
Abstract
Keywords
Introduction
Retail medicine clinics staffed by nurse practitioners and physician assistants are becoming increasingly popular because of their convenience and affordability.1,2 Several studies have demonstrated that retail medicine “does no harm” in regard to return visit rates and cost of care.3-7 However, few studies have assessed their impact on continuity of care in field settings.
Retail clinic visits may weaken the patient–physician relationship if they reduce continuity of care by replacing visits with the patient’s primary care provider. This possibility is of concern to some primary care providers but has not been studied previously. Others have worried that care provided in retail clinics might drive up total costs by triggering otherwise avoidable follow-up visits with primary care providers or emergency departments due to incomplete resolution of the clinical problem. This could actually increase continuity of care, as it is normally measured, by dividing the number of visits to the primary care provider by the total number of outpatient visits.
Continuity of care can be measured and compared as the percentage of visits patients make to their primary care physicians (PCPs). The purpose of this study is to test the hypothesis that continuity of care is different for patients who have used retail clinics as compared to patients who used only the standard office practice.
Methods
Two randomized groups were selected as follows: (a) 200 adult family medicine patients seen in 1 of 3 retail medicine walk-in clinics from January 1, 2011 to December 31, 2011 and (b) 200 adult family medicine patients who only used standard office care during the same time period. The sample was limited to patients who relied primarily on insurance offered to clinic employees, thus minimizing bias associated with financial incentives as coverage was identical between the standard office and retail clinics. Visit counts excluded visits when patients were hospital inpatients. This study can be described as an example of managerial epidemiology because the design is observational and because continuity of care is a concern to both managers and clinicians.
Patient identifiers were neither used by the data analyst nor were they supplied to coauthors. Retrospective studies of anonymous secondary data are defined as quality improvement and not as research by the local institutional review board.
The retail medicine walk-in clinics are intended for patients who have common conditions. The retail clinics are staffed by board-certified nurse practitioners and physician assistants with family medicine physicians available by telephone. The 4 standard care clinics and the 3 retail medicine clinics are owned, staffed, and managed by the same multispecialty group practice.
Continuity of care was measured as the percentage of total non-hospital visits that were made to the PCP. Continuity of care exhibited a skewed distribution; 35.5% of patients were outliers with zero visits to their PCPs. A dichotomous dependent variable was used to measure outlier low continuity (zero PCP visits vs some PCP visits). Differences in mean continuity between users of retail clinics and nonusers of retail clinics were tested using the Kruskal–Wallis statistic because variances were unequal. Differences in the percentage of zero continuity patients were tested using the χ2 statistic. The odds of being a low continuity outlier were adjusted for age and gender using multiple logistic regression analysis.
Results
Patient ages ranged from 18 to 66 years with a mean age of 39.9 years. Sixty-seven percent were female and 68.3% were married. The mean of continuity of care was 31%, but 43 percent had zero visits to their PCPs. Only 42% of patients older than 50 years used the retail clinics, versus 53% of those aged 18 to 29 years.
Mean continuity of care for retail clinic users versus other patients is shown in Figure 1. The means were 0.17 for retail and 0.44 for nonusers (P = .00). The Kruskal–Wallis test was used because of unequal variances. The percentages with zero visits to their PCPs were 54.5 for retail clinic users and 31.0 for nonusers (P = .04; see Figure 2.)
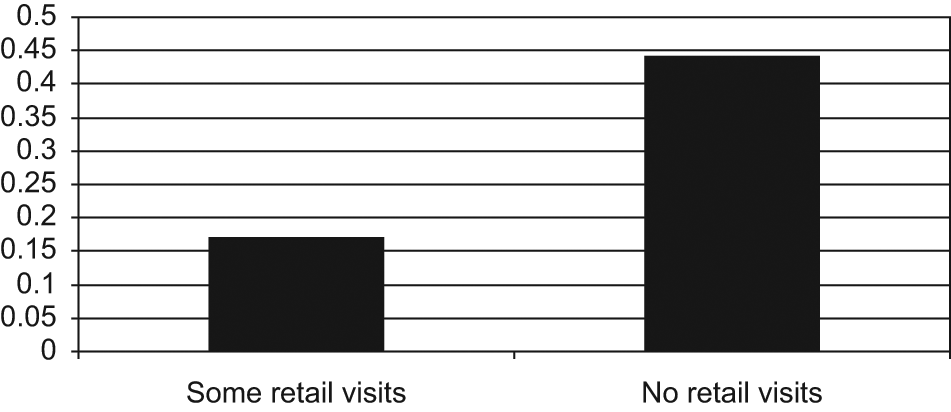
Mean continuity for users of retail clinics versus nonusers.

Percentage of patients who had zero visits to their primary care providers.
The odds of making zero visits to the PCP were adjusted for age and gender using multiple logistic regression analysis. Nonusers of retail clinics had lower adjusted odds of being a zero-continuity outlier than users of retail clinics (odds ratio = 0.38, confidence interval = 0.25-0.58, P = .00).
Discussion
Patients increasingly value speed for all types of services, including medical care. The body of systematic evidence supporting retail care models has increased steadily. Return visits of pediatric patients8,9 and adult patients10-12 to emergency departments has been studied. The cost differences of retail clinics in comparison with other forms of care have been favorably compared. 5 The impact of retail clinics on early return visits among pediatric patients was reported in 2008. 7 To study adult patients, a 2009 project used 2 different comparison groups to “triangulate” the assessment of return visits by adult primary care visits. 3 Other studies of retail medicine have addressed return visits for otitis media, 6 sinusitis, 4 standardized costs, 13 waiting times, 14 quality of care, 15 and cost savings. 16
In our study, the age composition of retail clinic patients was different from other patients; patients older than 50 years were less likely to visit retail clinics. Age is related to continuity but even after adjusting for age composition, continuity is lower for retail clinic users than nonusers in our study. In the linear model, visits to both specialists and physician assistants or nurse practitioners also were associated with lower continuity. If primary care clinics desire to increase continuity, they should consider focusing their attention on visits in these areas in addition to the retail clinic users.
A commonly used measure of continuity is the percentage of total visits that take place with one’s own physician. This was called the Usual Provider Continuity index by Breslau and Reeb. 17 Saultz and Albedaiwi 18 described this as interpersonal continuity to distinguish it from other types of continuity. Our study used the traditional measure of continuity: percentage of visits to the primary care provider. This approach may be less valid in today’s high-technology environment and with team-based care. Nonvisit care, such as phone calls and e-mail correspondence, could enhance continuity in ways not captured by the traditional care. Future research projects should explored new measures of primary care continuity.
Continuity of care is associated with many positive outcomes, including improved delivery of preventive services decreased hospitalizations lower health care costs and improved chronic disease management.19-21 Having a greater number of visits and a recent health maintenance visit with a primary care physician is associated with successful delivery of preventive services. 21 The decreased continuity of care and the large number of zero visit outliers seen among retail clinic users may undermine these goals. We did not assess these endpoints in this initial study. Further study is warranted to determine the effect of retail clinic use on the delivery of preventive services and chronic disease management within a patient-centered medical home.
The study of retail medicine clinics is a moving target. Usage of these clinics is expanding rapidly. Originally limited to treatment of minor acute illnesses, retail clinics may expand into management of chronic illnesses and may become the de facto source of primary care for large segments of the population. 2 If this happens, the decline in continuity may reverse itself.
Conclusion
Continuity in primary care is widely valued. Continuity may strengthen relationships and foster trust. In an age of automated information systems, new definitions of continuity may be necessary. The clinical practice should be able to instantly alert a continuing patient about preventive tests that might be due and services that might be needed to address chronic illnesses. Future studies should explore new measures of continuity. In addition, validating the expected benefits of continuity with regard to its impact on clinical outcomes and efficiency remains a continuing challenge.
The results of this retrospective analysis of electronic medical records suggest that our retail primary care clinics may reduce continuity of care in our clinics. This may be an artifact of not adjusting for electronic communication between provider and patient. However, our findings suggest that the growing use of retail medicine may adversely affect continuity unless steps are taken to counteract this tendency. Furthermore, efforts to increase traditional continuity might fruitfully be targeted at providers other than PCPs. At the same time, we suggest that traditional notions of continuity should be reconsidered.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.