
Abstract
Chronically ill populations have a strong need for quality public health nutrition services to aid in disease management and improve health outcomes. Evidence suggests that neglecting the importance of adequate nutrition in chronically ill patients has far-reaching implications on the health status of the individual and the health care costs. Research is currently lacking a focus on this topic. This pilot study done through the nonprofit organization MANNA (Metropolitan Area Neighborhood Nutrition Alliance), which serves the greater Philadelphia area, explored the health care expenditures of 65 MANNA clients over time in comparison with a similar group of Medicaid patients who did not receive MANNA services. Health care expenditures were examined before and after clients began receiving services. The study found that the mean monthly health care costs decreased for three consecutive months after initiation of MANNA services. Other health care cost–related factors, such as inpatient costs, length of stay, and number of hospital admissions also displayed a downward trend. These results help show the significance of medical nutrition therapy and home-delivered meal services on overall health care.
Introduction
Quality public health nutrition services, including access to healthy meals and nutrition education are needed by all individuals. However, the need for these services is even greater for individuals who are chronically ill, which can aid in disease management and improve health outcomes. Individuals battling chronic illnesses benefit from public health nutritional services, both in the form of education and food support. Studies and research now generally recognize that nutritional support of patients with acute and chronic illnesses can improve quality of life, the ability to withstand medical regimens, and perhaps even quantity of life. 1(p25) Previous studies also provide evidence that suggests that neglecting the importance of adequate nutrition in chronically ill patients has far reaching implications on the health status of the individual as well as the overall cost of health care. 2(p61) The Academy of Nutrition and Dietetics, formerly the American Dietetic Association, stresses the importance of medical nutrition therapy (MNT) in improving the health of the general population and studies have linked MNT to improved health and cost outcomes. The cost of caring for chronically ill populations, especially those in the later stages of disease, has been estimated to cost the American economy more than $1 trillion annually. 3(p1) However, there is a lack of literature examining the outcomes related to provisions of home meal delivery, education, and counseling for this population. There also are no current studies that examine the relationship between the provision of medically appropriate meals with MNT and health care costs. Improved health care cost outcomes are of extreme importance, especially following the recent economic crisis. Those most affected by this are populations with the highest nutrition requirements, including chronically ill populations. For individuals who are low income or have other difficulties accessing healthy food, medically tailored, home-delivered meals programs could be a viable solution. Organizations, such as the Metropolitan Area Neighborhood Nutrition Alliance (MANNA) work to bridge the gap between food access, medical nutrition therapy, and improved health outcomes for chronically ill populations.
MANNA History and Pilot Study Objectives
MANNA is a nonprofit, nonsectarian, volunteer-intensive organization that serves clients in the greater Philadelphia and Southern New Jersey area who are at acute nutritional risk and battling any life-threatening illness. Although socioeconomic status is not a factor in receiving services, a significant proportion of MANNA clients are Medicaid eligible. MANNA provides each client 3 nutritionally balanced meals a day, 7 days a week, free of charge. Meals can also be modified to accommodate various dietary restrictions and cultural preferences. MANNA’s registered dietitians provide MNT to the clients and offer support through nutrition counseling and meal planning. MANNA’s goal is to improve our clients’ nutritional status, strengthen their ability to fight their disease, and improve their quality of life. Reducing overall health care costs in theory should be a result of the mission to improve health.
The objective of this pilot study was to compare the MANNA program’s outcome in lowering the overall cost of health care in individuals battling chronic diseases, including HIV/AIDS, renal disease, and various forms of cancer. The pilot study examined in detail 2 questions: (a) Does provision of MANNA services correlate with reduced expenditures, emergency room visits, and hospital admissions? (b) Do MANNA patients have lower health care costs and/or better health outcomes than patients with similar medical conditions who are not receiving MANNA services?
Materials and Methods
Population Demographics
The population represented in the study strongly reflected the demographics of the overall MANNA client population at the time of the study with 63% African Americans and 29% Caucasians. The gender distribution was slightly higher with females than are usually served by MANNA. The average age of a MANNA client is 61 years whereas the average age of the study participants was slightly younger at 52 years. The average annual income of current MANNA clients, based on those who reported income levels is $10 188. This income level is slightly lower than the 100% poverty income level of $11 170. 4(p1) It should be emphasized that MANNA serves people based on their medical condition and acute nutritional risk factors; socioeconomic status is not factored into eligibility.
The MANNA client group and the comparison group were well matched on gender, age, race, and ethnicity. Both groups were predominantly African American and almost entirely non-Hispanic. The average age of both groups was 52 years. Table 1 provides a summary of the demographics and Table 2 provides a summary of chronic diseases and nutritional illnesses of the MANNA clients and the comparison group, which further supports the similarities between the 2 groups.
Demographic Characteristics of Study Participants (August 2007 to December 2010).

Number of Study Participants with Charlson Indexed Chronic Illnesses or Nutritional Diseases as Coded in Medicaid Managed Care Organization Health Claims (August 2007 to December 2010).

Sample Selection
Two sample groups, the MANNA client group and a comparison group, were obtained. MANNA clients were screened for eligibility according to whether or not they had received services between August 1, 2008 and April 30, 2010 for at least 3 months without interruption and were also members of a local Medicaid managed care organization (MCO). The study was completed during this time frame because the 21 meals per week program began in July 2008. The MANNA group consisted of 65 clients who had any health care claims at a hospital, clinic, or skilled nursing facility during the designated time period. Based on the client demographics diagnosis codes on their health claims, which were categorized through the Charlson Comorbidity Index (CCI), a comparison group was selected. The comparison group was further narrowed to match 8 nutrition-related diagnosis codes. This was an essential step since MANNA clients are screened for nutritional risk for eligibility in the meal delivery program. The comparison group was determined through logarithmic regression and, from this, 633 comparison members were identified.
Analytic Frameworks
A descriptive analysis first examined the characteristics of both the MANNA clients and the comparison group which included demographics, CCI diagnosis codes and nutrition diagnosis codes. An analysis examined the cost patterns of MANNA clients pre- and postservice. Outcomes were evaluated on a monthly basis and included overall health care costs, health care costs for emergency room visits and health care costs for hospital admissions. Since there was a large percentage of an HIV/AIDS client in the MANNA group, this subset was also looked at and published separately. An analysis between MANNA clients and the comparison group was also conducted. The outcomes examined included overall health care costs and health care costs for emergency room visits and cost as well as admissions, length of inpatient stay, and cost. Another noted difference among the two groups, which was not among the original research questions, was the number of patients discharged to home. Analyses were conducted using SAS version 9.3.
Results
Pre- and Post-MANNA Services Analysis
Comparing overall health care costs in the 12 month time frame that was examined showed a significant decrease in costs among all MANNA clients. A significant decrease in costs also was observed in the 3 months following the initiation of MANNA services. Among all MANNA clients, the average monthly costs dropped from $38 937 to $28 183. This is depicted in Figure 1. Average monthly inpatient costs for all MANNA clients decreased as well, with a significant drop observed during the first 3 months following the initiation of MANNA services from $174 320/month to $121 777/month. This is depicted in Figure 2. Average monthly emergency room costs were also examined, but the findings were inconclusive.

Average monthly health care costs of all MANNA clients 6 months prior to service and 6 months after beginning service (August 2007 to December 2010).
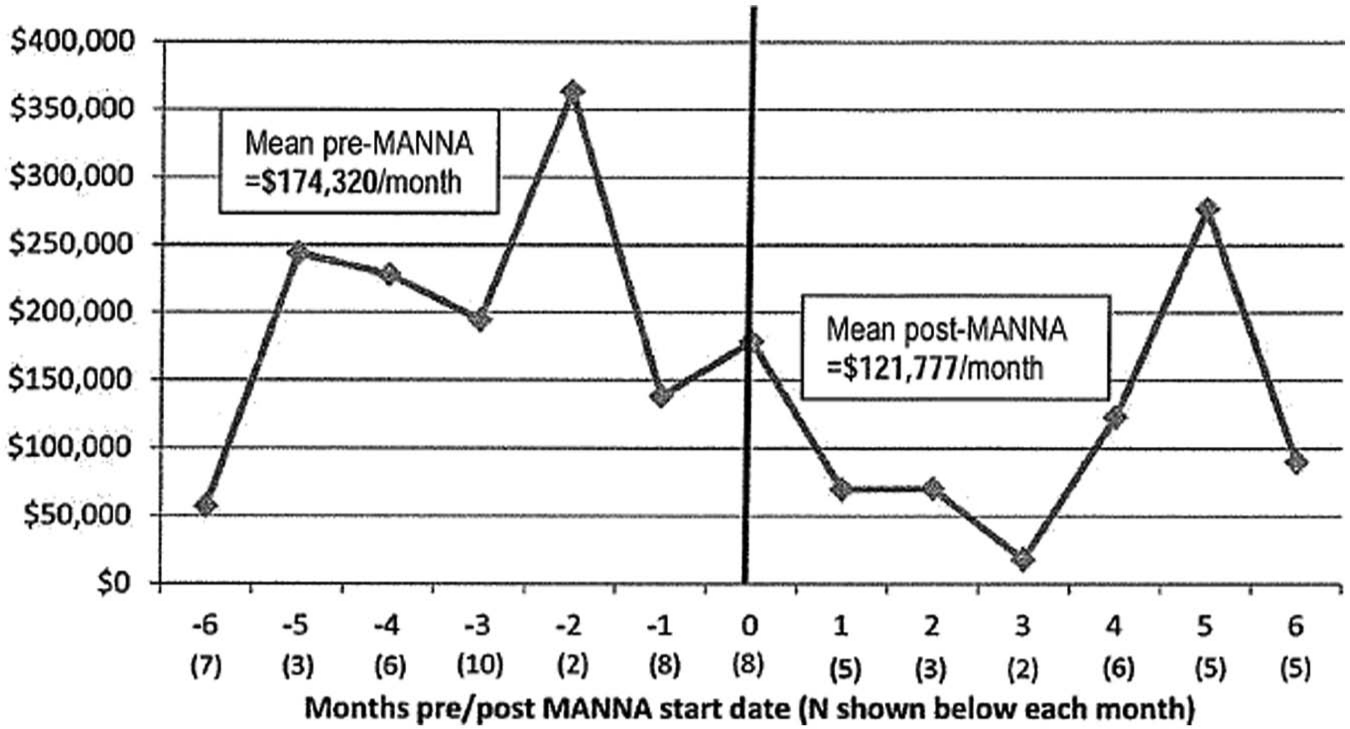
Average monthly inpatient hospital costs of MANNA clients 6 months prior to service and 6 months after beginning service (August 2007 to December 2010).
Comparison Group Analysis
In examining the total health care costs for both groups, the result showed a decrease in costs for the MANNA client group except for emergency room visits, which were inconclusive. The total average monthly cost was $28 000 for MANNA clients versus $41 000 for the comparison group, a difference of 55% which is statistically significant. It had a calculated P value of less than .05.
The cost and frequency of hospital admissions and length of stays were all significantly lower in the MANNA client group versus the comparison group. The overall costs associated with these findings were also lower on average at $132 000 in the MANNA client group versus $220 000 in the comparison group. The average number of inpatient visits was lower and the length of stay was shorter. A key finding was that, on average, in the 12 months following the start of MANNA services, 93% of clients with inpatient hospitalizations were discharged to their homes as opposed to 72% of the comparison group who were discharged to an acute care facility. Table 3 depicts these results. The results that were calculated to be statistically significant are denoted and all had P values less than .05.
Mean Monthly Visit and Costs for MANNA Clients (After Starting MANNA services) and the Comparison Group.

Difference between MANNA clients and comparison group is significant at P < .05.
Again, emergency room costs were researched, but the results were inconclusive.
Discussion
The findings of this study provided statistically significant evidence that critically ill and nutritionally at-risk individuals served by MANNA experienced lower health care costs. This occurred both in comparison with costs before initiating MANNA services and with costs of a comparison group of individuals who did not receive the services. This was observed in 3 of the 4 pre- and post-MANNA service analyses; monthly health care costs for all MANNA clients, clients with HIV/AIDS, and inpatient hospitalization costs. Average monthly health care costs of the MANNA client group overall was 28% lower in the 6 months following initiation of MANNA services compared with the 6 months prior to beginning services. It should also be noted that at no time during the 6 months following the initiation of MANNA services did the monthly health care costs reach the levels they were in during the 6 months prior to initiation of services. The average monthly health care costs were 31% lower in the MANNA client group versus the comparison group. This indicates that nutritional services had a significant impact on the overall health care costs of those individuals.
Another key finding was in relation to the average number and length of stay for inpatient hospital visits. Not only was the length of stay 37% shorter for the MANNA client group but also the number of admissions was half that of the comparison group. After their discharge, the MANNA clients group was 23% more likely to be discharged to their homes rather than to a long-term care or subacute rehabilitation facility than the comparison group. The results showed having access to the nutritional food and MNT services provided by MANNA helps reduce the incidence of being discharged to a more costly facility. This not only represents a lower financial burden to the health care system but also suggests that their health is more stable on discharge.
The findings of this study are consistent with prior research showing that nutrition is an integral part of disease management. Chronically ill patients with several comorbid conditions have complicated nutritional needs that may be challenging for patients or their caretakers to adhere to without additional support. MANNA’s nutritional services provide continued support to those individuals to help nourish the client back to health. Home meal delivery with MNT allows for chronically ill individuals to maintain a healthy body weight, withstand side effects of treatments, improve immune function, and enhance their overall quality of life. These associations correlate with lowered overall health care costs that would be associated with the care for their chronic illness.
Limitations
There are some limitations that are present with this pilot study, which includes the sample size of MANNA clients, identification of the comparison group, lack of background information pertaining to the comparison group, and the overall timeline in which the outcomes of the study was examined. When factoring in the number of patients who had submitted health claims with the participating MCO, the client base at MANNA during the time of the study was quite small although still robust enough for a pilot study. Although the sample size was large enough to provide statistically significant findings for the comparison analyses, it was small for the pre- and post-MANNA service analyses. Having a larger client sample size would help improve the external validity of the pre- and post-MANNA service analyses.
When identifying the comparison group, a very large initial population was examined to find individuals who were comparably as sick as the MANNA clients. Since criteria for MANNA’s meal service mandates clients are at nutritional risk, it was essential to include nutritional diagnosis codes. Adding the nutritional component to the consideration did skew the chronic disease prevalence. This may have resulted in a bias in favor of higher costs and utilization among some in the comparison group. Since the differences existed only among those who had more than 4 chronic illnesses, the relative percentages were small and there were no differences in the proportion of those with nutritional diagnosis codes. Thus, we believe that this bias was minimal.
Since the MCO only provided aggregate data, matching could not be done in an ideal one-to-one manner.
Also because only aggregate data was provided by the MCO for the comparison group, there was little knowledge of the comparison groups’ social service support. Some in the comparison group may have been receiving other food support or nutritional services at the time of the study. This limitation may have affected the differences in costs and utilization between the 2 groups. However, since MANNA is the only service in the area that provides 21 medically appropriate meals and MNT, it is likely that any additional food support for the control group addressed the issue of food security with little attention to improvement in health. These results are specifically examining the costs of health care in relation to a medically appropriate meals program and not general food resources. Further research is needed to study this potential bias in the comparison.
The timeline of this study was 12 months for the MANNA client group. Not all MANNA clients received services for the entire 6 months that the pre- and post-MANNA analysis covered. Longer timelines could provide additional information about the efficacy of a nutritional program such as MANNA’s and demonstrate stronger correlations between long-term health care costs and utilizations of a nutritional program. Having more subjects and following their progress longer could also help MANNA clarify optimal service duration periods for reducing health care costs.
Future Goals
Based on the findings of this pilot study, it is the goal of MANNA to expand the study to address the limitations mentioned. Expansion of the study will allow for more external validity in application of the findings. One possibility includes expanding the potential partnerships with insurance and medical care providers that exist outside of the Medicaid populations. Expansion of the study would allow for more external validity in application of the findings. As the Affordable Care Act is implemented, there will be an emphasis on quality of care and use of community-based interventions to improve health. We believe that investigating the importance of programs that address optimizing nutrient needs for chronically ill patients should be acknowledged as an essential cost-effective intervention for improving health.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Jill Gurvey was working for OMG who MANNA hired to analyze the data during the research. The research was done as part of her employment with no other financial incentives. None of the other authors were involved in the subject selection or data analysis but all were employees of MANNA when they authored the submission as part of their employment or internship.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies