
Abstract
Obesity and depression are often comorbid conditions. There appears to be a bidirectional relationship between these. Obesity at baseline has been shown to increase the risk of onset of depression and depression at baseline increased the odds for developing obesity. Less is understood about the impact of obesity on depression treatment outcomes. The authors’ hypothesis was that obesity (body mass index [BMI] ≥30 kg/m2) and morbid obesity (BMI ≥ 40 kg/m2) would each have negative effects on depression remission rates after 6 months of enrollment into collaborative care management for depression. In a retrospective analysis of 1111 depressed patients with a PHQ-9 (Patient Health Questionnaire) score of 10 or greater, multivariate analysis for the odds ratio of achieving remission at 6 months demonstrated that the patient’s BMI at baseline was not an independent risk factor for depression outcome at 6 months. Collaborative care management for depression has been shown to be effective for improving depression outcomes, yet minimal prior research has focused on other clinical comorbidities that might affect outcomes. Although obesity was common in the study population, it was reassuring, based on this study that 6-month depression treatment outcomes do not appear to be significantly affected by the patient’s baseline BMI.
Introduction
Clinical factors such as comorbid anxiety and the severity level of depression have been shown to significantly influence response to collaborative care management (CCM) of patients with major depression1,2 (also K. B. Angstman, MS, MD, et al, unpublished data, 2012). Obesity and depression are often comorbid conditions 3 ; the incidence of depression in obese women is as high as 25%. 4 Patients with depression have higher attrition rates in weight loss programs 5 and worse outcomes, including less weight loss. 6 A meta-analysis of 15 studies (N = 58 745) of obesity and major depression demonstrated a bidirectional relationship. 7 Obesity at baseline increased the risk of onset of depression (unadjusted odds ratio [OR] = 1.55) and depression at baseline increased the odds for developing obesity (OR = 1.58).
Less is understood about the impact of obesity on the outcomes of depression treatment. In 2005, an 8-week fluoxetine trial for 369 outpatients with major depressive disorder showed that increased weight was associated with increased risk for fluoxetine resistance. 8 A 5-week study of 408 patients hospitalized with major depressive disorder demonstrated a slower and overall diminished response in patients with obesity compared with patients with a normal body mass index (BMI). 9 It may be hypothesized that obesity would negatively affect treatment response.
In a 2006 meta-analysis of 37 randomized controlled studies with 12 355 patients, CCM was found to have significant improvements in clinical outcomes at 6 months compared with usual care. 10 Quality metrics for depression outcomes in Minnesota focus on clinical remission at 6 and 12 months. 11 Thus, prior studies on this patient population have been on the clinical outcomes 6 months after enrollment into CCM1,2 (also K. B. Angstman, MS, MD, et al, unpublished data, 2012).
The purpose of this study was to evaluate the impact of baseline BMI at the time of enrollment into CCM on depression outcomes, while controlling for other clinical variables. Our hypothesis was that initial obesity (BMI ≥ 30 kg/m2) and morbid obesity (BMI ≥ 40 kg/m2) would each have negative effects on depression remission rates after 6 months of enrollment into CCM.
Methods
The development and utilization of the collaborative care model in our institution have been reviewed previously.12,13 CCM was initially implemented at 1 of 4 primary care sites in March 2008, a second site added in September 2008 and the 2 remaining clinical sites on March 2010. Approximately 100 000 adult patients are cared for by these primary care practices. When a provider diagnosed a patient with major depression or dysthymia and the initial Patient Health Questionnaire–9 (PHQ-9) 14 score was 10 or greater, the patient was given the option of enrolling into CCM. Patients with a diagnosis of bipolar disorder (not just an abnormal Mood Disorder Questionnaire (MDQ) 15 were excluded from CCM, but those with other psychiatric comorbidities such as generalized anxiety disorder (screened by the Generalized Anxiety Disorder Scale–7 [GAD-7]) 16 or alcoholism (using the Alcohol Use Disorders Identification Test [AUDIT] 17 ) were not included.
This retrospective chart review study included patients enrolled into CCM from March 1, 2008 through June 30, 2011, allowing for 6 months of follow-up data through December 30, 2011. Since pregnancy (101 patients) and bariatric surgery (4 patients) have large physiological changes in BMI, these patients were excluded from the study, as were those who declined to give authorization for clinical research.
The dependent variable was the treatment outcome of symptomatic remission as measured with the 6-month PHQ-9 score (PHQ-9 score <5). The independent variables were age, gender, race, marital status, clinical diagnosis, initial screen scores (PHQ-9, GAD-7, AUDIT, MDQ) and BMI. BMI was calculated from the electronic medical record by using a weight within ±30 days and a height within 2 years prior to or 6 months after enrollment into CCM. All other data were obtained from a CCM database. Statistical analysis was performed by MedCalc software (version 12.2.1.0, http://www.medcalc.org). Chi-square analysis was used for categorical variables and one-way analysis of variance was used to compare the means across the groups of continual variables. This study was approved by the institutional review board.
Results
In all, 1947 patients were diagnosed with major depressive disorder or dysthymia in these primary care practices during the study time period and chose to be enrolled in the CCM process. Of these patients, 81.5% (1587) had BMI data available and only 27.4% (435) were of a normal BMI (BMI ≥15 and <25 kg/m2), whereas 44.7% (710) were obese (BMI ≥ 30 kg/m2). Of the obese patients, 10.4% (165) were noted to have a BMI of ≥40 kg/m2 (morbidly obese). At enrollment, patients with a normal BMI were younger and were more likely unmarried women with their first episode of depression (Table 1). Although statistically significant differences in intake scores (GAD-7 and AUDIT) were seen, these were not clinically apparent differences. Compliance (measured as 6-month follow-up PHQ-9 completion) and clinical outcomes (remission rates at 6 months) were not statistically different between the groups.
Enrollment Data Into Collaborative Care Management for Depression by BMI.
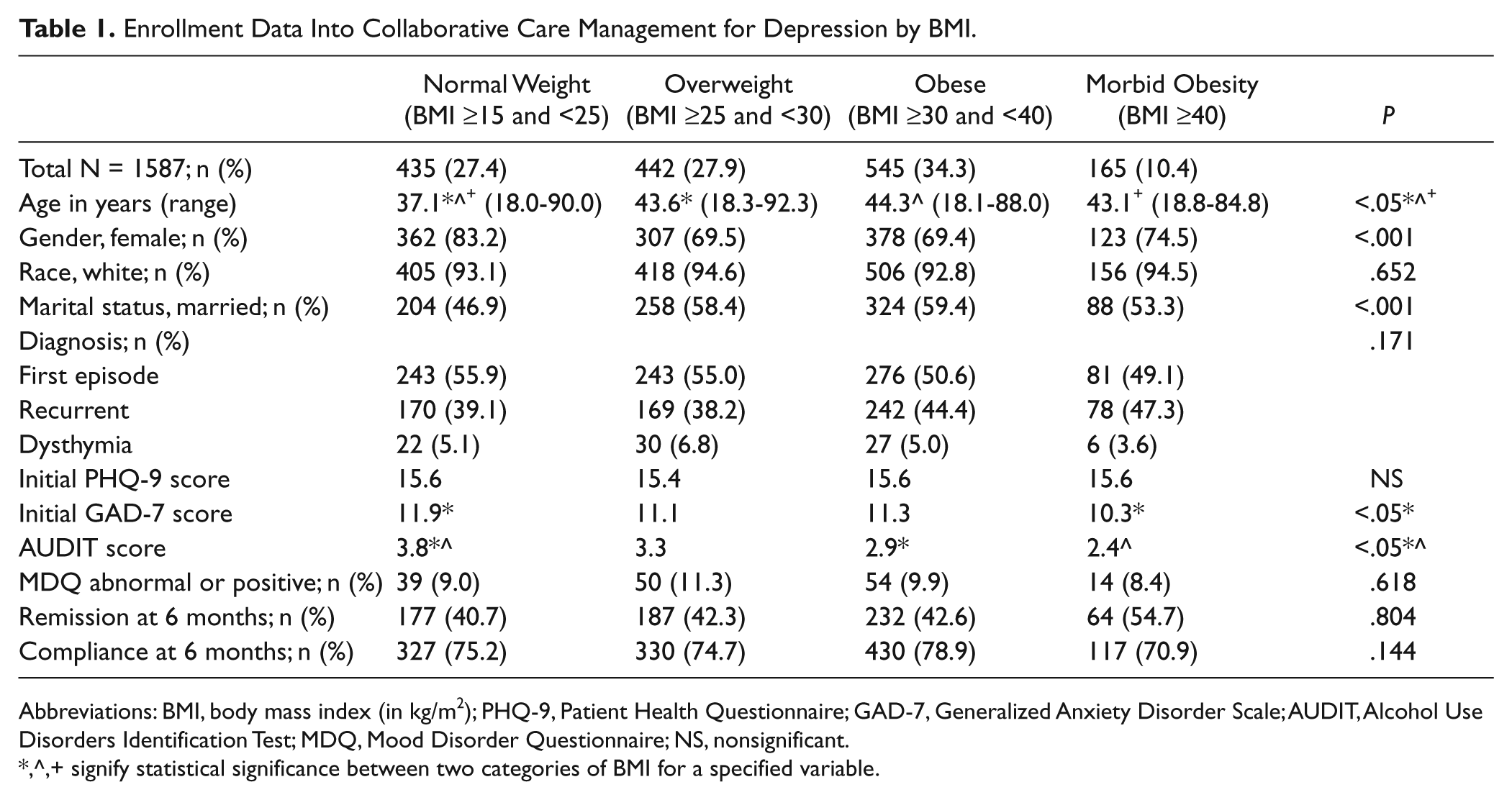
Abbreviations: BMI, body mass index (in kg/m2); PHQ-9, Patient Health Questionnaire; GAD-7, Generalized Anxiety Disorder Scale; AUDIT, Alcohol Use Disorders Identification Test; MDQ, Mood Disorder Questionnaire; NS, nonsignificant.
signify statistical significance between two categories of BMI for a specified variable.
For the evaluation of outcomes at 6 months, Table 2 demonstrates the percentages of patients categorized by their initial BMI and corresponding treatment response rate based on PHQ-9 scores defined as being in remission (PHQ-9 score <5), mildly symptomatic (PHQ-9 score 5-9), or having persistent depressive symptoms (PHQ-9 score ≥10). There were no statistically significant differences in all 3 outcomes between the groups with respect to the patient’s baseline BMI. Obese patients were not less likely to remit or have persistent depressive symptoms at 6 months compared with those with normal BMI.
Depression Outcomes at 6 Months by Baseline BMI, in Patients With Follow-up PHQ-9 Measurements.

Abbreviations: BMI, body mass index (in kg/m2); PHQ-9, Patient Health Questionnaire.
Using a logistic regression model to predict the odds ratio for the outcome of remission (PHQ-9 score <5) at 6 months, the clinical factors of recurrent depression, PHQ-9 score and an abnormal MDQ score were found to be statistically significant, an observation that had been shown in prior studies(Table 3). While controlling for all variables, the patient’s BMI at baseline was not an independent risk factor for depression outcome at 6 months, even when evaluated by category of BMI (normal, overweight, obese, or morbid obesity).
Odds Ratio for Clinical Remission (PHQ-9 Score <5) in Collaboration Care Management for Depression After 6 Months, by Variable.

Abbreviations: PHQ-9, Patient Health Questionnaire; GAD-7, Generalized Anxiety Disorder Scale; AUDIT, Alcohol Use Disorders Identification Test; MDQ, Mood Disorder Questionnaire; BMI, body mass index.
Discussion
In this retrospective study using a clinical CCM database, we found that our initial hypothesis was not supported. The patient’s baseline BMI category was not an independent predictor for depression outcome 6 months after enrollment in CCM.
With only 27.4% of our depressed patients having a normal BMI at the time of diagnosis and enrollment into CCM, a negative impact of obesity on remission of depressive symptoms would have had significant clinical implications. Based on these results, BMI was not independently associated with outcomes at 6 months.
More than 80% of patients studied were female. It had been reported that there might be a gender-specific cross-sectional correlation between BMI class and depression symptoms and that increased BMI in men may have an inverse association with depression. 18 A study conducted among elderly males with depression in China showed a trend toward decreasing depressive symptoms with increasing BMI. 19 In our study, gender was not determined to be an independent predictor of depression outcomes at 6 months. Still, it would be interesting to further study this relationship in a larger sample of men treated under CCM.
To our knowledge, no prior study had looked into BMI as a predictor of depression outcome in the setting of CCM, with this large sample size. Compared with prior studies,8,9 no specific therapy was evaluated and the endpoint was 6 months rather than 5 or 8 weeks. Patients were recruited from a primary care outpatient practice, and therapeutic management decisions were at the discretion of the primary care provider, with oversight by the CCM psychiatrist. Although not studied, an analysis of comparing time to remission by BMI would also be intriguing.
This study does have several limitations. It involved only one, relatively homogeneous clinical population (that generally had adequate health insurance). It was a retrospective analysis with significant attrition. Also, it is possible that the time frame was too short to see an impact of obesity on depression outcomes. Longer term follow-up may be needed. Although this study was not designed to evaluate the effect of depression improvement on weight over time, we currently have a study on this in progress. Future studies evaluating measuring specific obesity-directed treatments (such as motivation interviewing or dietitian interventions) in addition to CCM for major depressive disorder would be encouraged.
Conclusions
Collaborative care management for depression has been shown to be effective for improving depression outcomes; yet minimal prior research has focused on other clinical comorbidities that might affect outcome in this model. Although obesity was common in our study population, it was reassuring, based on this study that 6-month depression treatment outcomes do not appear to be significantly affected by the patient’s baseline BMI.
Footnotes
Acknowledgements
Thanks to Julie Maxson for assistance in data collection.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.