
Abstract
Introduction
Polypharmacy among elderly patients, usually defined as 10 or more prescriptions, is regarded as a serious concern because it has been implicated in drug–drug interactions, adverse drug reactions, low adherence to drug therapy, falls, fractures, visits to emergency departments, unplanned hospitalizations due to adverse drug reactions,1-6 increased health care costs, and even increased mortality.7-9 Furthermore, the number of medications taken by the elderly is increasing. 10 Strategies for monitoring, understanding, and controlling polypharmacy are increasingly important. In fact, the US Department of Health and Human Services has identified the reduction of polypharmacy in the elderly as a goal of Health People 2010. 11
Risk factors for potentially inappropriate medication use in the elderly include gender, age bracket, living arrangements, and education. In a Swedish study, use of some medications was higher among elderly persons residing in institutions, but the risk of drug interactions was lower in this group than in the community-dwelling elderly. 12 Another Swedish study reported that older age and female sex were related to inappropriate use of psychotropic drugs, but the risk for potentially serious drug–drug interactions was inverse for these variables. 1 In short, the risk factors for polypharmacy are complex and not well understood.
Investigators have used various thresholds to define polypharmacy, ranging from more than 5 to ≥25. No consensus exists as to the most valid cutoff level. Instead, most investigators seem to rely on associations in the data available to them to determine how many medications constitute polypharmacy.
Quality indicators such as polypharmacy can be studied using the traditional epidemiological triad: person, place, and time. 13 The purpose of the study reported here is to investigate the epidemiology of polypharmacy among geriatric family medicine patients at hospital discharge. We expected to find that polypharmacy varied across the places to which patients are discharged and to find chronological patterns. We also expected that polypharmacy would be related to personal characteristics of the patients studied.
Methods
Hospital discharges were chosen for study because medication discrepancies in elderly patients making the hospital-to-home transition are common. 14 Two groups of hospital admissions to a family medicine inpatient service were sampled over a 12-month period. All the patients in the first group were rehospitalized within 30 days. The second group was a random sample of hospitalized patients who were not rehospitalized within 30 days. Patients 65 years and older were selected from each group, resulting in 46 readmitted within 30 days and 96 not readmitted within 30 days. The 2 samples were combined (N = 142) because tests revealed no interaction between readmission status and any of the independent variables.
Medication count was the dependent variable and included all medications both prescribed and over-the-counter listed on the patient’s hospital dismissal summary, which is reviewed with the patient prior to discharge. Polypharmacy was defined as >16 medications at dismissal; this divided the data at the 75% percentile. Independent variables related to person, place, and time. Personal characteristics measured were number of emergency room visits in the 12 months prior to hospitalization, number of hospitalizations in the previous year, number of high-risk diagnoses, age, gender, education measured in years, and marital status (married vs not). Place was defined by the living situation at admission and the disposition location. Disposition location was classified as home with self-care versus any location in which personal health services were provided, including home with home health care. Time was measured as the month of admission. Diagnoses determined to be high risk based on hospital admission rates 15 were chronic obstructive pulmonary disease, cancer, diabetes mellitus, congestive heart failure, and coronary artery disease. Patients were scored as having 0 to 1 versus 2 or more of these high-risk conditions.
Mean differences in emergency department visits were compared for patients who had more than 16 medications and for those who had ≤16 using the Kruskal–Wallis test. The Kruskal–Wallis test was also used to test for differences in hospital admission in the previous year. A t test was used to test for age differences and differences in years of education. Chi-square tests were used to test for differences in gender, living situation, discharge location, marital status, and number of high-risk diagnoses. Variables significant in the foregoing tests were entered into a multiple logistic regression model to compute unconditional odds ratios.
Results
The mean number of medications at dismissal was 13.5 (range = 3-34, median = 13). We found that 23.2% of patients were taking more than 16 medications at the time of dismissal from the hospital. No interactions were found between readmission status and any of the independent variables.
Results of univariate tests are shown in Table 1. Emergency room visits and hospital admissions in the previous year were not related to polypharmacy. Age, number of years of education, marital status, and living situation at the time of admission to the hospital were not related to polypharmacy. Table 2 shows that 2 or more high-risk diagnoses were independently related to polypharmacy (odds ratio [OR] = 4.75, confidence interval [CI] =1.0-11.2, P = .00). Being discharged to a location with personal health services such as home health care or a skilled nursing facility also was related to polypharmacy (OR = 3.07, CI = 1.3-7.2, P = .01).
Association of Polypharmacy With Personal Characteristics and Place (N = 142).
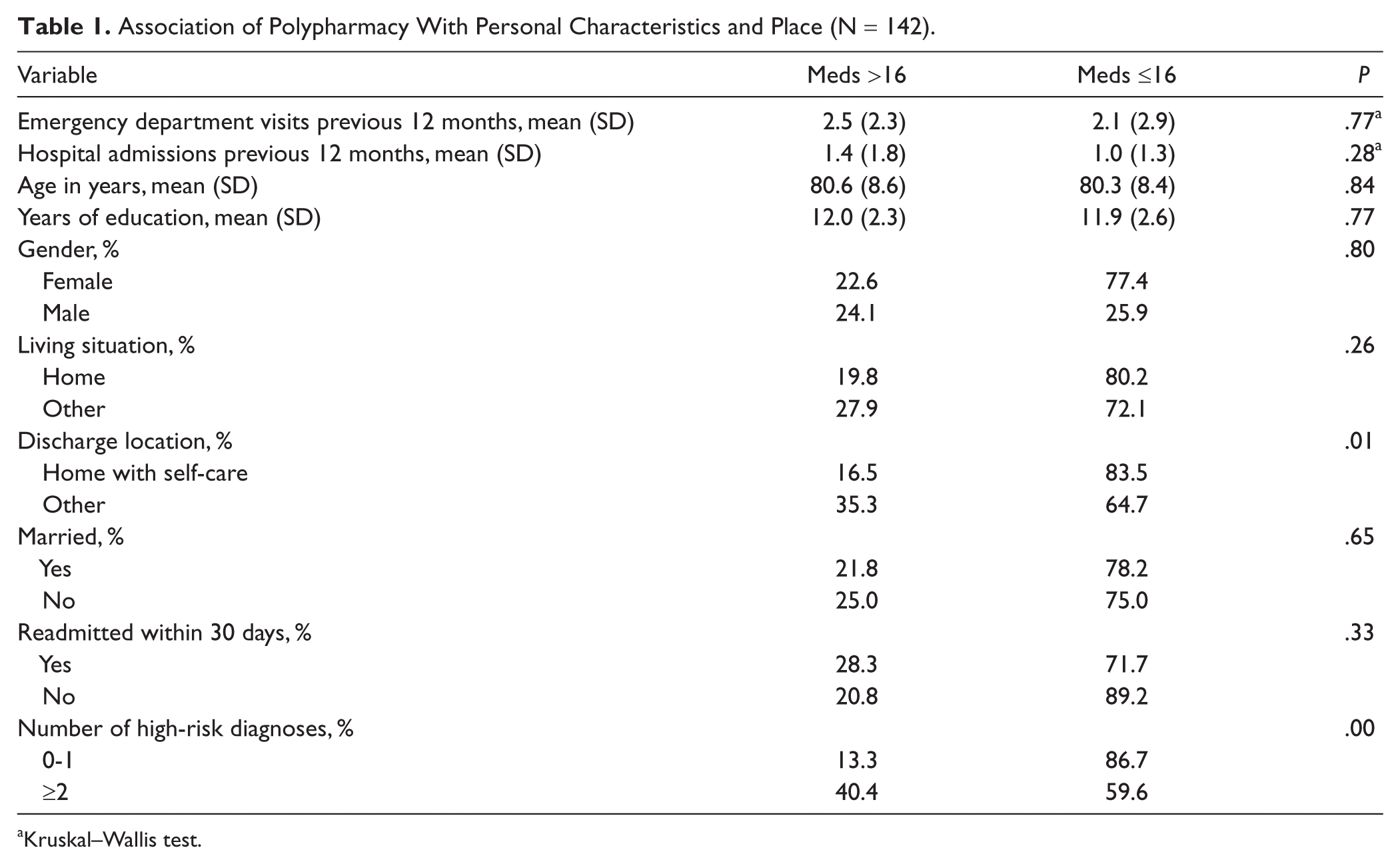
Kruskal–Wallis test.
Logistic Regression Analysis of Polypharmacy (N = 142, P = .00).

The percentage of cases taking more than 16 drugs was plotted by month (Figure 1). Percentage ranged between 0% and 50%. The percentage for any given month did not rise above an upper confidence limit set at 2 standard deviations above the mean, indicating no discernable seasonal pattern.

Percentage >16 medications by month with mean and 2-sigma upper confidence limit.
Discussion
A study of the epidemiology of quality can be described as an example of managerial epidemiology. 16 Locating risk factors for polypharmacy in person, place, and time is a first step toward efficient monitoring and more detailed investigations. Pharmacy review of the medication lists of patients at high risk for polypharmacy is necessary to further validate this indicator.
The findings of this study differ somewhat from published evidence. Age, gender, education, and living situation at the time of admission were not significant in our sample. This may be because of local circumstances. The sample may have been too small to detect significance in these personal characteristics. We found that being discharged to a location in which personal health services were provided was associated with polypharmacy. This corresponds to a previously reported association between institutionalization and polypharmacy. 12
Polypharmacy has previously been described among nursing home residents, recipients of home health care, and elderly individuals at increased risk for hospitalization. Twenty-four percent of nursing home residents receive nine or more medications. 17 It could easily be argued that nursing home residents, home health care recipients, and hospitalized individuals are sicker and have more chronic illnesses, making increased drug use appropriate and even necessary. However, a study of hospitalized frail older patients found that 44% were discharged with at least one unnecessary medication. 18 It appears that there is a cycle: Polypharmacy among home health care recipients increases the risk of hospitalization and polypharmacy at time of hospital dismissal increases the risk for requiring nursing home or home health care. Although the cause of the polypharmacy in individuals being dismissed from the hospital setting to the nursing home or home health care setting cannot be delineated from this study alone, it does identify a population in whom providers can target for interventions.
Combining those readmitted with a random sample of those not readmitted may introduce selection bias not accounted for by the interactions we checked. Many studies have found prior hospitalization, living situation, and disease comorbidity to be associated with readmission risk19-21. However, our small sample size in this hypothesis generating study may have been inadequate to detect these differences. Since the data are cross-sectional, the relationship between use of supportive nursing services and number of medications may not be causal. We attempted to control for complexity using a single measure (2 or more high risk conditions vs less than 2), but further adjustment may be necessary.
Our study validates those previously published that show a correlation of polypharmacy with the presence of multiple comorbid conditions in the elderly.7,22,23 The risk factors for inappropriate drug use in the elderly are complex. Since some of the studies reporting negative associations with polypharmacy were cross-sectional, it is possible that clinical complexity drives both the number of medications and the risk of adverse outcomes. A higher number of prescriptions is related to inappropriate drug use but does not measure inappropriateness directly. A study of medication use in the United States related the number of medications to assessments of potential inappropriateness and concluded that taking more than 25 medications was a risk factor. 10 However, the measures of potentially inappropriate medication use are controversial.
Multiple medication use has been shown to be the most consistent and strongest predictor of adverse drug reactions in older adults. 6 Studies have suggested that the probability of having an adverse drug reaction increases from 13% for individuals taking 2 drugs, to 82% when more than 7 drugs are taken, to 100% when more than 10 drugs are used. 11 Furthermore, upward of 12% of hospital admissions among the elderly may be secondary to adverse drug reactions. 7
In summary, the total number of medications taken is a risk factor for negative events but not proof-positive of inappropriate prescribing. The evidence available suggests that monitoring the rates of polypharmacy is prudent. High rates should trigger more detailed investigations. The same can be said for other simple quality indicators (eg, complication rates after surgery, hospital readmissions within 30 days, or risk-adjusted in-hospital mortality rates).
A limitation of our results is the small sample size, which lowers power, and the exploratory nature of the variables. Future research projects should examine homogenous case types, measure appropriateness of particular medications, and study larger samples.
Conclusion
Quality improvement interventions designed to reduce the rate of inappropriate polypharmacy among discharged persons 65 years and older can be targeted at patients who have 2 or more high-risk diagnoses and at those discharged to a location in which they will receive personal health services.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.