
Abstract
Objective
A busy primary care practice staffed mostly by residents faces difficulties providing coordinated care that is consistent over time. 1 These challenges often result in patients becoming “lost to follow-up.” In an effort to improve the quality of patient care, the clinic seeks to adopt a medical home practice model.However, as in many clinics with limited resources, implementing this practice model presents several challenges, including poor continuity of care, coordination of care, and follow-up.
The ambulatory intensive care unit (ambulatory ICU) provides close follow-up of a patient with high needs resulting from comorbidities, lack of support or understanding, or a history of non-adherence to treatment. As a result, the primary care provider (PCP) is kept closely informed of a patient’s progress and is able to more quickly respond to changes in health status, and the nurse providing the care is able to establish a relationship with the patient that goes beyond the medical problem focus to help drive health improvement by focusing on holistic care. The nurse can also facilitate meetings with social workers to help with housing or transportation issues, and with a pharmacist to help with medication understanding, changes, and ways to improve adherence, all with the objective of improving the patient’s overall health and access to health care.
The goal of this quality improvement project was to use the ambulatory ICU to improve the quality and continuity of care by implementing an intensive nursing approach in a team-based collaboration to follow vulnerable and often complex patients. Providers refer patients they identify as needing extra assistance in the primary care setting, and many of these patients face a combination of health challenges, including chronic illness, acute illness, and adherence issues. In collaboration with a PCP and any providers who see the patient on an acute basis, this care model more closely monitors and updates a patient’s progress, providing him or her with a time-sensitive response to his or her health issues. In addition to providing better care for the patient in this way, the system allows the provider more satisfaction in the ability to enhance communication with and provide better outcomes for the patient. Using the electronic health record, members of the entire collaborative team are able to interact with each other to keep one another informed, and the ambulatory ICU nurse takes the lead in overseeing that continued communication between the patient and provider and determining when the relationship can recede into a less intense focus after patient and provider goals have been met. Patient goals were identified and modified over the course of the implementation as the project became better defined by the patients’ needs.
Methods
Study Design
This report includes data from a quota sample of the first 100 patients referred into the program (see sample characteristics in Table 1). Providers referred patients they felt would benefit from more intensive follow-up contact with the project nurse, particularly if the provider’s own schedules did not permit frequent follow-up in clinic. Referred patients included those without a PCP, those needing extra education on medication or disease processes, those needing reminders about specialty appointments, those patients who were seen in the urgent care clinic with an acute condition to follow improvement, and those with a history of frequent ED usage or poor adherence to health improvement strategies, including medication management. Patients who were already enrolled in an automated randomized Medicare trial (a Care Management Program, or “CMP”) were automatically excluded. Referrals came from faculty and residents who were PCP, urgent care providers, or covering providers.
Demographics of Patient Population

Intervention
The project created an ambulatory ICU into which residents and faculty in the primary care clinic could refer patients that they identified as at risk for hospitalization, inappropriate ED use, being lost to follow-up through the patient’s lack of adherence or the provider’s schedule prohibiting personal follow-up, or exacerbation of an acute or chronic medical condition. The structure of the ambulatory ICU comprised 3 nurses, the referring provider, and the PCP.
After a provider referred a patient to the ambulatory ICU, the nurse reviewed the patient’s medical record and collaborated with the referring provider to identify short-term goals. These goals included monitoring blood sugar and uptitrating insulin, monitoring medication usage for new or maintenance medications, reminding a patient to schedule a specialty appointment, calling a patient to update on the status of labs, following up symptoms after an acute episode, or educating a patient on his or her chronic illness (ie, hypertension, asthma, diabetes), among others. As the study had rolling admission based on referrals from providers, each patient’s improvement over time was calculated based on the amount of time that he or she spent in the ambulatory ICU. If the patient was monitored in the ambulatory ICU for 2 months, the 2 months prior to entry were considered for improvement calculations. The time periods ranged from 1 month to 8 months. Patient goals were classified as (1) assignment of a new PCP, (2) adherence issues (pharmaceutical or specialist referral), or (3) health issue follow-up, including managing chronic diseases such as diabetes, hypertension, and asthma. The nurse maintained this communication with the patient on a weekly basis for as long as necessary, ranging from 1 week to several months, at the nurse’s discretion. The nurse also updated the patient’s electronic health record and corresponded with the referring provider and PCP in order to identify resources or special needs as well as to update the provider on the patient’s ongoing health status. To qualify as successfully meeting goals, patients being assigned a new PCP needed to keep their initial appointment with the new provider in the clinic. Successful adherence included reporting taking medication as directed, including picking it up from the pharmacy, or making and keeping specialist referral appointments. Improvement in health status for chronic conditions was qualified by a sustained decrease in blood glucose readings, or a decrease in blood pressure—that remained down—of at least 10 mm Hg systolic.
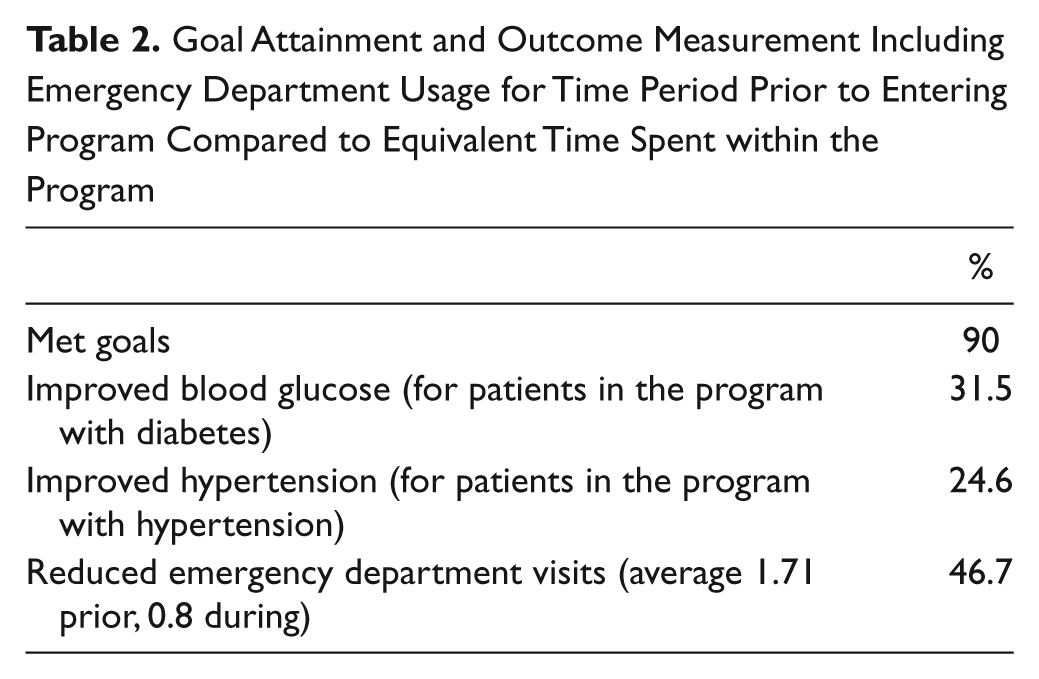
Goal Attainment and Outcome Measurement Including Emergency Department Usage for Time Period Prior to Entering Program Compared to Equivalent Time Spent within the Program
Main Outcome Measures
The primary outcome measure was meeting graduation criteria established at enrollment in the program. Secondary outcomes included improvements in blood glucose or blood pressure values, as well as frequency of ED visits within the hospital network and an increase in making and keeping specialist appointments. These measures were meant to give an overview as to the success of the intervention: decreasing inappropriate use of the ED, better management of chronic diseases as evidenced by improving vital signs, and increased adherence regarding specialty office visits.

Workflow chart
Results and Level of Statistical Significance
Ninety percent of patients met their goals for graduation from the ambulatory ICU. Twenty-four percent of patients kept an appointment with a new PCP, 35% made or kept appointments with specialists or successfully transitioned into a new medication regimen or taper, and 39% were followed for an acute health situation that resolved to the provider’s satisfaction (ie, follow up of infection or resolution of symptoms/side effects).
For those patients being followed for diabetes improvement, finger stick glucose measurements were tracked for the period before entering the ambulatory ICU equivalent to the time spent in the ambulatory ICU. Twelve patients, or 31.5% of those being followed for diabetes, showed an improvement consisting of a general and consistent trend downward. Sixteen patients, or 24.6% of those being followed for hypertension, showed a sustained improvement of at least 10 mm Hg systolic readings in the clinic.
The number of emergency room visits was similarly calculated according the amount of time that the patient had spent in the ambulatory ICU, with number of visits to any emergency department in the hospital network logged in the electronic health record or any records that were faxed to the clinic from ED outside the network. The average number of emergency room visits was roughly halved, from 1.71 visits per person to 0.8 visits per person.
The use of specialists was another metric used, as many patients had poor adherence to following up with specialist appointments. This measure showed a slight improvement, a 1.04% increase in the number of specialist appointments kept after entering the ambulatory ICU compared to the equivalent time period before entry.
Conclusions
The program did have a net benefit in reducing ED usage by a significant percentage as well as some improvement in diabetes and hypertension management. Patients largely met their goals as determined by their providers, and anecdotally, patients and providers both were very pleased with the program and the outcomes. The program could benefit from continued improvement, such as having more defined values as objectives from the outset, and more definition around whether an objective had been met in order to measure success. As the program grows, more procedures are being implemented to standardize the referral process as well as the outcome measurement. The program is also being expanded to include social workers, resource counselors, and a PharmD to best meet patient needs.
Limitations
Limitations of the data collection include the fact that the collection and analysis was performed by the same person, who designed and implemented the program. Because each patient was different and had different goals in the program, outcomes were difficult to standardize and measure. Consequently, metrics were instituted after the study to evaluate for goal attainment, reduction in number of ED visits, increase in keeping specialist appointments, reduction in blood pressure if managing hypertension, and reduction in blood glucose if managing diabetes. The study is therefore limited by definitions of significant change, by exacerbations of disease and seasonal illnesses, and by incomplete patient notes in the electronic charting system showing glucose and blood pressure values. Also, it is worth noting that appropriate ED usage versus inappropriate ED usage is not deducted from these calculations, and more in depth analysis of each patient’s records might give more information into the effectiveness of the program. Finally, the initial 35 patients referred into the program were patients at high risk who were transferring from a resident leaving the clinic to a new PCP rather than those identified with a specific need, so outcomes were based only on whether the patient kept an appointment with a new PCP rather than other values. Additionally, two patients enrolled in the program passed away during the intervention period after meeting their goals.
As the program transitions from being run by one part-time nurse to two full-time staff nurses who will dedicate a portion of their time to following patients in the program, there are issues that need to be resolved around streamlining and sharing efforts, as well as data management issues for a multi-user environment. There was a consistent effort throughout the initial phase to market to and educate referring providers about the program and the most appropriate patients for referral. There was also a slight redundancy of effort in patients who were randomly referred to the CMP for Medicare patients over the course of this trial. Efforts to make the program sustainable were important from the initial undertaking and were therefore prioritized.
Discussion
In the recent past, strategies to improve continuity of patient care have included developing the Patient-Centered Medical Home (PCMH) and the Chronic Care Model (CCM). This clinic sought to achieve the PCMH by optimizing the team-based approach of the CCM with provider collaboration and intensive RN follow up.
The PCMH, as defined by the American Academy of Family Physicians, is a model to improve the quality of healthcare for patients while also reducing costs by centralizing one source (the medical home) for the patient’s medical record and coordination. 2 The PCMH emphasizes a PCP as the central coordinator for a patient.That provider takes the lead to make referrals to specialists and to follow up on those results. A PCMH is also focused on the patient as a whole person, coordinating all care for that patient through the PCP, improving quality and safety of care while enhancing access to care for the patient.3,4
The CCM is a team-based approach to following patients with long-term management needs for chronic illnesses such as hypertension and diabetes. The CCM model differs from the PCMH in focusing particularly on long-term management rather than clinic operations and information sharing. 5 Despite this difference in focus, both models are intended to improve patient outcomes and to reduce the costs of providing quality patient care. 6
This project used the team-based approach of the CCM but also meets some of the goals of the PCMH, namely, improving coordination and access of care through one PCP and focusing on the whole patient by (1) communicating with patients after a visit to reinforce teaching, communicate labs, verify understanding of medication usage, ensure adherence with medication usage/confirm ability to obtain medication, and coordinate specialty care visits; (2) titrating or changing dosage of a medication as needed; and (3) communicating patient concerns to a provider in a timely manner to foster a dialogue about the patient’s health priorities and concerns during a transition or acute health status change. Closing this loop of communication helps to reduce ED visits and fosters communication and collaboration between the patient and the provider as well as improves the quality of health care by increasing the amount of contact. 7 Timeliness of follow-up has been shown to improve patient outcomes. 8 Delivering low-cost telephone care for follow-up is not only cost effective but has been shown to be more clinically effective in some trials, as it improves convenience and accessibility for the patient.9,10 The program reported in this study was an initiative by the clinic to improve clinical quality and patient experience, two of the structural capacities required by Medicare to enhance payments. 11
Addressing this clinic’s concern—to reduce the cost of providing health care with many patients receiving capitated care while receiving broken care provided from many different sources including the ED—was key to this study.Although dollar amounts were not captured by the project, use reflects a general savings to the health care system, even if the clinic itself does not benefit. Ultimately, savings to the health care network, improvements in quality and consistency of care, and improved patient and provider satisfaction were achievable goals that were measured by the project.
The passage of the Patient Protection and Affordable Care Act of 2010 supports the development of the Accountable Care Organization (ACO), which promotes provider led organizations with a strong primary care base that are accountable for quality and costs across their patient population. The ACO is linked to quality improvement and reducing overall costs, as well as reliable and increasingly sophisticated performance measures. Developing the Accountable Care Organization in conjunction with the PCMH helps move payments from volume focused to value oriented. 12 This project, based in a primary care setting and initially funded by a small grant but transitioned to existing staff at no extra cost, shows that an effectively cost-neutral investment in time spent with intensive nursing follow-up does reduce costs to the health care system by reducing the number of ED visits while improving patient outcomes in both acute and chronic conditions, or simply by keeping them connected to a PCP when they are at risk of being lost to follow-up.
Ultimately, the benefits to each patient are visible in the 90% of patients achieving their goals. The clinic has higher satisfaction for both patients and providers, measurable improvement in outcomes, and a sustainable way to continue to move toward a PCMH. Identifying those patients who have the highest cost burden with comorbidities, poor adherence, and inappropriate use of resources targets the inefficiencies inherent in a large health care system and drives savings from the bottom up. Staff members at this clinic are very satisfied with the program and are looking forward to continued improvement of delivery of high-quality, low-cost health care to the most vulnerable patients.
Footnotes
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) received no financial support for the research, authorship, and/or publication of this article.