
Abstract
Approximately 24 million Americans are living with diabetes. 1 Successful management requires coordination of multiple therapeutic modalities, support for patients’ participation in self-management activities, paying attention to diverse cultural attitudes and beliefs, and providing added clinical supports to health care providers.2 -4 Yet most care is provided in a fragmented way with limited connection occurring across the continuum of care between inpatient, outpatient, primary, and specialty care, ancillary providers or community-based care management programs. There are calls for increased integration across the US health care delivery system to improve outcomes for patients with chronic diseases.
Patient-Centered Medical Homes (PCMHs) are viewed as a viable programmatic response to fragmented and poorly coordinated health care services. Features of PCMHs include the provision of quality, continuous, integrated care across a range of clinical and community-based services. 5 Evidence is promising on the effectiveness of PCMHs in improving patient experiences, quality of care, and health outcomes. Reports from observational studies associated with three demonstration projects showed that adoption of the PCMH model is associated with some improvement in health care quality, clinical outcomes, and patient experiences.6-8 PCMH implementation has also been found to be associated with reduced emergency room use and lower total costs of care.9-12
In 2008, the National Committee on Quality Assurance (NCQA) adopted criteria for practice recognition as a PCMH. There are 3 levels of NCQA recognition ranging from level 1 to level 3. To be recognized, using then updated NCQA’s 2011 guidelines, practices must demonstrate that they have met certain standards of care within 6 categories: enhance access and continuity, identify and manage patient populations, plan and manage care, provide self-care and community support, track and coordinate care, and measure and improve performance. 13 PCMH recognition of level 1, 2, or 3 is based on whether specific performance elements within the 6 domains have been achieved and reported to NCQA.13,14 Each domain includes a must-pass element in order to be recognized. In addition, assignment of recognition at level 1, 2, or 3 depends on the number of additional points earned.
Though practices may achieve the same level of NCQA recognition, the manner and approach to implementing elements of the patient-centered medical home model may be different. Differences can be due to practice philosophy, available resources, and overall implementation strategy. Using Donabedian’s framework for understanding quality of care we can assume that the differences in the way PCMHs are implemented (ie, the structure) can result in varying ways of delivering medical care (ie, the process) resulting in different outcomes. 15 This study, seeks to understand whether differences in how a medical home is implemented has any impact on patient reports of care. Understanding these relationships can help primary care practices organize in a way that will improve patient experiences and outcomes.
Methods
This is a mixed-methods study that uses a qualitative approach to describe how 4 primary care clinics implement elements of the PCMH model and attitudes toward that model, as well as a quantitative approach to determine the association between specific practice’s emphasis on PCMH domains and patient engagement and experiences with care. Four primary care clinics that are part of the Department of Family Medicine at an academic health science center located in Florida participated in the study. All of the clinics are located in the same metropolitan area and have a similar organizational structure. The medical directors are employed as faculty members of the university. The clinics were selected based on convenience: Medical directors agreed to participate in the study and provided access to their patients. In addition, all of the locations must have been recognized as an NCQA level 3 patient-centered medical home. Three of the clinics (2, 3 and 4) are similar in size and have between 11 000 and 16 000 patients a year. Clinic 1 is much smaller and sees about 3000 visits a year.
Qualitative Approach: In-depth Interviews With Medical Directors
To understand how the medical home was implemented at the 4 locations, project staff conducted in-depth interviews with medical directors, other providers, and administrative staff at each of the 4 clinics. For consistency, this article reports only on conversations with the medical directors and lead administrators representing 7 interviews. In a separate article, we will report on findings from all participants. Participants were interviewed separately at 3sites. The medical director and the lead administrator participated in the same interview at clinic 1. The interview protocol asked about each element of the PCMH model: the use of information technology, referral procedures, use of health educators and counselors and other care management supports, linkages to community-based programs, and practice culture and characteristics. Each interview took about an hour and occurred in the clinic. The interviews were taped and then transcribed.
A series of codes were developed a priori to catalogue interview content into medical home–related domains. Two investigators coded each transcript. Each individually coded the transcript and catalogue statements into each domain. Then the 2 investigators would compare their coding output and reconcile any differences. At team meetings, project members collectively identified key themes and conclusions. Findings reported in this manuscript emphasize core components of the medical home that we think may directly impact patient experiences with care.
Quantitative Approach: Survey of Clinic Patients
All individuals aged 18 years and older with an ICD-9 (International Classification of Diseases–9th Revision) code indicating diabetes, who had at least 2 visits within the past 2 years were mailed a letter informing them of the purpose of the study and giving them an opportunity to opt out. Stratified by the 4 participating clinics, a total of 5300 letters and brochures were sent with 217 people deciding to opt out. The Survey Research Laboratory at the University of Florida randomly selected individuals within each clinic to telephone for a total of 1301 participants. The cooperation rate (the number of complete interviews divided by the number of telephone numbers contacted ranged from 65% to 73%). The survey instrument included items from the Ambulatory Care Experiences (ACES). This instrument has been extensively tested and validated and has been used in numerous studies.16-18 Using items from the ACES we constructed the following medical home domains: organizational access, comprehensive knowledge, integration and care coordination, communication, health promotion, interpersonal treatment, and trust. Items used for each domain are listed in Table 1. For domains that consisted of multiple questions, the items were added together and then high-, low-, and medium-level categories were created based dividing the distribution into thirds. For the single-item domains the response structure was never, almost never, sometimes, usually, almost always, and always were assigned a score from 1 to 6. Bivariate and ordinal logistical analyses were conducted to determine how PCMH experiences varied by site of care. To protect anonymity, clinics are referenced as “clinic 1,” “clinic 2,” “clinic 3,” and “clinic 4.” Since there is variation in the sites by key demographic characteristics, we controlled for age, gender, marital status, educational attainment, and self-reported health status in the regression analysis. We recognized that the observations are likely to be highly correlated around the site of care. We therefore computed models that controlled for patient clustering by practice to allow for robust standard errors.
Ambulatory Care Experiences Survey Medical Home Domains.

Adapted from Safran et al. 16
Results
Qualitative Analysis
While all 4 practices have NCQA accreditation, the degree and manner in which medical home components have been adopted vary. Information from participants revealed differences in use and perception of value of information technology, use and perception of disease management supports, and the extent to which clinics link to community-based services. For example, while 1 clinic extensively used a diabetes registry, the other 3 clinical centers reported not having the capacity to implement registries. The use of disease management supports also differed where 2 clinics were structured to refer patients to other sites for diabetes education or nutritionists, while 2 clinics had substantial onsite medical support services to provide to patients; for example, one clinical center had an onsite diabetes educator, pharmacist and podiatrist while the other clinical center employed pharmacists and psychiatrists as well as offered diabetes education, smoking cessation, and pain clinics to patients.
Each of the 4 clinics linked patients to community services differently; providers at 2 centers knew of community resources and referred patients when possible. However, no formal process for referring patients, or partnership with the center and the community organization was established. Providers at another center reported using an extensive list of community resources to refer patients, such as food pantries, homeless shelters, and disability services. However, they also reported that no formal partnership between the clinical center and the community organization/agency in which they refer patients has been established. On the other hand, providers at one clinical center reported having established relationships with community organizations/agencies, including programs specializing in diabetes and exercise, to which to refer patients. They also report the need to link patients to services based on the patients’ insurance, as well as their location. Based on qualitative results, the study team concluded that one clinic had a much stronger PCMH orientation compared with other sites of care. This clinic was chosen as the referent clinic for the multivariate models and will be referred to as “clinic 1.” Additional findings from the qualitative analysis are reported elsewhere. 19
Quantitative Analysis
Table 2 shows differences in demographic characteristics across the sites of care. A greater proportion of patients at Clinic 1 are white, married, have education ≥12 years, and are in excellent or good health. At the time of the study, clinic 1 has only been opened for 4 years, and consequently those patients report a shorter length of time with this clinic. These factors were adjusted for in multivariate models because of the differences in patient characteristics across the clinics.
Sample Characteristics by Clinic: Adults With Diabetes With at Least 2 Primary Care Visits Within a 2-Year Period (N = 1301).

P <. 05.
Table 3 shows results from the ordered logistic models that compare Clinic 1 to other clinics on PCMH domain ratings. Overall, the odds of patients reporting higher domain ratings were significantly lower for the other 3 clinics compared with the clinic with the stronger PCMH orientation (Clinic 1). Specifically, patients from Clinic 1 were significantly more likely to feel that their medical center had adequate communication, health promotion, interpersonal treatment, trust, organizational access, comprehensiveness, integration and adequate office staff compared with patients from clinics 2, 3, and 4. Confidence intervals between clinics 2 and 4 tend to overlap for all domains except trust and integration, indicating that the likelihoods of a high rating on domains are not different for these locations. Relative to clinic 1, clinic 3 has the lowest odds of a higher rating on any domain compared with clinics 2 and 4.
Ordered Logit: Associations Between Primary Care Clinic and Positive Ratings of Patient-Centered Medical Home–Related Aspects of Care Among Patients With Diabetes at 4 Clinics. a

Models control for: race and ethnicity; age; marital status, educational attainment, self-reported health status; length of time at practice, and age.
P < .0001.
A graphic representation of these findings is displayed in Figure 1. The graph shows that confidence intervals between clinics overlap in some instances indicating that the likelihood of a higher rating on those domains is not different across these locations. For example, within the communication domain, clinics 2 and 4 have overlapping confidence intervals. However, clinic 3’s confidence interval does not overlap with those of clinics 2 or 4. For the trust domain none of the confidence intervals overlap indicating that odds of providing a higher rating are different for each clinic.
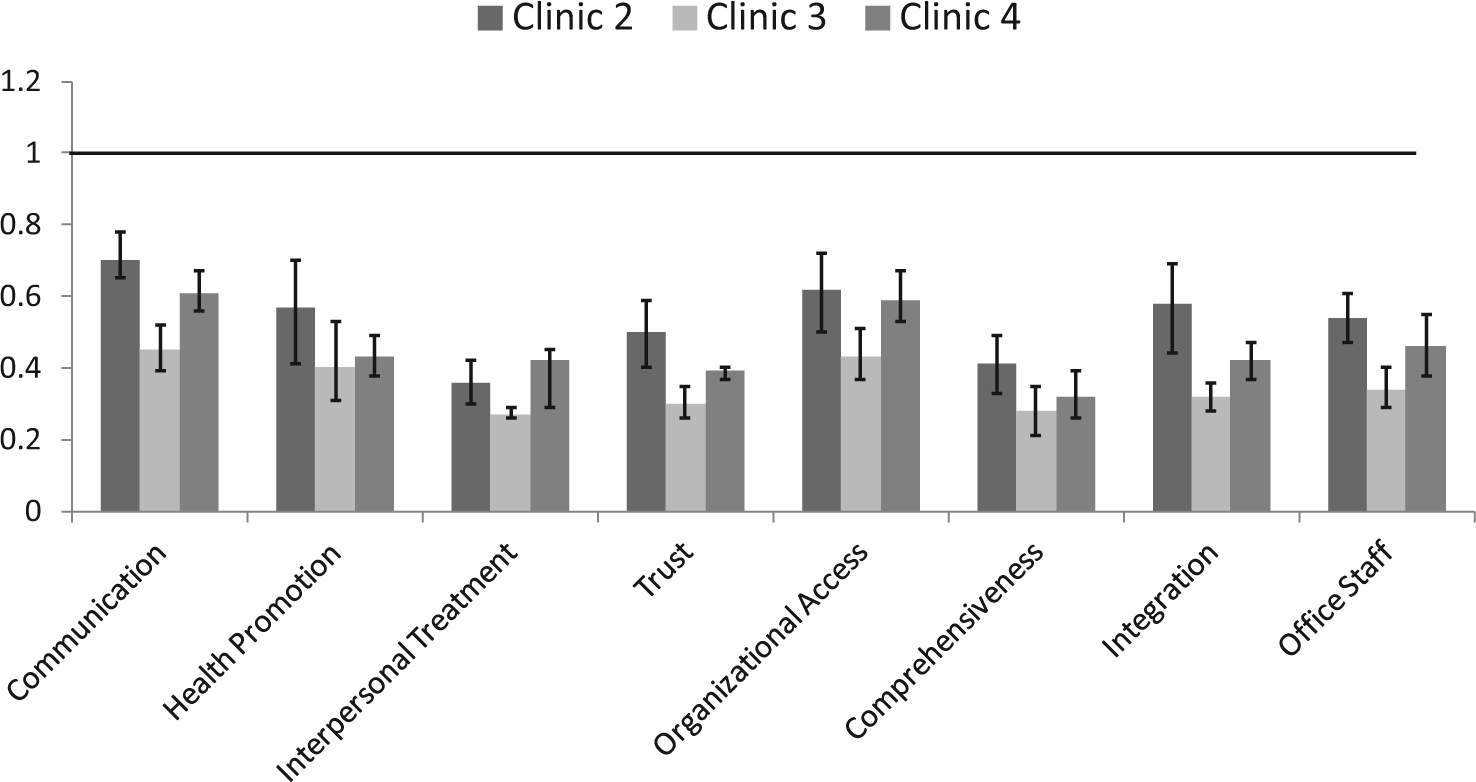
Odds ratios showing likelihood of positive ratings of patient-centered medical home aspects of care among patients at clinics 2, 3, and 4 (relative to clinic 1).a
Discussion
As expected, the odds of providing higher domain ratings were lower for the other 3 clinics compared with clinic 1. In addition, the magnitudes of the differences from clinic 1 appear to be similar across the clinics regardless of the outcomes. Clinic 1 has been participating in the Florida Academy of Family Physician’s Master Diabetes Clinician Program. The program is built on 2 principles, using a chronic disease registry to optimize diabetic patient’s chronic care and enhanced training for medical staff to become active participants in diabetic care. The enhanced training is an essential component of team-based care and has allowed the staff at clinic 1 to engage their diabetic patients on multiple levels of care. The registry prints out diabetic report cards for the patients at each of their chronic diabetes care visits which are written in a language the patients can easily understand and compares the numbers versus their previous visits. It also alerts the patient and staff if the patient is due for their annual diabetic care, that is, influenza vaccine, monofilament exam. Many patients feel empowered by these report cards to participate further in their diabetic care.
We note that the characteristics of patients in clinic 1 differ from patients in the other 3 clinics. These demographic characteristics could provide a partial explanation for why ratings of the PCMH domains are more favorable in clinic 1 compared with the other locations. Higher proportions of individuals in clinic 1 are high school graduates, White non-Hispanic, and in excellent or very good health. These individuals may be more likely to provide positive reports regardless of where they receive care. However, we controlled for these demographic characteristics in our analyses. Furthermore, our qualitative research highlighted substantive differences in the way care is provided across the clinics. Consequently, we feel confident that higher scores are associated at least in part with how care is provided in clinic 1.
This study emphasizes the importance of team-based care, chronic disease registries, and patient engagement as important components of the journey from theory to practice of the PCMH. Primary care clinics wishing to improve experiences of care, might consider ways in which team-based care can be incorporated into the practice. In addition, it demonstrates that not all PCMH clinics are alike, even though they all achieved the same level of NCQA accreditation, and that these differences can affect patient perceptions of their care. Further research is needed in 2 areas. First, there should be continued exploration in understanding the differences in PCMH operationalization. Nuances to the model could likely result in differences in outcomes of care. Second, research should focus on identifying which elements of the PCMH model provide the greatest benefit to patients. Such work would inform practices as to which components of the model they wish to emphasize as they undergo PCMH transformation.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Supported by The Aetna Foundation, a national Foundation based in Hartford, Connecticut that supports projects to promote wellness, health and access to high quality health care for everyone. The views presented here are those of the author and not necessarily those of The Aetna Foundation, its directors, officers, or staff.