
Abstract
Introduction
Collaborative care management (CCM) for the treatment of depression has been shown to be an effective therapy for improving clinical outcomes.1,2 CCM incorporates key components of evidence-based models for chronic illness care. These components are the community, the health system, self-management support, delivery system design, decision support, and clinical information systems. 3 Although some studies have demonstrated that there can be long-term demonstration of cost-effectiveness,4,5 CCM can be seen as a resource-intensive treatment. Ideally, resource utilization would not be expended for those who are going to improve with minimal intervention. Likewise, continued care for a population that will not improve despite CCM would also be considered a waste of resources. In the later scenario, early identification of these patients who would not be effectively treated with CCM could allow for alteration of their therapy or change in modality.
Recently, the combination of 3 patient self-assessment tools and the clinical diagnosis (of either first episode of depression or recurrent episode) allowed for the development of a model to predict persistent depressive symptoms 6 months after enrollment into CCM. 6 The patients at highest risk were those with severe anxiety symptoms, abnormal screening on the Mood Disorders Questionnaire (MDQ) 7 and severe, recurrent depression. The patients at lowest risk for persistent depressive symptoms were those without anxiety symptoms, a negative MDQ and moderate, first episode of depression. The probability rates ranged from 42.1% to 6.6%. The CCM used in this study involved a registered nurse as a care manager with weekly case review by a consulting psychiatrist supported by a depression registry.
A previous pilot study on Patient Health Questionnaire–9 (PHQ-9) 8 scores over a 6-month time frame for those patients who did improve demonstrated that there was a rapid decrease over the first month or two after enrollment in the PHQ-9 scores. 9 Patients who were more severely depressed improved the most, with all patients regardless of initial depression severity, scoring at a 5 to 6 by the first month after treatment initiation. An emerging trend in this study suggested that there may be characteristics that distinguish between those who may improve quickly, and those who may benefit from CCM, thus using resources more efficiently.
As the STAR*D trial demonstrated, a significant quality indicator for depression care is the improved clinical outcomes of remission.10-12 Other potential quality indicators could be decreased time in treatment and decreased treatment failures compared with usual care. Using a database of patients enrolled into CCM, we used a case-controlled mechanism to study those patients who did not benefit from CCM and after a year of treatment were transitioned to another type of care. The hypothesis was that by studying the epidemiology of patients in prolonged care management (PCM), characteristics could be used to help define this group.
Methods
Primary care patients from our multisite practice have been able to be enrolled in collaborative care management for depression since March 2008. Eligibility criteria for CCM enrollment was a clinical diagnosis of major depression or dysthymia and a PHQ-9 score ≥10. Once the clinician decided to activate the patient into CCM, the patient met with a care manager for the intake process. This involved a mental health history (diagnoses, prior treatments, and medications), further patient self-assessment with Generalized Anxiety Disorder Questionnaire (GAD-7) 13 , MDQ, and the Alcohol Use Disorders Identification Test (AUDIT). 14 Our CCM was part of a statewide initiative (Minnesota) that began in 2008 and the enrollment data collected was designed to be consistent at all sites. 15 The care manager met with the consulting psychiatrist weekly to review new patients as well as any enrolled patients with concerns. All recommendations for treatment (medication or therapy) were reviewed with the primary care provider. Those patients who improved and were in remission were to have a “relapse prevention” session with the care manager prior to conclusion of services. Patients who had persistent symptoms for more than a year after enrollment were transitioned out of the program, as they were not improving from the services. Our CCM program has been described in greater detail in prior articles.16,17
By March 2012, 2921 patients have been enrolled in CCM at our sites. Of this group, 132 patients were transitioned out of the program after being enrolled for more than 1 year. They will comprise the case group for this study. A random selection of 396 of the 714 patients who had achieved remission (PHQ-9 score <5) by 6 months were the control group (control to case ratio 3:1). The independent variables studied included age, gender, marital status (married or not), race, clinical diagnosis, baseline PHQ-9, GAD-7, AUDIT, and MDQ scores, and insurance coverage. After initial enrollment, the determination of number of face to face care management visits and the PHQ-9 score over time (at 10 and 26 weeks) were also evaluated. The dependent variable was case status (PCM >1 year vs. remission at 6 months).
Since the continuous variables were not in a normal distribution, Mann–Whitney testing was used for statistical analysis. Categorical data were analyzed with χ2 testing. Analysis of covariance was used to determine a baseline, 10-week, and 26-week PHQ-9 score for both the controls and the cases, while controlling for the other independent variables. Logistic regression modeling was performed while retaining all independent variables studied. Calculations were performed on MedCalc software (http://www.medcalc.org, version 12.3.0.0). This study was reviewed by our institutional review board.
Results
Table 1 demonstrates the univariate comparisons of the case and control groups. The control group was significantly more likely to be married (61.1% vs 49.2%, P = .022), with their first episode of depression (56.1% vs 46.2%) rather than dysthymia (6.1% vs 11.4%, P = .048), and less severe depression as measured by the initial PHQ-9 (<.001 for both average score and category of severity) than the cases. Although there was no difference in the percentage of hazardous drinking noted by a score of ≥8 on the AUDIT (P = .382), the control group did have a higher average AUDIT score (3.3 vs 2.3, P < .001). Age, gender, race, and insurance coverage along with initial GAD-7 score and MDQ scoring were not significantly different between the groups.
Comparison of Patients With Persistent Depression in Care Management at 1 Year, Versus Those in Remission at 6 Months, by Variable.
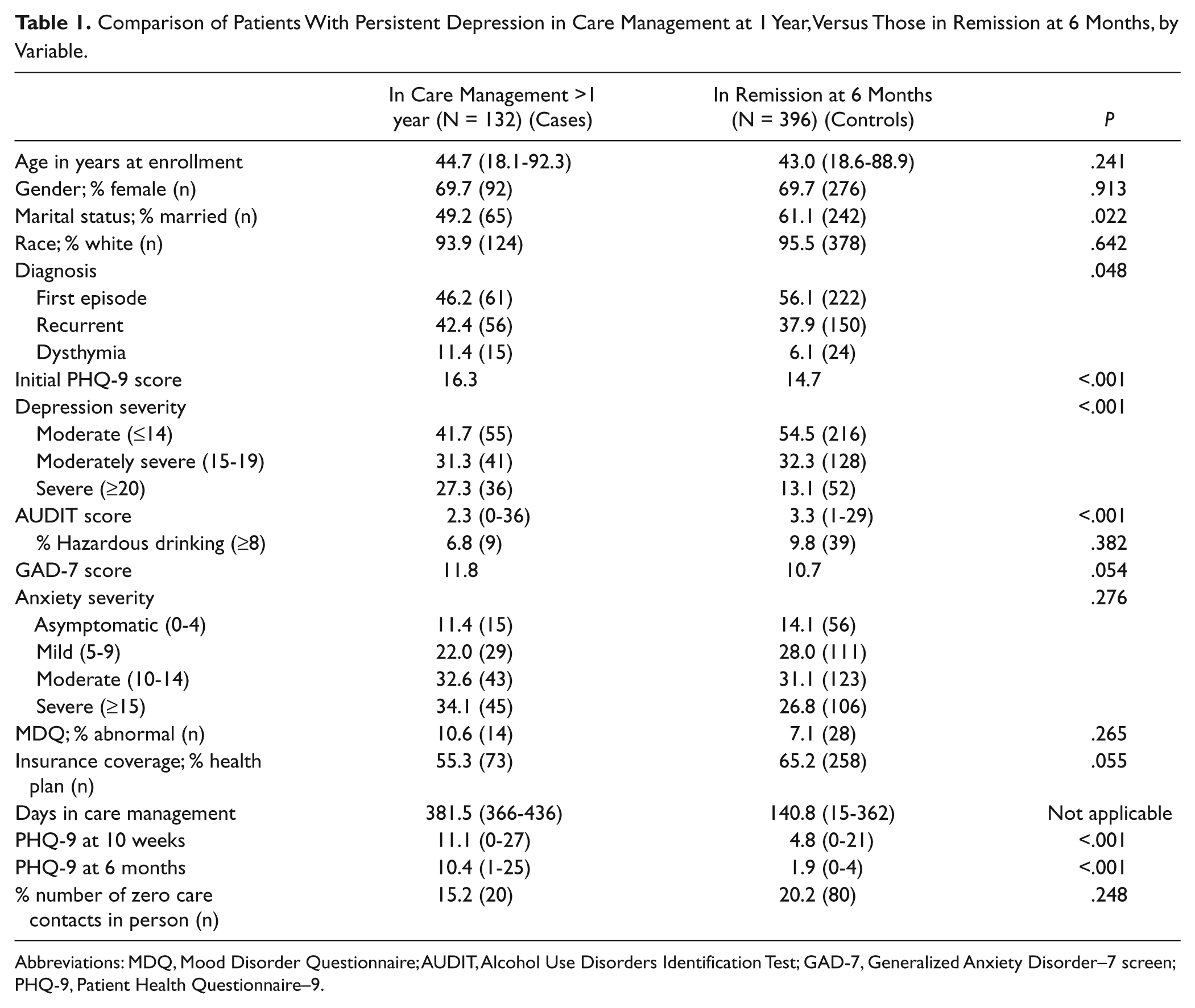
Abbreviations: MDQ, Mood Disorder Questionnaire; AUDIT, Alcohol Use Disorders Identification Test; GAD-7, Generalized Anxiety Disorder–7 screen; PHQ-9, Patient Health Questionnaire–9.
There was no difference between the case and control groups on the percentage of patients that did not have a face to face care management visit (15.2% vs 20.2%, P = .248). As expected, there were large differences noted in the 10-week (11.1 vs 4.8, P < .001) and 26-week (10.4 vs 1.9, P < .001) PHQ-9 scores (cases vs controls, respectively).
With regression modeling, the odds of a patient in this study having PCM at 1 year (case) was highly significant for those unmarried patients (odds ratio [OR] = 1.736, confidence interval [CI] = 1.115-2.703, P = .015) with dysthymia (OR = 2.362, CI = 1.104-5.052, P = .027) and severe depression (OR = 2.856, CI = 1.551-5.260, P = .001), when controlling for all the other independent variables. Age, gender, race, insurance coverage and intake GAD-7 and MDQ scores were not independent risks factors for PCM at 1 year. An increased AUDIT score at baseline was inversely associated with the risk of being in the case group (OR = 0.891, CI = 0.823-0.965, P = .005; Table 2).
Odds Ratio of Persistent Depression After 1 Year in Collaborative Care Management, Logistic Regression Modeling With All Independent Variables (N = 528).

Abbreviations: MDQ, Mood Disorder Questionnaire; AUDIT, Alcohol Use Disorders Identification Test; GAD-7, Generalized Anxiety Disorder–7 screen; PHQ-9, Patient Health Questionnaire–9.
By using analysis of covariance with all the independent variables, the adjusted baseline PHQ-9 was 16.0 for the cases versus 14.8 for the controls (P < .001). By 10 weeks, the difference was much larger (10.7 vs 4.9, P < .001). At 26 weeks, the control group by study definition was <5, with an average PHQ-9 score of 2.0, whereas the case group was still elevated at 10.2 (P < .001; Figure 1). While controlling for all predictor variables, the cases had an adjusted PHQ-9 score that was higher than the control group at baseline and this difference increased over time. By normalizing the 10- and 26-week PHQ-9 scores to the baseline scores, at 10 weeks, the case group was 70.3% of baseline and the control group 26.7% (P < .001) and at 26 weeks, the case group was still 63.6% of baseline and the control group 13.3% (P < .001). The mean PHQ-9 for those in the case group at 1 year was 8.6.

Adjusted Patient Health Questionnaire–9 (PHQ-9) scores at baseline, 10 weeks, and 26 weeks, by groups.
Discussion
The variables found in this epidemiological case–control approach that independently correlate to an increased odds ratio of PCM include unmarried status, severe depression, and the diagnosis of dysthymia. Prior studies by our group that have focused on outcomes at 6 months have found that anxiety, depression severity, and clinical diagnosis have been the significant predictive variables.6,16,18,19 Using the case–control study approach allowed for the inclusion and study of the diagnosis of dysthymia, which had been previously difficult to evaluate using other methods because of the relatively smaller numbers of patients with that diagnosis in our CCM program.
Although these 3 independent variables suggest an increased risk of prolonged depression symptoms despite one year of CCM, they do not by themselves allow sufficient clinical discernment at the onset of CCM. At the initial assessment, differentiating treatment plans for an unmarried patient with severe dysthymia may not be possible. However, taken in conjunction with the additional information of the PHQ-9 results over time could help differentiate these groups. If the above patient has a baseline PHQ-9 score of 21, a follow-up PHQ-9 of 18 at 10 weeks, and a score of 16 at 6 months, there should be a high likelihood that this patient would have been in PCM at 1 year after enrollment. Consideration certainly could be given to altering therapy or reassessing diagnostic options at 6 months instead of waiting another 6 months for them to “fail” CCM prior to acting.
Collaborative care management patients initially were planned to meet face to face with a care manager at least once during the intake evaluation. During expansion of the CCM process from one to five sites, there were times when the care manager and patients would not meet directly. This caused concern that the patients who did not start CCM with a face to face meeting would have worse clinical outcomes. In this case–controlled methodology, this was not noted be an issue.
The somewhat “protective” nature of increased alcohol use was unexpected. Prior retrospective reviews at our clinical sites have not previously demonstrated this as either a positive or a negative predictor variable6,16,18,19 of the AUDIT score with depression outcomes at 6 months. Though the association was statistically significant, the clinical significance of this finding is unclear. Mean AUDIT scores were low in both groups with a difference of only one point between groups. Additionally, there was no difference in the amount of hazardous drinking between the groups. This increased AUDIT scores in the patients with remission at 6 months compared with those with PCM deserves further study.
Although the case–control study design allowed for the analysis of a relatively rare event (prolonged CCM for more than 1 year), the control group selection may confound the associations determined as other possible confounding variables were not studied. Limitations of the lack of diversity in gender and race as well as the study design with a population from one large primary care clinic may decrease the ability to generalize our findings to other practices.
Conclusions
Case-controlled analysis of patients in collaborative care management for depression for more than 1 year was compared with a randomized sample of patients who achieved remission by 6 months. Although there were clinical variables that were independent predictors of prolonged CCM (such as unmarried status, diagnosis of dysthymia or severe depression), the results did not provide sufficient clarity to suggest changes in clinical practice at enrollment into CCM. However, the trend of the patient’s PHQ-9 score over time in CCM may allow differentiation between groups sooner than 1 year.
Footnotes
Acknowledgements
Ms Julie Maxson and Mr Isaac Johnson assisted with data collection and registry management.
Declaration of Conflicting Interests
The author(s) declared following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Angstman has a consulting agreement with Tamber Health. Tamber Health was not involved in study design, data analysis or manuscript preparation. The other co-authors have no potential conflicts of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article:
Funding was from Department of Family Medicine, Mayo Clinic Rochester.