
Abstract
Introduction
Health care professionals (HCPs) play a prominent role in promoting tobacco control and smoking cessation programs. However, their smoking habits may prevent them from providing unbiased advice on smoking cessation 1 and may even prevent them from being efficiently involved in cessation programs designed for patients. 2 HCPs are not immune to the addictive effects of smoking, and their professional role may at times conflict with their personal choice of smoking. 3 Historically, public health efforts have focused on smoking-cessation programs for the general population. However, smoking by certain HCP groups has not received as much attention and determinants of smoking have not been studied in depth in this occupational group.
The purpose of this analysis was to estimate prevalence rates of current smoking among 4 groups of health care professionals: physicians, nurses, respiratory therapists, and occupational therapists and to identify sociodemographic and work-related factors that may contribute to smoking among HCPs.
Methods
This analysis is based on a cross-sectional study designed to evaluate the prevalence of new-onset asthma and associated occupational factors among licensed HCPs. The statewide self-reported mail survey was based on a representative random sample of HCPs aged 18 years and older with active professional licenses in Texas in 2003. The survey was completed by 3650 HCPs, including physicians (n = 862), nurses (n = 941), occupational therapists (n = 968), and (n = 879) respiratory therapists, corresponding to a participation rate of 66%. A detailed description of the survey can be found elsewhere. 4 The main dependent variable was current smoking. A binary current smoking status variable was constructed using the following questions from the questionnaire “Have you smoked at least 100 cigarettes during your life?” and “Do you smoke cigarettes now?” Those who responded in affirmative to both questions were coded as current smokers. Information on smoking status was missing on 50 subjects, leaving the final sample size of 3600 for analyses. Number of hours worked each week was assessed using the following question from the questionnaire “How many hours per week did you usually work on this job, including overtime?” HCPs’ working hours were categorized into <40 h/wk, 40 to 49 h/week, and ≥50 h/wk. Years working as a HCP was based on the following questionnaire item: “How many years have you worked as a health care professional?,” and collapsed into 2 categories: <10 years and ≥10 years working as a HCP. Body mass index (BMI) was calculated based on self-reported height and weight and grouped into normal weight (BMI < 25 kg/m2), overweight (25 < BMI < 29.9 kg/m2), and obese (BMI ≥ 30 kg/m2). Geographical location was defined as rural if the ZIP code was located in a county with a population less than 50 000; otherwise, it was considered to be urban. Other covariables included age (<30, 30 to <45, 45 to <60, and ≥60 years), sex, race/ethnicity (non-Hispanic black, non-Hispanic white, Hispanic, and other race/ethnicity), and profession (physicians, nurses, respiratory therapists, and occupational therapists). Sample weights were computed using poststratification to obtain prevalence estimates representative of actual population sizes of each health care professional group. Simple descriptive statistics were used to examine the sample characteristics, and to estimate current smoking prevalence professional status. Univariable and multivariable logistic regression analyses were performed to explore the association between independent and dependent variables. Interaction between years worked as a HCP and working hours was explored. All analyses were performed using Stata version 12.0 statistical software package using its survey feature (StataCorp, College Station, TX). The parent study was approved by the Human Subjects Committee of the University of Texas, School of Public Health at Houston. The Institutional Review Board of the University of North Carolina at Charlotte approved access to and analysis of the data for the purpose of this study.
Results
Table 1 describes the characteristics and estimated prevalence of current smoking in the study population. The mean age of the study participants was 45.3 years (SD = 11.9 years). The majority of respondents were female (77%) and self-identified as non-Hispanic white (72%). An estimated 55% of HCPs were overweight or obese. The majority of respondents reported living in an urban area, had worked 10 years or more as HCP, and were working full time (40 hours or more per week) at their current or most recent job as a HCP. The overall estimated prevalence of current smoking was 9% among HCPs, but this differed significantly across the 4 professional groups. It was higher among respiratory therapists (16%) followed by nurses (11%), occupational therapists (7%), and lowest among physicians (3%). Prevalence was significantly higher among females, non-Hispanic whites, and those living in rural areas (Table 1).
Baseline Characteristics and Estimated Prevalence (%) of Current Smoking in the Study Population.

Abbreviations: SD, standard deviation; BMI, body mass index; HCP, health care professional; NS, nonsignificant.
Unweighted n and weighted % are reported.
P values were derived from χ2 tests.
Female HCPs had a 76% greater odds of current smoking in the unadjusted analysis (odds ratio [OR] =1.76, 95% confidence interval [CI] =1.18-2.63). When compared with non-Hispanic black HCPs, non-Hispanic white HCPs had almost 4 times the odds of current smoking (adjusted OR = 3.95, 95% CI = 1.24-12.59). Those who reported working and/or living in rural areas were more likely to be current smokers (unadjusted OR = 1.60, 95% CI = 1.02-2.50). However, the OR became statistically nonsignificant when adjusted for other variables in the model. No relationship between years working as a HCP and current smoking was observed in the study. However, the odds of current smoking were significantly greater for HCPs working for 50 hours or more per week, and increased in a dose-dependent manner from 1.26 (95% CI = 0.78-2.04) for HCPs working 40 to less than 50 hours per week to 2.07 (95% CI = 1.20-3.57) for HCPs working 50 hours or more per week, as compared with those working less than 40 hours per week (Table 2). Similarly, compared with physicians, the odds of current smoking were significantly greater for nurses (adjusted OR = 4.63, 95% CI = 2.46-8.72), respiratory therapists (adjusted OR = 7.94, 95% CI = 4.45-14.16), and occupational therapists (adjusted OR = 3.23, 95% CI = 1.65-6.32; Figure 1). There was no evidence of interaction between weekly working hours and years working as a HCP was not statistically significant (P > .05; data not shown).
Unadjusted and Adjusted Odds Ratios (95% Confidence Intervals) of Current Smoking Among Health Care Professionals.
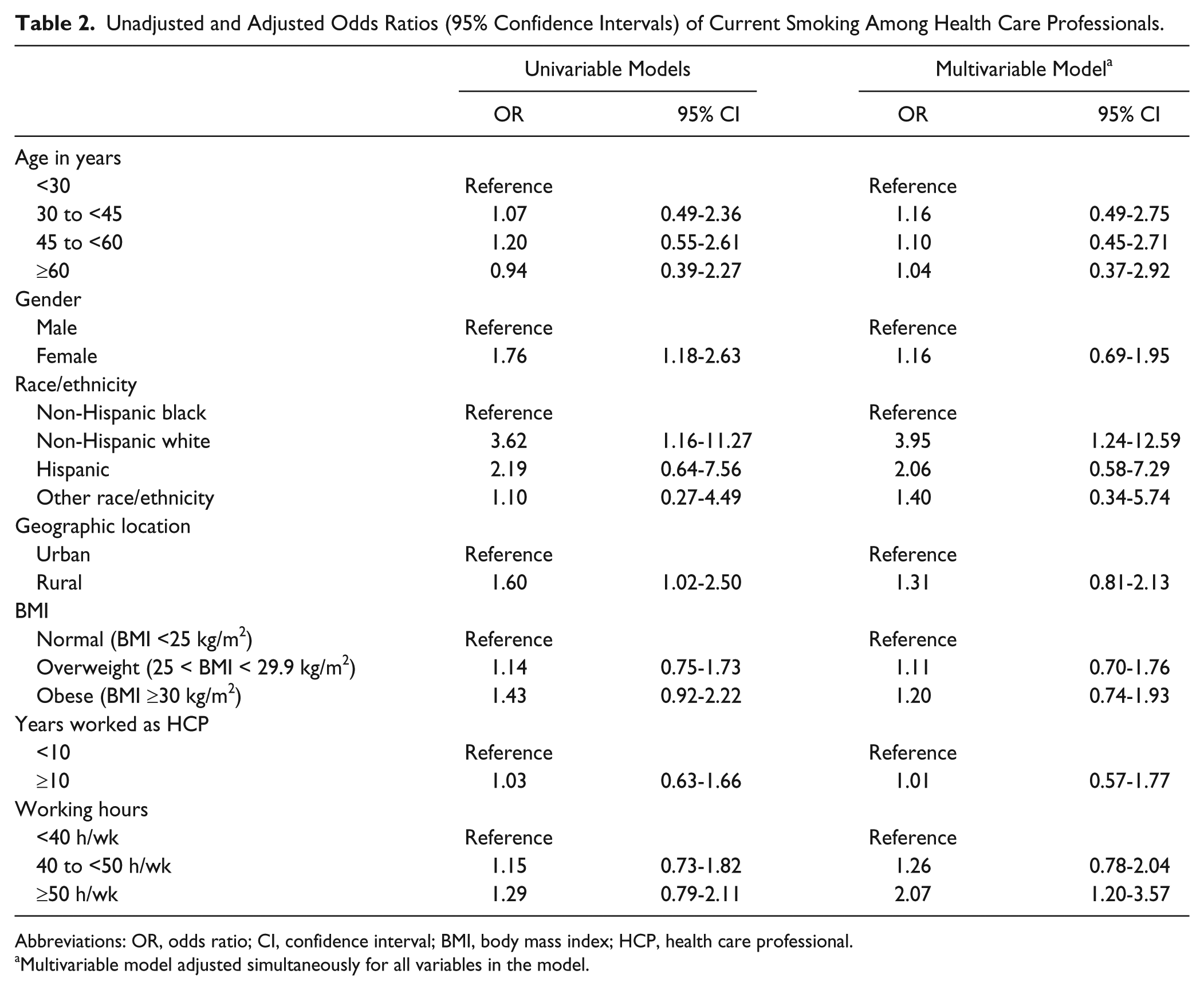
Abbreviations: OR, odds ratio; CI, confidence interval; BMI, body mass index; HCP, health care professional.
Multivariable model adjusted simultaneously for all variables in the model.

Adjusted odds ratio (95% confidence intervals) of association between health care professional groups and current smoking.a
Discussion
This study found that prevalence rates of current smoking are highest among respiratory therapists, followed by nurses, occupational therapists, and physicians. Working long hours was associated with increased odds of current smoking among HCPs.
The prevalence of smoking in this study varied from 3% among physicians to 16% among respiratory therapists. The odds of current smoking were more than 7 times elevated among respiratory therapists as compared with physicians (Figure 1). According to data from the National Health Interview Survey, approximately 19% of the working adult US population smoke cigarettes and the prevalence of current smoking in health care practitioners and technical occupational group is approximately 12%. 5 However, information regarding smoking practices among different HCP groups in the United States remains relatively sparse. Sarna et al, 6 using data from the Tobacco Use Supplement of the Current Population Survey reported the prevalence rate of current smoking rates in 2003 of 15.5% among respiratory therapists, 11.1% among registered nurses, and 2.2% among physicians, similar to our study. The rates remained relatively unchanged in 2006-2007 for registered nurses and physicians, but increased to 19.5% for respiratory therapists. Respiratory therapists, who frequently interact with smokers, play a vital role in promoting smoking cessation programs in health care settings. 7 The high smoking rates among respiratory therapists indicate a persistent issue in this professional group. Although smoking among nurses has declined over the past decade, 8 this decline is limited to registered nurses as the smoking rates among licensed practical nurses are higher than the estimated rates in the general population, 6 raising questions if income and education disparities between registered nurses and licensed practical nurses could partly be responsible. The smoking rates among physicians are generally the lowest of all the HCP groups in the United States, similar to other developed countries, including Australia, New Zealand, and the United Kingdom.9,10 The prevalence of smoking was 7.0% among occupational therapists in our study, but to our knowledge, this is the first study reporting smoking prevalence rates in this HCP group. More studies are needed to explore if their smoking behavior has any effect on their interaction with patients.
We also found a statistically significant association between current smoking and working hours, with a greater than 2-fold increase among HCPs working 50 or more hours per week. It is well established that working conditions vary across different groups of HCPs 11 and that working long hours and engaging in shiftwork contribute to smoking among HCPs. Previous studies found lower quit ratios among HCPs with higher weekly working hours, extensive work shifts, higher workloads, and more conflicts at the workplace than among those with better working conditions and flexible working hours. 11 In Germany, a greater degree of nicotine dependence was found among participants working 15 or more hours per week. 12 Working long hours may result in stress, which makes individuals engage in unhealthy behaviors such as smoking as a coping mechanism. 13
Current smoking was highest among non-Hispanic white HCPs, which reflects the national trend observed in the general working adult US population. 5 However, higher weighted prevalence rates observed among female HCPs was opposite the national trend in the US general population, where smoking rates are generally greater among men. 5 The higher smoking rates observed among female HCPs observed in this study could partly be explained by the fact that the majority of female HCPs were nurses and smoking rates among certain group of nurses, such as licensed practical nurses, are generally higher than the general population. 6 Smoking to cope with work-related stress could be a plausible explanation for the higher rates observed among female HCPs in this study. Nurses working long hours are more likely to experience fatigue, anxiety, and exhaustion. 14 Further analysis of our data revealed that smoking rates were elevated (albeit nonsignificantly) for female HCPs across all categories of weekly working hours, with the highest prevalence recorded for those working 50 hours or more per week (12.9%, Figure 2). Future studies should evaluate work stress levels among HCPs.

Prevalence and 95% confidence intervals of current smoking among health care professionals by gender and weekly working hours.
Rural residence was related to current smoking in the univariable analysis only. Smoking prevalence rates in the United States are generally higher for rural residents as compared with urban residents. 15 The higher prevalence of smoking among rural residents is generally associated with presence of certain sociodemographic characteristics such as low income, low educational attainment, and lack of health coverage.15-17 However, it is unlikely that any of these factors contribute to higher smoking rates observed among rural physicians. Whether underreporting of smoking among physicians can explain this discrepancy should be explored in future studies.
One of the major limitations of this study is that the data are 10 years old. In a recent update to their 2006-2007 data from the Tobacco Use Supplement of the Current Population Survey, Sarna et al 18 reported a significant decline in current smoking rates among registered nurses only (2010-2011, 7.1%), after remaining steady from 2003 (11.1%) to 2006-2007 (10.7%), whereas the rates among licensed practical nurses were virtually the same as in 2003. However, the most current data (2010-2011) on smoking rates among registered nurses were based on very small numbers (n = 116) as compared with 2003 (n = 272) and 2006-2007 (n = 254). Hence, more studies using larger study sample, like ours, are needed to confirm the trend observed among registered nurses. In addition, there were no data reported on smoking rates among occupational therapists, an important emerging occupational group.
The cross-sectional nature of the study precludes us from making any conclusions regarding the temporal sequence between explanatory variables and current smoking. Additionally, the use of secondary data analysis limits the study to examine the association of only a few variables with smoking status. Self-reported smoking data may be subject to social desirability bias. In a recent systematic review, Connor Gorber et al 19 reported that self-reported smoking history generally underestimates the smoking prevalence. There could have been the possibility that some HCPs have underreported their smoking behaviors to avoid any work-related conflicts. It was not possible to determine the degree of underreporting of smoking status in the survey.
In conclusion, smoking is not uncommon among HCPs. Although, HCPs’ smoking behavior may not be an occupational health priority, it is still a public health concern, particularly among respiratory therapists and nurses who play a critical role in the success of patients’ smoking-cessation procedures. Additional epidemiological research using prospective cohort design should be considered to examine longitudinal changes in smoking trends among HCPs. In addition, cessation interventions to reduce smoking rates among high risk HCPs should be considered at hospital and health care settings.
Footnotes
Acknowledgements
We are grateful to Dr. George Delclos, MD, PhD, for providing access to data and reviewing this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by Grant Nos. 5R01OH03945-01A1 and T42CCT610417 (PI: George Delclos) from the National Institute for Occupational Safety and Health/Centers for Disease Control and Prevention.