
Abstract
The recognition and assessment of organizational social context (culture, climate and morale) is particularly valuable in primary health care. Both culture and climate have been shown to be associated with work morale and to predict job satisfaction, organizational commitment and voluntary turnover of employees in nursing. This study aims to describe the social contexts of primary health care centers from the viewpoint of health care professionals. A descriptive study using an organizational social context instrument for data collection was undertaken. From 29 teams in 18 public primary care centers of one Lithuanian county, 344 health care professionals participated. The results of the study show that different organizational cultures, climates and levels of morale existed in primary health care centers, at both team and organizational levels. The differences between teams were significant in terms of culture rigidity and resistance. Climate differences were found at both team and organization levels in regard to stress and functionality. A variance of about 7% in work morale was seen in teams and organizations. Managers should recognize the different kinds of social contexts in which teams work, in order to enable them to co-work efficiently in evidence-based primary care settings.
Keywords
Introduction
Organizational social context consists of three dimensions: organizational culture, organizational climate, and work attitudes (morale). 1 Organizational culture and organizational climate are the two key constructs of existing research on organizational social context, yet have very much lived separate lives within their own disciplines and traditions. 2 A work attitude is an individual-level construct that includes job satisfaction and organizational commitment, which together capture the morale of the workforce. 3 Our study describes the organizational social context in primary health care using organizational culture, organizational climate and work attitudes (morale).
Organizational social context is thought to be useful in explaining how organizations influence the behavior, attitudes and wellbeing of members, why some organizations are more innovative and quicker to adopt new technologies, and why some organizations are more successful than others. 1 So-called constructive organizational cultures have been found to promote and support innovation, whereas defensive cultures appear to hamper innovation. 4 Culture is also purported to be associated with climate. Defensive cultures seem to add to the probability of alienation, emotional exhaustion, work load and experienced disagreement; 1 however, Bosch et al. reported no associations between organizational culture, team climate and patient outcomes. 5
The delivery of health care services today therefore demands person-centeredness, flexibility, innovation, teamwork and a constructive organizational culture.
The recognition and assessment of organizational culture is particularly valuable in health care, as it addresses the therapeutic milieu, thereby creating the potential to maximize service, quality, and outcomes for both health care providers and the recipients of care. 6 Several studies suggest that organizations establish the social context for services, as organizational social contexts directly affect service quality and outcomes.1,7
Background
Organizational culture, climate and morale
In the literature we have numerous definitions of organizational culture and climate. Some studies reported that these two concepts are different, whilst some see them as more or less overlapping. 8 In this study the concepts organizational culture and organizational climate are held in clear contrast to each other: organizational culture being the way things are done in organizations, and organizational climate being the way members of organizations perceive and experience their work environment. 2 These are distinct constructs of the human services environment. According to Glisson and James, 1 a climate consisting of individual experiences is based on individuals and is a psychological attribute, whereas culture is clearly an attribute of an organization and thus an attribute of a system or collective.
Culture is defined as normative beliefs and shared behavioral expectations in an organizational unit. These beliefs and expectations prescribe the way work is approached and are the basis for socializing co-workers in the way things are done in the organization. Organizational culture captures expectations, and values what is important in a specific organization. These expectations and values are either implicitly or explicitly expressed in the behavior of fellow workers, and have the capacity to socialize members of the organizations who may seek to behave in ways that meet the expectations of their workplace. 7
Organizational climate is based on psychological climate. 9 Psychological climate is to some extent socially influenced by the collective social construction of acquired meanings of the work environment, which leads to the accommodation of one’s interpretive standards. It is plausible that especially when new ambiguous events are encountered, a need for discussing them arises. 10 The psychological climate experienced by members of the organization appears to be related to working attitudes (morale). 11 Work attitudes are measured by job satisfaction and organizational commitment, and together compose the morale of the service providers who work in the organization. 3 Patients can expect to be taken care of by a team which has a high morale. High worker morale has been associated with workplace stability, supportive managers and clear roles, while low morale has been associated with insufficient staffing levels, high levels of verbal abuse, risk of violence, and of workers feeling they have no voice in the workplace. 12
Looking broadly at worker morale, the literature links the type of work with job satisfaction 13 or with some level of organizational commitment.4,14 The literature also provides combinations of factors related to stress, 15 including turnover with worker burnout, resilience, and emotional exhaustion.13,16
Over the last decade, fewer studies have been interested in culture, climate or morale in primary health care. For example Rostila et al. conducted a study of social context in primary health care in Finland. 10 Although evidence for the possible relevance of teamwork and culture is growing, most evidence for these intuitively appealing concepts is based on studies in hospital settings. 5 Nowadays, primary health care is inconceivable as anything other than a competently functioning health care team, 17 and health care professionals are increasingly aware that interprofessional collaboration and effective team communication are essential for improved patient care and safety. 18
Internationally, both climate and culture have been shown to predict job satisfaction, organizational commitment and the voluntary turnover of employees in nursing and various types of caring work. In primary health care it has been noted that climate differs in regard to functionality and engagement, and differences were bigger in terms of climate than in terms of culture.1,10 Organizational climate and services have been seen to differ between child welfare service systems and this may explain the variance in service system outcomes. Systems with more engaged organizational climates had significantly better outcomes and fewer services to children were provided in stressful climates. 19
Culture and leadership were the most important factors in predicting climate in primary care teams. The lack of relationships found between most organizational factors and team climate suggests that interpersonal aspects of teamwork override organizational aspects, and that individuals who commit to working in this environment will engage in teamwork regardless of other environmental factors. 20 The association of organizational culture and climate with individual work attitudes (morale) may differ depending on the clinical context and between clinicians. 21
Primary health care
In health care, organizational changes are continuous. From the late 1990s, all countries in the Baltic region were trying to improve primary health care and implement reforms to rationalize their health care systems. The most intensive reforms were introduced in Estonia, Latvia, Lithuania, Poland, and also in some regions of Russia. 22 The main focuses of primary health care reform following Lithuanian independence were decentralization and strengthening interprofessional collaboration. 23 Following these reforms, the number of primary health care institutions markedly changed with the number of primary health care centres increasing 2.4 fold and private care sector increasing 34 fold. Such reorganization of primary health care systems, however, did not change work relationships. Lithuanian primary health care professionals continued to work in a traditional hierarchical relationship. 24
Aim
The aim of this study was to describe the social contexts (organizational culture, climate and morale) in primary health care centers from the viewpoint of health care professionals.
Methods
Instrument
The organizational social context (OSC) measurement system 1 was used to assess the key characteristics of culture, climate and morale. The questionnaire consisted of background factors and the OSC instrument. The background questions were demographic (age, gender, education, qualification and year of qualification), and work related (work experience in health care, in primary health care, and present organization, current position in organization, client groups worked with, and the specialized area in which they worked as a team member).
The OSC measurement system is guided by a model of social context that comprises both organizational (structure and culture) and individual (work attitudes and behavior) level constructs, including individual and shared perceptions (climate) that are believed to mediate the impact of the organization on the individual. 1 The OSC measurement system includes 105 items. 25 The instrument includes three dimensions: organizational culture (42 items), organizational climate (46 items) and morale (17 items). Culture is structured as rigidity (14 items: e.g. ‘I have to ask a supervisor or coordinator before I do almost anything’; ‘We usually work under the same circumstances day to day’), proficiency (15 items: e.g. ‘Members in my organization are expected to have up-to-date knowledge’; ‘Members in my organization are expected to act in the best interest of each client’) and resistance (13 items: e.g. ‘Members in my organization are expected to avoid being different’; ‘Members in my organization are expected to be stern and unyielding’). Rigid cultures allow service providers only a small amount of discretion or flexibility in their activities, with the majority of controls coming from strict bureaucratic rules and regulations. Proficient cultures place the health and wellbeing of each client first and service providers will be competent, working to meet the unique needs of individual clients with the most recent available knowledge. Resistant cultures are described as service providers showing little interest in change or in new ways of providing services and will suppress any change efforts with criticism and apathy. 26
Climate was measured by stress (20 items: e.g. ‘How often do your co-workers show signs of stress?’; ‘No matter how much I do, there is always more to be done’), engagement (11 items: e.g. ‘I can easily create a relaxed atmosphere with clients I serve’; ‘I have accomplished many worthwhile things in this job’) and functionality (15 items: e.g. ‘I understand how my performance will be evaluated’; ‘My job responsibilities are clearly defined’). Stressful climates are characterized by employee perceptions that they are emotionally exhausted by their work and are unable to accomplish the necessary tasks at hand. Engaged climates are characterized by employee perceptions that they are personally able to accomplish many worthwhile things and remain personally involved in their work and concerned about their clients. Functional climates are characterized by employee perceptions that they receive the cooperation and help they need from co-workers and administrators to do a good job, and that they have a clear understanding of how they fit in and can work successfully within the organization. 26
Morale (17 items: e.g. ‘I am willing to put in a great deal of effort in order to help this organization be successful’; ‘I find that my values and the organization’s values are very similar’) consisted of commitment to the organization and satisfaction with their job. These criteria include the morale of service providers, service quality, and service outcomes as represented by improvements in the wellbeing of service recipients. 26 A five-point Likert scale was used to assess the characteristics of culture, climate and morale, with a score of 1 meaning not at all and 5 to a very large extent.
The OSC was translated using back-translation. 27 During the translation process the translations of the instrument were discussed between the researcher, translators and specialists (nurse, psychologist, social worker, manager). A Lithuanian language teacher was consulted to confirm the validity of the translation. Before data collection, the questionnaire was piloted with four teams of health care professionals from three different health care centers in different counties than the one under investigation. In total, 59 health care professionals completed the pilot questionnaire. On the basis of the pilot test, some minor linguistic changes were made.
The instrument has been found to be reliable and valid in previous studies conducted in the US and Finland.10,25,28 In our study the Cronbach’s alpha values for culture were 0.86 (rigidity), 0.89 (proficiency) and 0.94 (resistance). For climate the values were 0.89 (stress), 0.91 (engagement) and 0.89 (functionality). For work attitudes (morale) the value was 0.88.
Data collection
The data were collected between August 2009 and January 2010 among all health care professionals from all state primary health care centers (18 organizations) of one purposefully selected county in Lithuania (N = 1096: nurses 579; physicians 316; other 201). Questionnaires were completed during working hours in 29 health professional team meetings, which were organized in conjunction with the researcher. The participants were informed about the confidentiality of information and they gave written consent. The questionnaire took about 25–30 minutes to complete. Individually completed questionnaires in sealed envelopes were returned to the researcher who was present during the data collection meeting.
Ethical approvals from the directors of primary health care centers were obtained and from the Ethical Committee of the Faculty of Health Sciences. The research addressed all ethical considerations. 29
Data analysis
The analysis was carried out using IBM SPSS Statistics version 21. Descriptive statistics were firstly calculated for all variables. An index of within-group consistency of responses and single-item rwg was computed for each of the four constructs that describe characteristics of the groups. rwg shows how members of the team agreed in evaluation of one or other component. If all group members are in perfect agreement, they assign the same rating to the target, and the observed variance is 0, rwg = 1. In contrast, when all group members are in total disagreement, the observed variance will asymptotically approach the error variance obtained from the theoretical null distribution and rwg = 0. 30 Values of 0.70 and over have been reported as indicating acceptance agreement among responses according to the instrument developers.1,3
Between-group differences were calculated using the intraclass correlation coefficient (ICC) and eta-squared. The ICC (type 1) computed via a random intercepts model indicates the proportion of total variance that is between groups, and eta-squared indicates the proportion of total variation or sums of squares that is between groups. Hierarchical cluster analysis cluster methods (Ward’s squared Euclidean distance) were used for culture and climate profile grouping.
Results
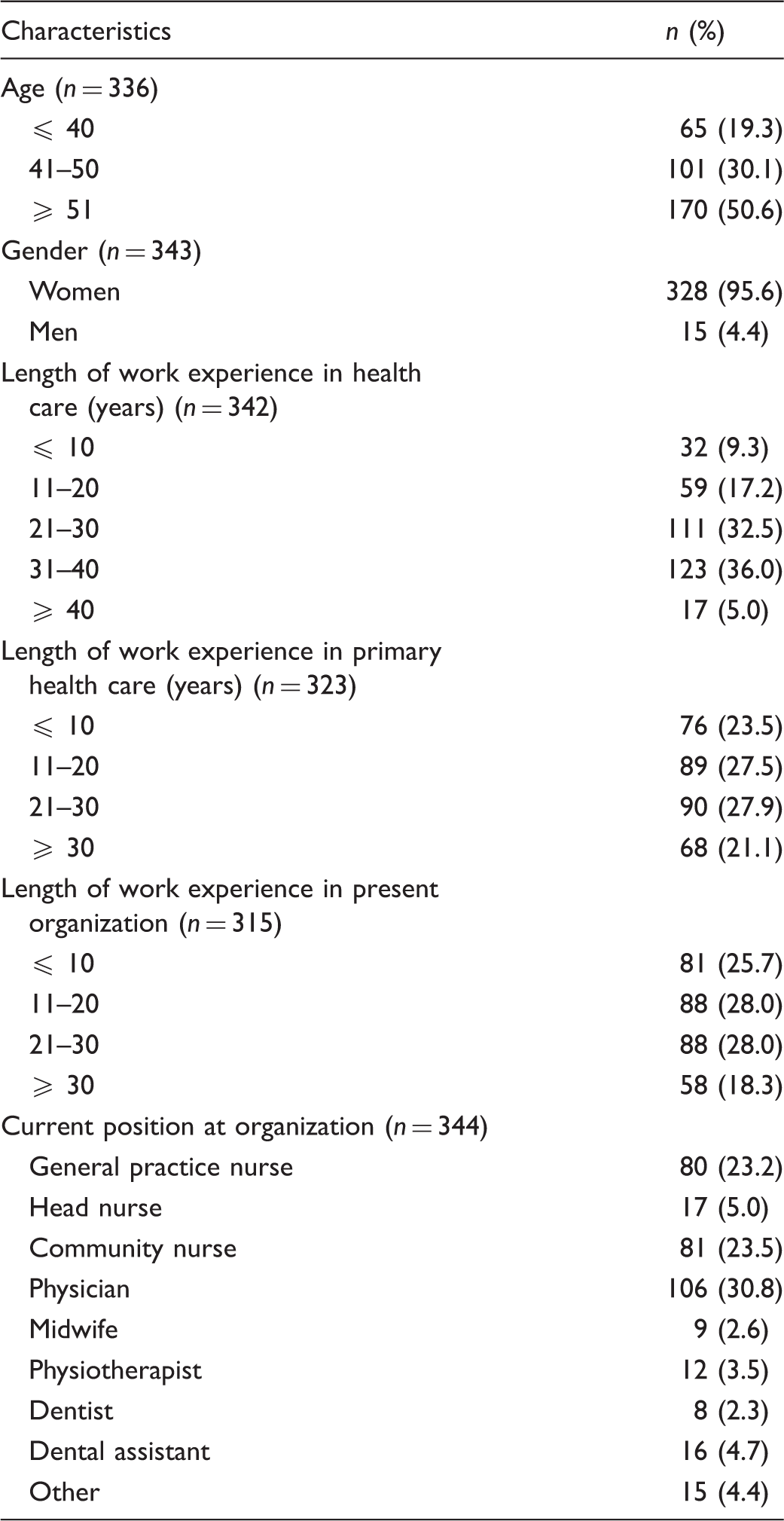
Demographic characteristics of respondents (n = 344).
The estimates of rwg at both team and organization levels were clearly above the critical value of 0.70. Within teams (within organizations), the estimates varied for rigidity between 0.70 and 0.97 (0.72–0.97), for proficiency between 0.71 and 0.98 (same), for resistance between 0.86 and 0.98 (same), for stress between 0.75 and 0.99 (0.76–0.99), for engagement between 0.80 and 0.99 (0.84–0.96), for functionality 0.69 and 0.98 (0.82–0.98), and morale 0.81 and 0.94 (0.83–0.94). These estimates of agreement indicate the existence of a team and organization level climate and culture, and justify using the means of individual level measurements of culture and climate as measures of group level culture and climate.
Differences of organizational culture, climate and morale between and within the teams and organizations (n = 344).
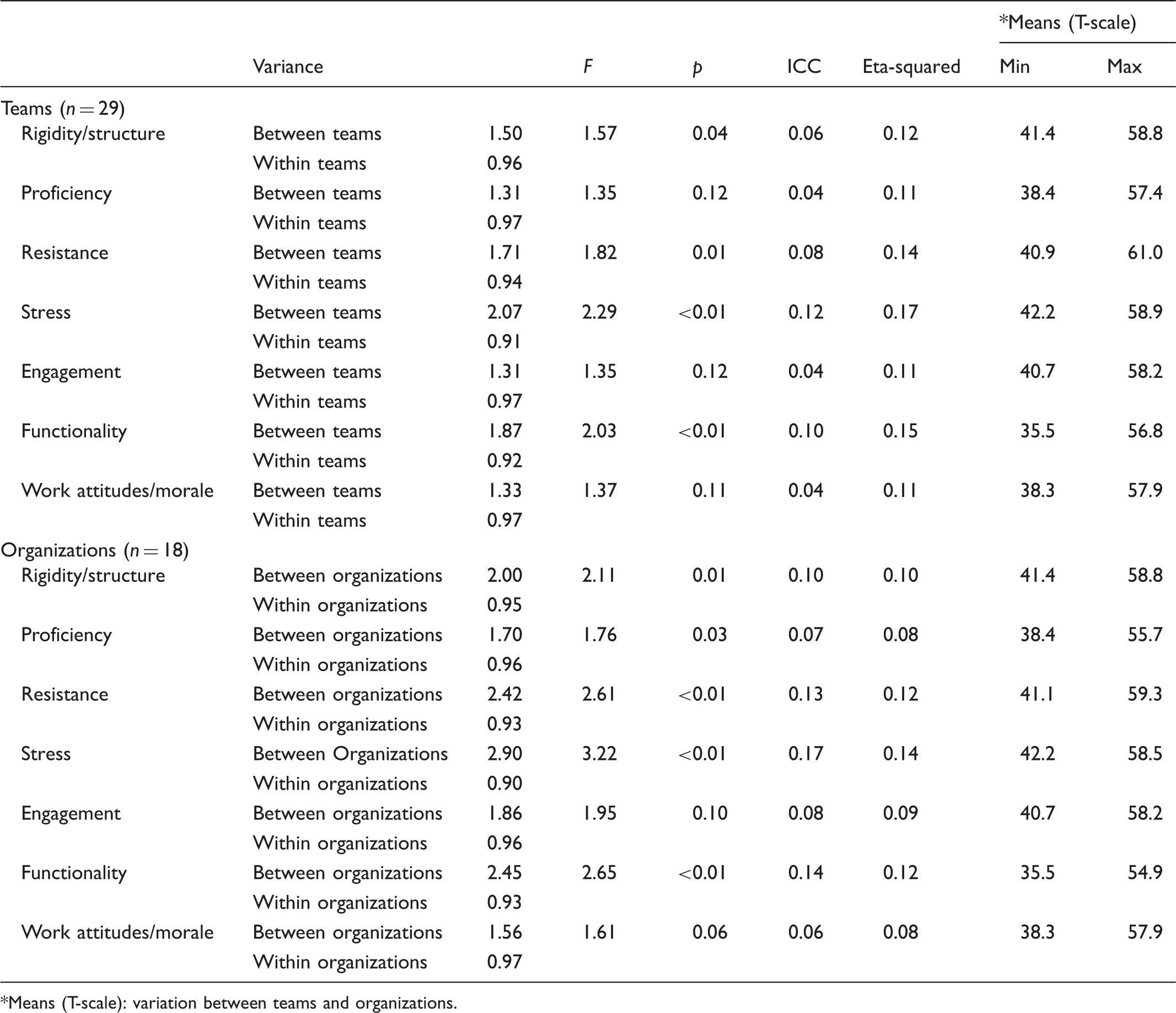
Means (T-scale): variation between teams and organizations.
The differences between teams were significant in culture rigidity (structure) and resistance. Significant variations were also found at the upper organization level in the same dimensions, and further variance in proficiency was also significant. There was most variation in culture proficiency and rigidity at team and organization level.
Based on team level background factors, it was found that the culture was more rigid the older the team members were (r = 0.59, p < 0.01), the longer the length of work experience in health care (r = 0.65, p < 0.01), the longer their length of work in the present organization (r = 0.43, p < 0.05) and the more resistant was the culture (r = 0.41, p < 0.05). Related to organizational level background factors, no statistically significant results were found.
Climate differs between team and organization levels concerning stress and functionality. Similar results were found within team and organization levels, the variation being largest in engagement. Based on the team level and organizational level background factors, no statistically significant results were found related to climate dimensions.
Differences in variations in climate were bigger than those seen in culture between teams and organizations. Resistance and functionality differed most at both team and organization levels. The culture and climate profiles varied among the teams. Data is presented using T-scale (mean 50, standard deviation – 10). Examples of these are presented in Figure 1 and Figure 2.
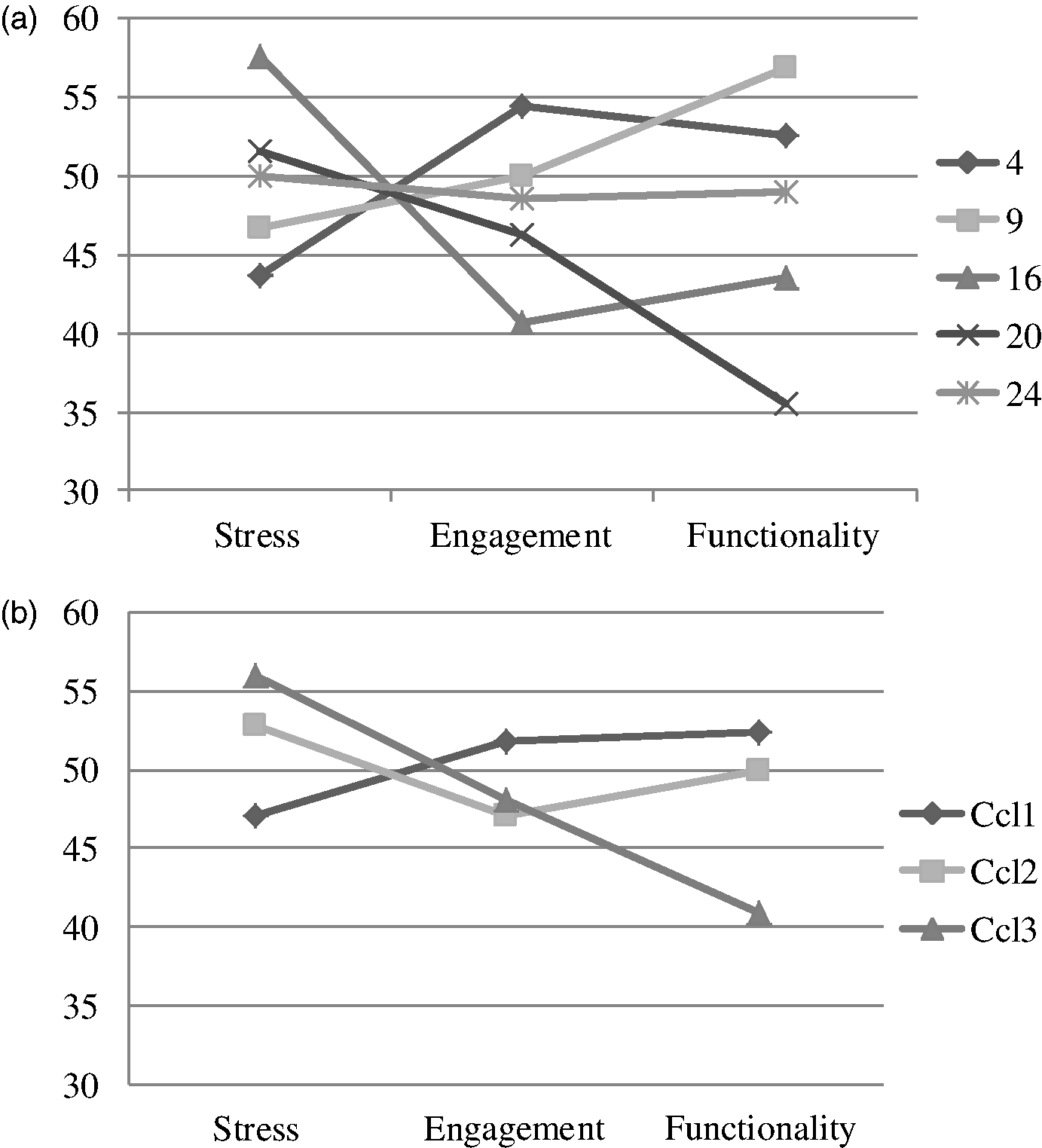
Examples of culture profiles from primary health care centers and different clusters between teams (n = 29). (a) examples of culture profiles, (b) culture profiles grouped into four clusters. Examples of climate profiles from primary health care centers and different clusters between teams (n = 29). (a) examples of climate profiles, (b) climate profiles grouped into three clusters.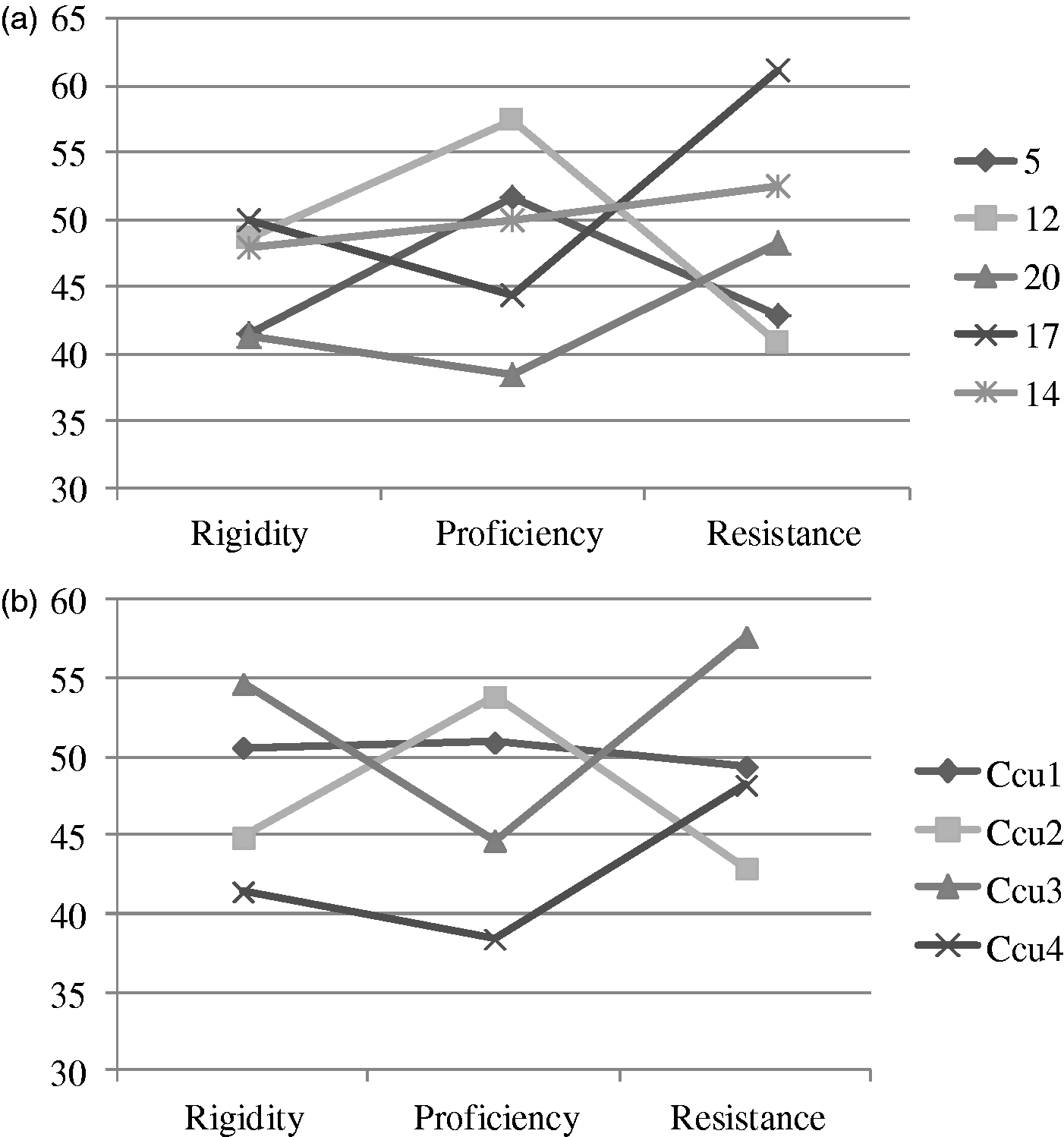
In Figure 1a, when comparing culture profiles with other teams, team number five is characterized by relatively low (compared with a sample average) ‘rigidity’, medium ‘proficiency’ and low ‘resistance’. Team number 17 however, shows medium ‘rigidity’, low ‘proficiency’ and high ‘resistance’. The culture profiles can also be grouped into four different clusters. It seems that one profile represents the profile with a moderate level of culture dimensions while the other profiles show variation between low, moderate and high levels of different culture dimensions (Figure 1b). Age, and length of work experience in health care, primary care, and in present organization all were statistically significantly (p < 0.001) related to the different culture profiles.
Comparing the examples of climate profiles: team number 20 is characterized by high ‘stress’, medium ‘engagement’ and relatively low (compared with a sample average) ‘functionality’. Team four, however, shows low ‘stress’, high ‘engagement’ and high ‘functionality’ (Figure 2a). The climate profiles can be grouped into three different clusters. One profile clearly shows the connection of high stress to low functionality. The other team profiles do not show the same kind of clear relationship of stress with other climate dimensions (Figure 2b). Lengths of work experience in primary health care were connected (p < 0.005) with the climate clusters and as well the length of work experience in the organization (p < 0.001). About 7% of the variance in work morale was seen in teams and organizations. Based on the background factors at team and organizational level, no statistically significant results were found.
Discussion
This study describes the social contexts in primary health centres in the Baltic country of Lithuania. Evaluating the study results we can state that different organizational culture, climate and morale exist at both organizational and team levels. This has been seldom previously reported in the European primary health care context. 10 Differences between teams, however, have been reported in several studies.3,11,25
Based on our results, variation between teams was seen in terms of rigidity and resistance. Additionally, however, Rostila et al. 10 found a variation in terms of proficiency that was not found in our study. Our results show that when the average age of team members was greater, with longer work experience in health care and longer work experience in their present organization, a more rigid culture was found. Glisson 26 has described rigid culture as a culture which allows service providers only a small amount of discretion or flexibility in their activities, with the majority of control coming from strict bureaucratic rules and regulations. It can be explained that the implementation of health care reform in Lithuania has not changed the traditional relationships between health care professionals as quickly as expected. As Jaruseviciene et al. 24 have stated, community nurses (who are the biggest group of primary health care professionals) mainly continued acting as physicians’ assistants and continued to work in a traditional hierarchical relationship with general practitioners.
Climate differences we found at both team and organizational level concerning stress, but in the Finnish context 10 this was only at the organizational level. As in a previous study, 10 climate was found to differ also in terms of functionality at team and organizational level. Engagement variation among Lithuanian primary health care teams was considerable at both the organizational and team levels – a result which has not been previously noted. 10 Climate stress variation at group level has, however, been reported in other studies in public health 10 and also in hospitals. 28 Climate difference concerning functionality was also seen in the results of a study by Rostila et al. 10 where they investigated the social context in public health and social services.
It was interesting to find that variation levels were larger in climate than culture (measuring the way things are done in the organizations), 2 as has also been noted for example in Finland. What does this reveal? Is it perhaps that organizational norms and values may not be influenced by recent developments as much as climate in various countries and cultural contexts? Hierarchical management systems may maintain the stability of cultural dimensions. If we want to manage the primary health process holistically, then we need less rigid cultures. This presents quite a challenge to managers, bearing in mind that many teams in this study were quite old and had worked in primary health care and in their present organizations for quite a long time.
Differences in variations in climate were larger than in culture between teams and organizations, and functionality differed most heavily at team and organization level. Rostila et al. 10 found that differences in functionality were of approximately equal size in home aid and health care at organizational level (about a quarter of the variance of perceptions of functionality).
The psychological climate experienced by members of the organization appears to be related to working attitudes (morale). 11 Morale consisted of a commitment to the organization and satisfaction with the job. These criteria include the morale of service providers, service quality, and service outcomes as represented by improvements in the wellbeing of those who receive the services. 26 Variation in work morale was about 7% in the teams and organizations in this study, and Rostila et al. 10 have previously reported that about 8% of the variance in work morale was associated with the work unit. Glisson et al. 25 stated that less rigid and more proficient cultures were associated with higher clinician morale, but that resistant cultures were not associated with morale. Also, more functional climates were positively associated with higher health care worker morale, but stressful climates were not associated with morale. 11
More knowledge is needed regarding the social context (and its implications) of the primary health care setting, as many changes have taken place in regard to service structures, technology, client choice, service enterprises etc. The contribution of management in this context also calls for further exploration. To achieve this, in-depth research is required to identify models that might explain the functionality of the service system. This is important to contribute knowledge for quality purposes, and also to benefit the health service system and its patients, especially in regard to safety.
Some methodological considerations of this study should be addressed. The instrument used in this research has been previously found to be reliable, and to offer a valid measurement of the organizational social context. The instrument was piloted in the Lithuanian context. To guarantee an equal provision of information for participants, the researcher personally organized the group meetings, informed the participants about the study verbally and with written information, and collected the resultant data. While all of the health care professionals in the studied sites were asked to participate, a limitation exists in that some teams had fewer participants. However, the criteria for using the instrument were fulfilled. The requirement is to have a minimum of six group members in a team, and only primary health care centres with more than six health care professionals were involved in this study. 1 A total of 29 teams participated, and the number of members in each team varied between 6 and 24.
Conclusions
The issue of how we handle the increasing economic challenges in health care is central to the success of primary health care. One core element is how the workplace’s social context supports us in achieving the best possible outcomes from the viewpoint of clients, workers and the organization. It is important to determine whether there are obstacles in this social context which hinder our best possible performance, and unnecessarily cause a situation where clients need to seek help from services other than primary health care.
Managers should recognize different kinds of social context among teams to enable them to co-work efficiently in evidence-based primary care settings. Whether the culture is resistant or constructive in a certain unit, managers need to use different implementation strategies, e.g. when supporting the use of a new electronic recording system, or when deciding whether some changes in the tasks shared between nurses and physicians are needed. The largest variation, which was in engagement, urges the managers to evaluate their subordinate groups’ engagement while it is obvious not all teams gain the same outcomes in their work.
In primary health care it is especially important to support those teams in which the average age is quite high and who have a long work experience in the present organization. It is really challenging to the managers to support the teams to keep their enthusiasm to work. Thus we may consider rotating staff. With a stable staff situation, it is challenging to create an innovative culture and supportive climate. One challenge for the future may therefore be how to best integrate new staff members into these teams, keeping in mind that staff recruitment is generally difficult across the whole health care sector.
Cultural and climate differences among the teams and organizations of primary health care raise a challenge for managers looking for new ways to organize and support their workers. The culture may have mechanisms in place that are not being perceived (climate) as working or effective. In future we should consider more culture and climate relations to received outcomes.
Footnotes
Author contributions
NG, TS, PA and IR conceived and designed the study. NG and SB performed data collection and analysis. NG, TS and PA drafted the manuscript. TS, PA, PG and IR critically reviewed the paper for important intellectual contents. All authors read and approved the manuscript.
Acknowledgements
We would like to thank Mika Helminen for the statistical advice and the health care professionals of 18 primary health care centers who kindly agreed to participate in the study.
Funding
The study has been partly funded by Pirkanmaa Hospital District (EVO 9N074), Satakunta Hospital District (EVO 81041) and Finnish Cultural Foundation.
Conflict of interest
The authors declare that there is no conflict of interest.