Our study further suggested that children with multiple chronic conditions were more likely to persist in the top spenders over a longer time frame. This high cost persistence pattern found among children is similar to patterns in working-age adults, 11 the elderly, 3 and the poor (Medicaid enrollees). 16 Others have suggested that a patient-centered approach rather than a condition-centered approach is needed to contain the growing health care costs for patients with multiple comorbidities. 17
The strengths of this study include a large sample size, the longitudinal data, and the complete records of medical claims. Because of the relatively rich health care benefits at Mayo Clinic, few pediatric dependents would decline benefits, and most enrollees continued to be covered for the study period. In addition, health care for the enrollees was provided predominantly by an integrated provider group with shared medical records and a common database. Therefore, the medical claims include complete information on health conditions and related costs.
One limitation of our study is its reliance on the ICD-9 diagnostic coding system. Some congenital and developmental conditions and syndromes, although affecting multiple organs and body systems are captured by a single diagnosis code. It was not possible to determine whether these conditions were transitory or long lasting. In addition, some conditions classified as “chronic,” may have been used on medical claims when they were actually episodic, present for less than a year, or even “rule out” conditions. For this reason, some of the prevalence estimates may be overestimates of the true population prevalence. Other diagnosis codes, like obesity, are notoriously underutilized. In a previous study among adults where we linked body mass index as recorded in the medical record with diagnosis codes, we found that only 45.1% of people with body mass index >40 kg/m2 (morbidly obese) and 19.4% of people with body mass index from 35 to 39.9 kg/m2 (obese) had a diagnosis of obesity on their problem list (Mr J. Moriarty, Mayo Clinic, Health Care Policy and Research, personal communication).
Second, generalizability of the study results may be limited since the study population was limited to children of employees at a single health care system in the Midwest, and all the study participants had continuous health insurance coverage during the study time period. This employer-based health insurance may have led to higher retention among children with multiple chronic conditions. Furthermore, insurance benefits tend to encourage use of health care. This potentially higher continuity of care may lead to a higher likelihood of diagnosing chronic diseases.
Our study population did not include uninsured and other disadvantaged populations, and results may not be generalizable to such populations. For example, uninsured or disadvantaged children with asthma may be less likely to have access to continuity primary care and receive routine maintenance care and have more acute exacerbations that require higher cost emergency visits or hospitalizations. If this is the case, our results would underestimate costs for children with chronic disease in an uninsured or other disadvantaged population. However, we do not believe that characteristics of the health care system would bias the concentration or persistence over time of higher expenditures among individuals with more chronic conditions.
Families of children with chronic disease have a complex set of challenges that include health care expenses, time obligations for appointments, disease management and coordination, managing the disease itself, and the psychological strain on parents and family members with a sick child.18,19 For this reason, management of children with chronic conditions may need to take into account family resources and dynamics as well as the number and type of chronic conditions.20-22 Our data indicate that a significant proportion of the expenditures in children with multiple chronic conditions are because of inpatient hospitalization payments, and it will be important for future studies to focus on the hospitalization experience for these children to understand whether hospitalization use might be minimized with better outpatient management of complex children.
Conclusions
Our study suggests that the prevalence of multiple chronic conditions is common among children. Health care expenditures increased with the number of chronic conditions, and children with multiple chronic conditions were more likely to persist as top spenders in subsequent years. Further research into effective ways to manage the health care delivery for children with multiple chronic conditions is needed.
Footnotes
Acknowledgements
We thank Carol Greenlee for preparing the article. The authors would like to thank the Department of Pediatric and Adolescent Medicine (Dr Deborah B. McWilliams, Dr Jill A. Swanson, and Dr Robert M. Jacobson from Mayo Clinic’s Department of Pediatric and Adolescent Medicine) for the enrichment and revision of the article with their clinical expertise in community pediatrics.
Authors’ Note
The sponsor of the study had no role in study design, data collection, data analysis, data interpretation, or writing of the report.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Mayo Clinic Robert D. and Patricia E. Kern Center for the Science of Health Care Delivery.