
Abstract
Introduction
If health care reforms are to successfully contain the increasing and potentially unsustainable health care costs, then untreated mental illness, which is recognized as a significant driver of health care costs,1,2 must be addressed. Compared with commercially insured primary care populations, the Medicaid population has a prevalence of mental illness estimated at 50% versus the former’s estimated prevalence of 28%.3,4 Many of these patients with mental illness also have chronic medical disorders requiring care.5,6 Untreated mental illness impairs functioning, 7 which can result in inadequate self-care, and poor compliance with medication and medical monitoring.
Mental illness is a significant factor in disability, poverty, and unemployment.8,9 The majority of patients with chronic medical illness and psychiatric comorbidities are treated in primary care.10-12 Given the time and productivity pressures on primary care providers, patients with mental disorders may not receive optimal treatment.10-12 This cohort of patients may as well be unable or reluctant to access specialty mental health programs because of attitudinal barriers (believing that the illness will improve independently), financial barriers, stigma, or availability of clinics with specialized behavioral services.13-15
Therefore, addressing mental health issues is clinically important. Several models of primary care–behavioral health integrated care have been developed and extensively studied to address these issues. 16 Findings for some of these models show that for a possible minimal increase in immediate cost, mental illness addressed in the primary care setting can be vastly improved over the whole life span, potentially offsetting future costs.17-24 Other studies suggest that when mental health issues are adequately addressed, other health issues, such as diabetes, demonstrate improvement as well.16,25,26 Among these models is the colocation model.
The colocation model uses psychiatrists to provide behavioral health care. Colocation of behavioral health services in primary care is an international initiative as well. 27 In the colocation model, much research has been done in the colocation of psychiatrists specializing in substance abuse treatment in primary care clinics and indicates better overall outcomes with the greatest improvement observed in the sickest patients. 16 Moreover, in populations with multiple medical comorbidities, behavioral health care can reduce complications of chronic medical disorders with decreased physical health care expenses offsetting the cost of behavioral health care. 28 In the colocated model, medical management of primary care cases has also been shown to improve because of primary care and behavioral health care physicians actively coordinating care. 29
To address the growing need for behavioral health services in primary care clinics, we studied the utilization and sustainability of a colocation model at hospital-based community clinics. However, although the need for behavioral services in primary care and the potential improvement in costs and outcomes have been documented, there is scant literature on the logistical issues associated with colocation of behavioral health providers in primary care sites. Perhaps most important, given the historically lower compensation for these services, financial sustainability has been a major impediment to these initiatives. Our model specifically analyzed multiple factors we believed were critical to a successful and self-sustaining colocation program. We studied several clinics with different reimbursement models and considered the impact of a startup program with new specialty clinicians.
Program
The Setting
The County of the Bronx in New York City (NYC) offers an excellent opportunity for program development. The Bronx is home to 1.4 million residents with 31% living below the poverty level 30 compared with 21% in NYC. Medical comorbidities are prevalent as 25% of the adult population is obese, and 12% to 17% have diabetes, which is among the highest rates in NYC (20% and 9%, respectively).30,31 Rates of mental illness and annual rates of hospitalizations for mental illness are similarly elevated among the Bronx population compared with the greater NYC population at 949 admissions versus 813 admissions per 100 000 population. 31 Additionally, the Bronx demonstrates elevated annual rates of drug and alcohol related hospitalizations as well as elevated rates of drug related deaths compared with other counties in NYC. 31
Montefiore Medical Center (MMC), in the Bronx, New York, is a major academic medical center with a large system of satellite outpatient primary care clinics, many of which include specialty services. In 2010, Montefiore provided more than 3.3 million ambulatory care visits. The Department of Psychiatry at MMC in collaboration with the Montefiore Medical Group (MMG) began placing psychiatrists in busy medical group sites identified as in need of onsite psychiatric services. This naturalistic and qualitative case study focused on 3 psychiatrists working at 4 primary care sites, as shown in Table 1, to understand the challenges and opportunities of a psychiatrist working within a primary care environment.
Four Bronx Primary Care Sites and Staffing.
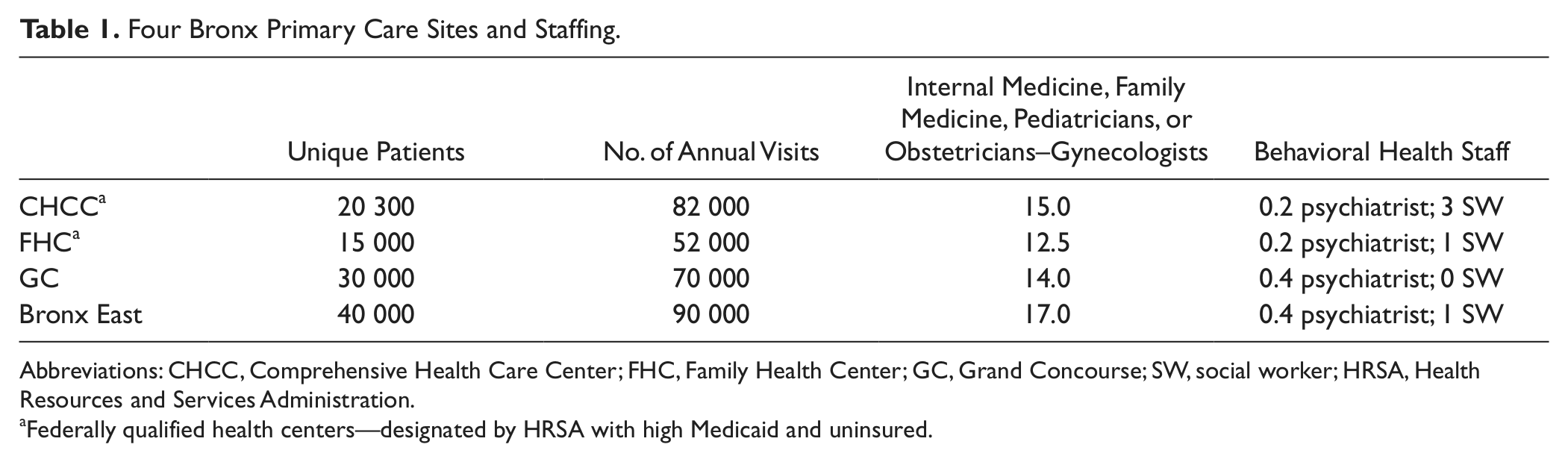
Abbreviations: CHCC, Comprehensive Health Care Center; FHC, Family Health Center; GC, Grand Concourse; SW, social worker; HRSA, Health Resources and Services Administration.
Federally qualified health centers—designated by HRSA with high Medicaid and uninsured.
Data Sources
De-identified data from quality improvement and utilization monitoring projects were collected for each of the 3 psychiatrists, including clinical activity, patient demographics, diagnoses, and practice patterns. The psychiatrists were extensively interviewed in person, by phone and e-mail regarding their observations of operational issues and experiences of providing services in the primary care settings.
Results
Demographics
The patient population for all psychiatric visits yielded a median age range of 46 to 51 years, with a race and ethnic predominance of Hispanic (61%), African American (29%), with the remaining 10% comprising Caucasian and other. Patient gender breakdown was 79.3% female and 20.3% male.
Diagnostic Distribution
The psychiatric diagnostic profiles for all 3 psychiatrists yielded a predominance of depressive and anxiety disorders. The remainder of the predominant psychiatric disorders identified is shown in Table 2. A standardized instrument to generate psychiatric diagnoses was not used. The psychiatric diagnoses shown are a reflection of the clinicians’ judgment. Of patients diagnosed with a psychiatric disorder, the top 7 medical comorbidities were hypertension (30%), asthma (22%), diabetes mellitus I and II (20%), lower back pain (16%), hyperlipidemia (13%), headache/migraine (12%), and chronic hepatitis C (10%). The great majority was diagnosed with 2 or more of the above medical comorbidities.
Psychiatric Diagnostic Profiles.

Practice Patterns
All psychiatric staff worked part-time at their respective sites. For the purpose of comparing productivity the data, which was gathered over a 6-month period, was annualized and projected based on a full-time equivalent. Actual patient visits (or attended appointments), were used to determine performance and fiscal projection. Based on the 6-month productivity, one of the psychiatrists (P1), a recent graduate of a psychiatric fellowship program, was projected to see 345 unique patients with 860 visits per year. The 2 experienced psychiatrists (more than 10 years of experience) were projected to evaluate 695 new patients with a total 1895 visits per year (P2) and 892 patients with a total of 1938 visits per year (P3), respectively, based on their 6-month productivity. The lower productivity of the recent graduate was attributed to less clinical experience and the transition from training to a practice environment. For all psychiatrists, the no-show rate was 50% for initial visits and varied between 39% and 50% for follow-up visits. The no-show rate was calculated based on ratio of attended to scheduled patient sessions. Fiscal projections factored in the absence of revenue from no-shows. The high initial visit no show rate remained consistent over time and may have been a function of the waiting time of 5 to 6 weeks for an initial evaluation.
Five patterns of follow-up care were observed unrelated to psychiatric diagnosis. The cohorts consisted of (a) weekly patients (~3% to 4%), who were seen at that frequency for several visits early in a crisis or initially for stabilization; (b) biweekly patients (~17%), seen in later weeks of a crisis stabilization; (c) monthly patients (~67%), who were more stable but in need of supportive therapy and medication management; (d) bimonthly or longer (~12%), seen for maintenance care; and (e) consultation only, composed of patients referred most commonly for presurgical psychiatric evaluation (bariatric, cosmetic, etc) and evaluation for fertility treatment or substance abuse treatment.
Revenue
Fiscal sustainability was a major consideration of this project. The high costs and overheads associated with medical office space are problematic for mental health professionals. Behavioral services are generally lower volume with lower reimbursement rates, which make them less sustainable in high cost environments. Several reimbursement models were in use depending on the practice site. Of the 4 profiled primary care sites, 2 were certified as Federally Qualified Health Centers (FQHCs). The reimbursement of psychiatric services at the FQHC is cost based. For the psychiatrist (P3) at these sites, projected annual revenue based on 1938 visits was $358 500, sufficient to sustain a full-time provider.
The 2 other sites although not FQHCs, had a high percentage of full risk capitated patients for which a case payment methodology was in effect. Reimbursement was set at $750 per referral, which was intended to cover up to 12 months of care. The new graduate psychiatrist (P1) beginning practice saw 345 referrals versus 695 referrals for the more experienced psychiatrist (P2) at the same sites. Projected annual revenue from the case payments in effect was $259 000 and $521 000, respectively. Were fee for service (FFS) reimbursement in place, using estimated reimbursement of $175 for evaluations and $130 for follow-up visits, total annual revenues would range between $127 000 and $278 000, with the former amount insufficient to cover the first year cost. P1 and P3 were salaried employees with the revenues used to support their salaries. P2 was a contractor and received case rate payment, which was sufficient to support her time commitment.
General Observations
There was unanimous agreement about the high need for on-site behavioral services at the primary care sites. Many patients referred by the primary care physicians acknowledged refusing to go to specialty mental health clinics or had agreed to go but did not follow up with outside referrals. The demand for consultations quickly resulted in a 5- to 6-week wait for an initial evaluation. The psychiatrists believed the long waitlist contributed to the high no-show rate for new evaluations.
Operational Issues
Multiple operational issues were identified. As the clinics were oriented to primary care, administrative staff had difficulties adjusting the psychiatrists’ schedules to accommodate the need for more frequent appointments required for behavioral stabilization of a subset of patients. Administrative staff although willing to make the appropriate scheduling adjustment, the deviation from the regular scheduling protocol for the medical staff remained a challenge.
The high no show rates contribute to the difficulty of sustaining psychiatric practice in most high cost environments. However, in our case study, despite the high no show-rates, all 3 psychiatrists were sustainable. Therefore, reduction of such a large no-show rate would have a major impact on revenue and reflect improved initial visit and follow-up compliance by patients, a quality improvement goal. As the limited availability of the psychiatrist impacted the time for new evaluations, which could be as long as 5 to 6 weeks, by reducing waiting times, patients might be less likely to access care through emergency departments, unaffiliated providers or clinic or postpone care. Primary care clinics generally have high numbers of walk-ins and routinely accommodate these patients who fill-in and compensate for no-shows. The psychiatrists had less ability to benefit from walk-ins as few patients present with behavioral chief complaints to primary care. Moreover, the psychiatrists had limited capability to accommodate walk-ins despite the high number of no-shows. Walk-ins with urgent behavioral needs require longer periods of time for comprehensive assessments interfering with patients waiting for their follow-up appointments. Solving the high no-show rate would greatly impact revenue and needs to be an area of further study for improvement.
Another problem was the availability of assistance with referrals to more specialized mental health and substance abuse resources, which depended on social work staff. The expertise of social work staff with these community behavioral health resources varied and resulted in referral delays or inappropriate referrals. The social work staff at the primary care clinic was adept at handling issues common to primary care and would over time expect to improve with experience. Privacy was a concern at one of the sites because of the poor sound insulation of examining room partitions. The use of white noise machines by the clinicians elicited complaints from the primary care physicians who found them distracting and interfered with auscultation. The white noise machine had to be turned off and privacy was partially improved by keeping all surrounding doors closed.
Peer Relations
The psychiatrists all noted the high productivity of their primary care colleagues. In contrast to psychiatric settings where patient encounters may range from 1 to 3 per hour, their primary care colleagues saw an average of 5 patients per hour. Primary care physicians identifying psychiatric issues had little time to adequately evaluate patient complaints resulting in consultation requests, which were generically formulated, for example, depression.
With respect to the psychiatric care provided by the primary care physicians, the need for mood stabilizers and antipsychotics often led to psychiatric referral. The high volume in these practice sites provided little opportunity for verbal feedback or discussion with the primary care physicians. E-mail became the default mode of communication. However, whenever an urgent situation arose, the primary care physicians were readily available to assist or evaluate a patient. Last, all the psychiatrists unanimously cited the enjoyment of working with their primary care colleagues and being in a medical setting.
Nonmedical Behavioral Health Providers
Among the psychiatrists, one of them (P3) participated in a coordinated behavioral health care model, working with 2 to 3 full-time social workers and a part-time psychologist. Nevertheless, this psychiatrist cited that despite the additional staff, patient need was so high that he could see only half of the patients he felt required biweekly treatment. In clinics with social work staff, much of their time was taken up with entitlement and social service activities, limiting their availability to provide treatment. The medical electronic record in place was not configured to accommodate comprehensive behavioral assessments and treatment plans. It was felt that the adequacy of behavioral documentation did not facilitate multidisciplinary care.
Patient Characteristics
A notable difference between the patient populations in primary care was the lower severity of illness compared to psychiatric clinics. It was common for many patients to never have consulted a psychiatrist, irrespective of diagnosis. The treatment responsiveness of the primary care patient population was noted. Primary care physicians and psychiatrists both reported that improvement of psychiatric symptoms improved patients’ compliance with medical care. Patients often expressed appreciation for the psychiatric care as well.
Directions for the Future
Delivering psychiatric care in primary care poses some unique environmental and financial challenges. Among them, and of particular concern, are the high initial and follow-up visit no-show rates. Decreasing the wait time for an initial visit and using nurses or social workers for initial screening and follow-up visits might improve compliance and reduce missed appointments. It is our plan to introduce the behavioral electronic medical record system, which is used throughout the Department of Psychiatry into primary care to better document assessments and treatment plans so that multiple providers can review care plans and communicate treatment updates. In addition, a comprehensive behavioral electronic medical record readily allows quality and care oversight, improvement activities and sharing of information should patients be accessing care at other behavioral sites (eg, psychiatric emergency services, outpatient clinics, etc). The unmet need for psychiatric services requires an innovative approach, which includes outcomes measurement, care and case management strategies and highly efficient use of resources.
Providing psychiatric care in a colocation model holds the potential to improve health care delivery and decrease health care costs. The Bronx has a high-need population, with few psychiatrists in primary care sites. Our data suggest that 1 full-time employed psychiatrist can provide needed behavioral services to approximately 15 000 to 20 000 primary care patients based on the ability of an experienced psychiatrist to provide 800 initial evaluations per year in a patient population where 4% seek behavioral care in the clinic. These 4 clinics would require 6 to 7 full-time employed psychiatrists based on their patient census. Our financial modeling predicts that psychiatrists are most fiscally sustainable in FQHC settings. In 2 of our clinics, we used a case-based reimbursement that can adequately fund psychiatric staff in a primary care setting in which this patient population is capitated.
The Department of Psychiatry through a wholly owned, not-for-profit subsidiary, University Behavioral Associates, has been using a case-based compensation model for more than 15 years. Patient care compensated under this program is monitored via a claims-based model and quality monitoring program. University Behavioral Associates has access to the behavioral electronic medical record used throughout the Department of Psychiatry and provides high-risk case management. 32
In many areas of the country, the shortage of psychiatrists makes a colocation model highly problematic. There is both a geographic maldistribution of psychiatrists and a manpower shortage. Tele-psychiatry and use of advance practice nurses or psychologists are some strategies used to compensate for this issue. While we had the opportunity to use psychiatrists in the colocation model, other models use collaborative care, which has also been shown to be efficacious in addressing the challenges confronting the need for greater delivery of psychiatric care to the primary care population where there are limited behavioral health resources. In the future, the opportunity for global budgeting and utilization of medical cost savings such as may occur in Accountable Care Organizations or Health Homes may provide an opportunity for supporting psychiatric services, which is problematic under fee for service reimbursement. Global budgeting for a population and need to generate medical cost savings may well foster the placement of behavioral services in primary care sites.
Conclusion
There is a need for psychiatric services at large primary care clinics in urban environments. It is financially feasible for hospital–provider systems to support a colocation model. Optimally integrating psychiatrists into primary care clinics requires some logistical interventions because of different professional practices and more complicated scheduling needs. Potential areas for education in the primary care clinic include better knowledge of the identification of substance abuse and psychotropic medication management. In turn, psychiatrists benefit from interaction with both the health care providers and the patient population within primary care settings. Although there are challenges to integrating psychiatric and primary care, the public benefit from the improvement in quality outcomes and lower health care costs renders this initiative an imperative. This is the integrated healthcare model of the future. Recognizing and appreciating the involved issues are the first steps in effectively implementing this model.
Footnotes
Acknowledgements
We would like to thank Alessandra Leon, MD, Anthony Stern, MD, and Lisa Turtz, MD for their helpful input.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.