
Abstract
The patient-centered medical home (PCMH) is an integrated primary care delivery model particularly suited for patients with poor diabetes control. Although PCMH models targeting adults with diabetes have shown some early success, little is known about the long-term benefits of medical homes in terms of health and cost outcomes. The performance of a PCMH model in adults with poor diabetes control was assessed using simulated controlled trial data obtained from the Archimedes model of disease progression and health care utilization. Using the Cardio-Metabolic Risk data set, we compared health and cost outcomes over a 20-year period between adults with poor diabetes control (HbA1c >9%) receiving standard care and these same adults receiving care under a PCMH model with a 49% HbA1c intervention improvement rate at a per-beneficiary per-month care management cost of $20 per month. The results suggest that the PCMH model has the potential to not only reduce the proportion of the population with bilateral blindness, foot amputations, and myocardial infarctions—and the mortality rate—but it can also do so in a cost-effective manner ($7898 per quality-adjusted life year). The PCMH model is cost saving for the population 50 to 64 years old and it is particularly cost-effective for men ($883 per quality-adjusted life year). Moreover, these effects are relatively large for adults 30 to 49 years old (lower bilateral blindness and death rates), women (lower foot amputation and death rates), and men (lower bilateral blindness and myocardial infarction rates). The PCMH model has potential long-term benefits to both patients with poor diabetes control as well as health care systems and providers willing to invest in this health care delivery approach.
Introduction
The patient-centered medical home (PCMH) is a primary care delivery model based on the idea that patients should have access to high-quality, integrated health care services that are comprehensive, team-based, and appropriately coordinated. 1 Under the PCMH model, each patient has a personal physician who is the first point of contact for any health issues that may arise with the patient. The physician also leads a health care team—composed of both physicians and other health care providers—that is easily accessible to the patient. It is not surprising then that the PCMH model has become a very attractive approach to structuring the delivery of health care services for patients with type 2 diabetes, a chronic disease requiring intensive health management to effectively keep it under control. 2
Diabetes is increasingly prevalent and costly. 3 The Centers for Disease Control and Prevention estimates that 1 in 12 Americans have diabetes, and 79 million American adults are prediabetic. In the United States, diabetes costs $116 billion annually in direct medical expenses. 4 The high costs and rising prevalence of diabetes strongly suggest the need to find cost-effective approaches to diabetes management. Diabetes management and the PCHM model are increasingly interwoven. Diabetes management highlights the potential strengths of the PCMH model, and the PCMH model provides promise for improved diabetes management. Managing diabetes with coordinated care provided by a team of clinicians and educators has been documented to improve short-term patient outcomes, reduce risk of complications and reduce payer costs. 5,6 Moreover, the American Diabetes Association and the American Association of Diabetes Educators have both endorsed the use of team-based disease management, a central element of the PCMH model. 7
Several demonstration studies have shown that diabetes patients experience substantial improvements in short-term health outcomes and incur lower health care costs in medical practices that implement a PCMH initiative. 2 For example, the Veterans Integrated Service Network 23 piloted a PCMH model—the Patient Aligned Care Team (PACT)—which served 2407 beneficiaries from July 2008 to August 2009. 5 The percentage of PACT diabetes patients with HbA1c <9% increased from 91% to 96% compared to an increase from 90% to 92% for non-PACT patients in the same facility over a 12-month period. PACT diabetes patients also experienced improvements in blood pressure and lipid control, and had lower hospitalization rates than non-PACT diabetes patients. 1 Other PCMH initiatives that have shown substantial improvements in health and quality outcomes—together with reductions in overall health care expenditures—include the medical home models implemented at the Geisinger Health System, the Pennsylvania Chronic Care Initiative, and the Washington’s Group Health Cooperative. 8 -11
Although PCMH models targeting adults with diabetes have shown some early success, it is more difficult to know the long-term benefits of medical homes in terms of health and cost outcomes. Adopting a PCMH model is likely to be costly in the first few years of operation while the benefits to patients oftentimes will be evident farther into the future (eg, the prevention of a foot amputation or blindness for a patient 20 years after a diabetes diagnosis). The purpose of this study is to identify the long-term health and cost outcomes of implementing a PCMH model for adults with poor diabetes control based on simulated clinical trial data obtained from the Archimedes model of disease progression and health care utilization.
Research Design and Methods
For this study, the Cardio-Metabolic Risk (CMR) data set derived from the Archimedes model provided simulated controlled trial data which allows us to evaluate what would occur if the PCMH model of care was implemented to treat adults with poorly controlled diabetes. 12 The Archimedes model simulates populations and clinical interventions, models the expected health outcomes of individuals and estimates the expected health care costs associated with those outcomes. The model can be used to estimate the expected cost and health outcomes that would be incurred by a simulated cohort of individuals who receive usual/standard care in the United States and to calculate the effects that an intervention may have on expected health and cost outcomes. 13
The Archimedes model was used to analyze the health and cost effects of using a PCMH model of care to treat adults with poor diabetes control (i.e., adults with an HbA1c >9%). Archimedes models health outcomes over time using mathematical equations to represent the onset and progression of different health conditions such as diabetes and cardiovascular disease. This mathematical representation of disease progression also includes interactions that a patient may have with the health care system over the life course. Such interactions include, among others, physician visits, prescription drug treatments, behavioral interventions, tests, procedures, and hospital admissions. 14
The results from 2 Archimedes model simulations for a population of adults with HbA1c >9% available in the CMR data set were used to evaluate what would happen to this population over 20 years—in terms of health and cost outcomes—if they reach HbA1c targets under a PCMH model compared with what would happen to the same population receiving usual care in the United States. 12
The Archimedes model has been validated for its use in simulating actual outcomes for diabetes and other diseases. There have been 69 external validation exercises comparing simulated and actual outcomes from clinical trials and cohort studies for disease complications and incidence such as myocardial infarction, diabetes incidence/complications and death. 14 The Archimedes model has been validated specifically for its accuracy in predicting the onset of diabetes and subsequent complications, and it has been used extensively to conduct cost-effectiveness studies related to diabetes care. 15 -19
The CMR data set includes the results from 19 simulated controlled trials comparing standard care (i.e., adults treated using national guidelines of care, with an average treatment adherence level to these recommendations) to interventions targeting diabetes, obesity, and cardiovascular disease. The Archimedes model simulations available in the CMR data set included the results for 100 000 individuals between 30 and 85 years old who are representative of the U.S. population (based on the National Health and Nutrition Examination Survey 1999-2006). 12 The simulated controlled trial data were analyzed using the Archimedes Healthcare Simulator (ARCHeS) Web-based interface to the Archimedes model. ARCHeS was developed with funding from the Robert Wood Johnson Foundation and it is widely used for comparative effectiveness and policy analyses. 13
Our analyses were conducted using one of the trials available in the CMR data set based on a simulated adult population with HbA1c >9%. We compared the long-term health and cost outcomes for adults with HbA1c >9% who received standard care for 20 years to the outcomes that would occur if 49% of those same adults were able to reduce their HbA1c <9% for the same time period. A 2012 report reviewing the benefits of implementing PCMH models included diabetes glycemic control improvement outcomes for seven out of 34 initiatives implemented across the U.S., with a median improvement rate of 49%. 1 This is the same rate we used in the simulation.
The costs of PCMH interventions vary widely and they are difficult to identify because typically they are aggregated with health care utilization costs. The additional costs of adopting a PCMH model focus on care coordination and information technology. 20 As such, we used the average $20 per-beneficiary per-month care management payment for fee-for-service Medicare beneficiaries used by the Centers for Medicare & Medicaid Services (CMS) in the Comprehensive Primary Care Initiative to approximate the additional care coordination costs related to adopting a PCMH model. 21 This CMS program uses and extends the patient-centered medical home concept (the Joint Principles of the Patient-Centered Medical Home) to support the transformation of medical practices into medical homes, with an emphasis on multipayer payment reform and information technology. 21
Results
Table 1 presents the descriptive statistics for the simulated cohort of adults with HbA1c >9% (n = 1961). About one third of the simulated cohort of adults with poor diabetes control was between 65 and 85 years old, 40% were 50 to 64 years old, and 28% were 30 to 49 years old. More than half of the simulated cohort (53%) were men and the average body mass index and HbA1c were 33.39 kg/m2 and 10.48%, respectively. About one fifth (19%) of adults with poor diabetes control were smokers, with a fasting plasma glucose of 249 mg/dL, systolic blood pressure of 128 mm Hg, diastolic blood pressure of 71 mm Hg, and an average weight of 94 kg.
Descriptive Statistics of Simulated Sample.
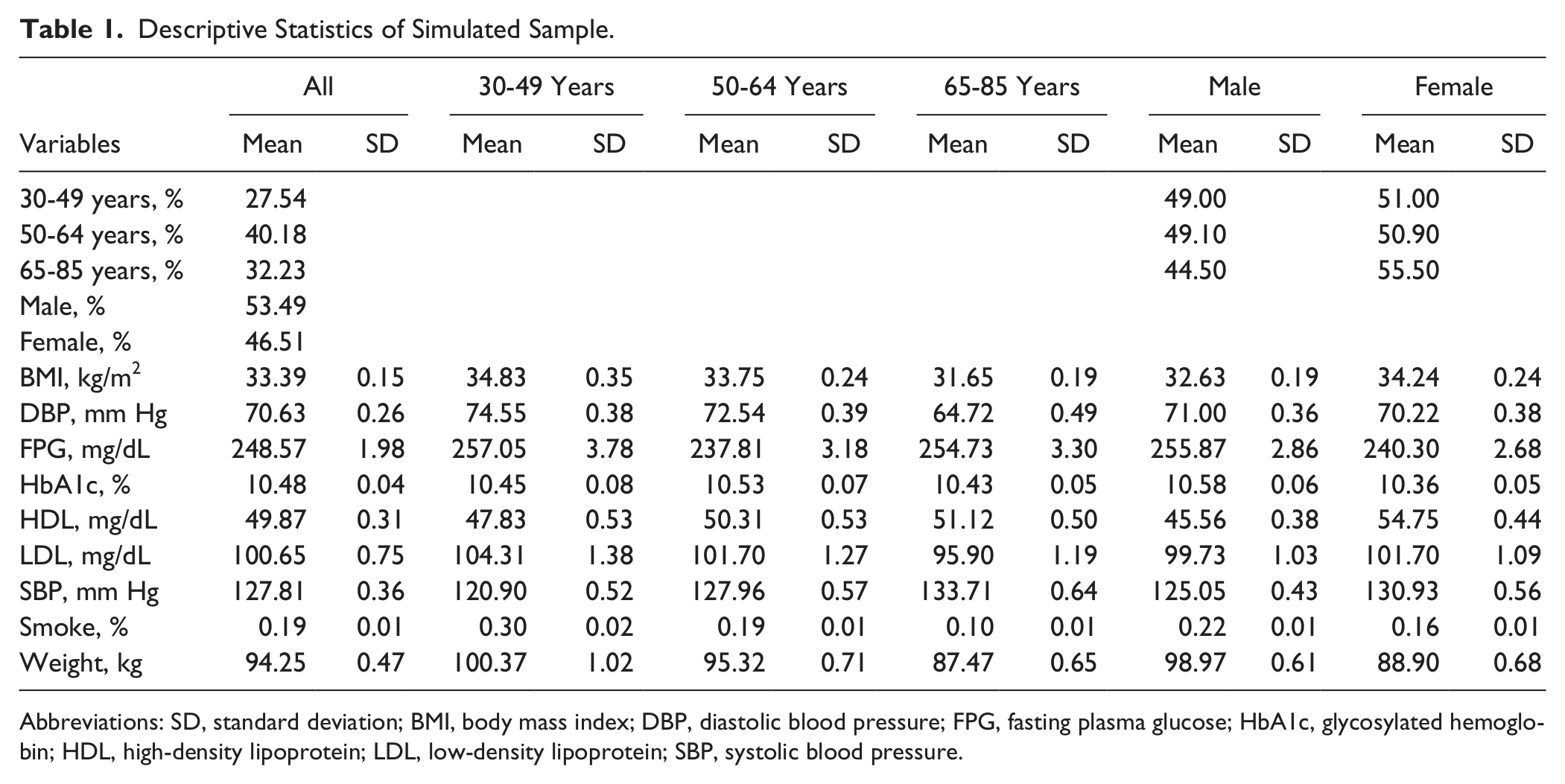
Abbreviations: SD, standard deviation; BMI, body mass index; DBP, diastolic blood pressure; FPG, fasting plasma glucose; HbA1c, glycosylated hemoglobin; HDL, high-density lipoprotein; LDL, low-density lipoprotein; SBP, systolic blood pressure.
Table 2 reports the intervention effects and the cost per quality-adjusted life year (QALY) of the PCMH intervention. The Archimedes model simulation indicated that 7.1% of adults 30 to 85 years old with poor diabetes control (HbA1c >9%) will experience bilateral blindness, but this proportion would be 1.2% lower under a PCMH model with a 49% HbA1c intervention improvement rate. The relative PCMH intervention effect on bilateral blindness was the largest for adults 30 to 49 years old (3.71%) and men (1.79%). About 34% of simulated adults with poor diabetes control will experience a foot amputation and this proportion would be 11.47% lower under the PCMH model considered. The relative PCMH intervention effect for foot amputations was particularly large for women (14.62%) and adults 50 to 64 years old (13.20%).
PCMH Intervention Effects and Cost per QALY Over a Simulation Period of 20 Years.

Abbreviations: PCMH, patient-centered medical home; QALY, quality-adjusted life year; MI, myocardial infarction.
Almost 25% of simulated adults with poor diabetes control will experience a myocardial infarction and this proportion would be 9.80% lower under the PCMH model considered. The relative PCMH intervention effect for myocardial infarctions was particularly large for men (11.10%) and adults 50 to 64 years old (11.03%). Half (50.22%) of simulated adults with poor diabetes control would have died in 20 years, and the death rate would be 1.22% lower under the PCMH model considered. The relative PCMH intervention effect for deaths was particularly large for adults 30 to 49 years old (3.96%) and women (1.97%).
The PCMH intervention was cost-effective (cost/QALY = $7898) and is cost saving for adults 50 to 64 years old (the pre-Medicare population) and relatively more cost-effective for men (cost/QALY = $883) than for women (cost/QALY = $16 649). The intervention would increase the number of life years by 117 and the number of QALYs by 169 over 20 years for the simulated cohort of 1961 adults with HbA1c >9%.
We also conducted sensitivity analyses to see how the cost-effectiveness results would change if the per-beneficiary per-month care management payment would increase from $20 to $40. This alternative care management payment is actually equal to the highest risk-adjusted care management payment under the Comprehensive Primary Care Initiative by CMS. 21 Under this higher payment, the PCMH intervention would be cost-effective for all adults (cost/QALY = $27 918) as well as for all subgroups (cost/QALY = $30 546 for adults 30 to 49 years old, $23 777 for adults 50 to 64 years old, $30 076 for adults 65 to 85 years old, $38 787 for women, and $19 273 for men).
Conclusions
Patient-centered medical home models have shown promise in improving relevant short-term health and quality outcomes, but little is known about their long-term prospects for both patients and the health care delivery system. Using simulated CMR data from the Archimedes model, we compared health and cost outcomes over a 20 year period between adults with poor diabetes control (HbA1c >9%) receiving standard care and these same adults receiving care under a PCMH model with a 49% HbA1c intervention improvement rate at a per-beneficiary per-month care management cost of $20 per month. Our results suggest that the PCMH model has the potential to not only reduce the proportion of the population with bilateral blindness, foot amputations, and myocardial infarctions—and the mortality rate—but it can also do so in a cost-effective manner ($7898 per QALY).
The PCMH model is cost saving (i.e., over a 20-year period, costs will be lower and QALYs will be higher under the PCMH model than under usual care) for the population 50 to 64 years old, and it is particularly cost-effective for men ($883 per QALY). Moreover, these effects are relatively large for adults 30 to 49 years old (lower bilateral blindness and death rates), women (lower foot amputation and death rates), and men (lower bilateral blindness and myocardial infarction rates).
Some gender differences in projected outcomes may be explained by differences in diabetes progression and outcomes that have been found to exist between women and men. 22 -25 Outcomes that differ by gender become more pronounced as the events accumulate over time. Possible causal mechanisms to explain gender differences in diabetes-related health outcomes include a greater impact of low-grade inflammation on insulin action in women and adverse effects on female hormones that regulate body fat distribution and insulin. 23,26 As these biological differences influence the progression of diabetes, they also may have an impact on how behavioral and medical interventions affect health outcomes.
There are several limitations to our study. First, although our results are based on a simulation model that is very realistic and complete, the Archimedes model—like any other simulation approach—does not necessarily capture all the intricacies about how individuals interact with the health care system. Second, we assumed a 49% improvement rate for the diabetes intervention and a $20 per patient per month cost of the PCMH model. Although these assumptions are based on existing information on short-term diabetes-related health outcomes and current reimbursement levels of care coordination, our estimates will be different if either the improvement rates or the cost of implementing a PCMH model change over time.
Still, our study suggests that the PCMH model has long-term benefits to both patients with poor diabetes control as well as health care systems and providers willing to invest in this promising health care delivery approach. Further research studies are needed to evaluate how the PCMH model would perform for adults with other relevant chronic health conditions such as obesity and cardiovascular disease, particularly for those with multiple comorbidities, which are the main target of the PCMH primary care model.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies