
Abstract
Introduction
Predictors of persons being up-to-date with colorectal cancer (CRC) screening include the following: having a physician recommendation for screening,1-5 having visited a doctor or other health care provider for a checkup in the past year, 6 having asked for a CRC screening test, 6 personal or family history of colon polyps or cancer, 6 male gender, 7 older age,1,7 having a greater number of chronic illnesses, 7 family history of colorectal cancer,1,7-10 and having engaged in other preventive cancer screenings in the previous year. 7 Lower socioeconomic status is also associated with lack of CRC screening.11-13
Since health care provider or physician recommendation for screening influences being up-to-date with CRC screening,1-3 intervention studies have been conducted to increase physician recommendation for CRC screening to patients. In a randomized controlled trial of patient and physician reminders, electronic reminders to physicians to encourage CRC screening tended to increase screening rates among patients with 3 or more primary care visits in 15 months. 14 In another cohort trial, clinical prompts on the patient medical record significantly improved the probability that a screening test would be ordered. 15 Even when patients have had a prior colonoscopy, a physician reminder increases the use of surveillance colonoscopy. 16
Knowing that the recommendation of CRC screening is one of the strongest predictors of screening, it is important to discern the differences between those persons who receive a recommendation for CRC colonoscopy screening and then do obtain a colonoscopy compared with those who do not get screened after the recommendation. Many studies have explored physician recommendation for CRC screening and the association with being screened.17-20 Studying Maryland Cancer Surveys from 2002 through 2008, it was noted that recommendations for colonoscopy/sigmoidoscopy increased over time from 67% to 83% for whites and 57% to 74% for blacks. However, in those studies, the follow-through by patients was variable. Through a person-to-person interview with 7915 subjects, 1615 (20%) reported receiving a physician recommendation. 18 In a retrospective chart review, physicians appropriately addressed CRC screening 53% of the time for 400 patients and 124 (31%) followed through with CRC screening. 21 From the 2000 National Health Interview Survey, of the 5096 persons who had a physician visit in the previous year, 4688 (92%) reported no recommendation from their doctor for sigmoidoscopy or colonoscopy. 22 Of those who completed the recommendation for sigmoidoscopy or colonoscopy, they were of older age and male. 22 Another study has compared persons who reported receiving CRC screening recommendations and the actual adherence to CRC screening for Hispanic patients. Factors associated with the nonadherence included younger age, being born in the United States, and a reported fear of testing. 19 This study reported here differs from the study by Jibara et al, 19 in that the recommendation for CRC colonoscopy screening was on the patient’s medical record, rather than one that was self-reported and focused on colonoscopy screening only. Information about CRC screening primarily comes from patient self-report,11,19,23,24 but evidence from the medical record is considered the gold standard for estimating services that have been provided patients.21,25
Advancing the research in this field by using medical record information and determining who was adherent, the purpose of this article was 2-fold: (a) to determine the characteristics of those who received a colonoscopy screening recommendation and those who did not and (b) to determine the differences between those who obtained a colonoscopy and those who did not after a physician recommendation for a colonoscopy.
Methods
After institutional review board approval, this research was conducted in the Iowa Research Network (IRENE), a Midwestern practice-based research network. Subject information was obtained through a baseline questionnaire mailed at the time of recruitment and a detailed medical record review 15 months after recruitment was initiated. The study was conducted between December 2008 and April 2011 and data analyses were conducted from April 2011 through March 2012.
This study intentionally chose a selected subset of patients from the data collected during a randomized controlled trial. The parent study enrolled patients from 16 family medicine practices in a randomized, controlled trial to test office reminder systems of gradually increasing intensity for CRC screening and assess their effect on screening. Enrolled patients due for screening within each practice were randomized with equal chance to 1 of 4 groups: (a) usual care; (b) physician chart reminder alone; (c) physician chart reminder and a multifaceted patient education mailing, including written and DVD materials about CRC screening, a self-completed CRC screening preference sheet, CRC screening reminder magnet, and a fecal immunochemical test kit; or (d) all of the preceding plus a telephone reminder from research project staff.26,27
Details of IRENE office and subject recruitment and implementation of interventions are described elsewhere.26,27 Sixteen IRENE offices participated in the study, and each office provided a list of names and addresses of patients between the ages of 52 and 79 years. A minimum age of 52 years was used, so that there would be no question that all patients were at the minimum age for initiating CRC screening. At the time the study was initiated, there was no upper age limit specified in national CRC screening guidelines, but it was felt that for many individuals reaching the age of 79 years, more serious health conditions might take precedence. Other inclusion criteria were for the patient to be residing in the community, not a nursing home, and be able to provide informed consent in English. From the lists provided by each office, a random sample of 530 individuals (50% men) was selected and invited to participate by mail invitation with the goal of 100 unscreened patients from each practice enrolling.
Baseline Questionnaire
The baseline questionnaire was mailed at the time of subject recruitment. The questionnaire was developed by the principal investigator (BTL) and contained questions about each main method of CRC screening (fecal occult blood tests, flexible sigmoidoscopy, barium enema, and colonoscopy), how recently the test was completed, and why the test was done; whether their physician had ever recommended that they undergo CRC screening; whether their doctor had ever recommended a CRC test for symptoms 11 ; and a demographic section. The questionnaire has been extensively tested with more than 500 participants in a previous study.1,28 Although developed independently of the instrument developed by Vernon et al, 29 many of the questions designed to ascertain screening status were very similar to those questions.
The subjects’ answers on the baseline questionnaire were used to determine eligibility for the parent study. Subjects were considered ineligible if they self-reported being up-to-date with CRC screening by any method (fecal occult blood testing in the past year, barium enema or flexible sigmoidoscopy in the past 5 years, or colonoscopy in the past 10 years).30-32 Thus, subjects for study were limited to those eligible in the parent study.
Medical Record Review
Half of the 16 offices had an electronic medical record and the other half had paper records. For 2 of the offices to review the record for 10 years, a review of the older paper record and the newer electronic medical record was completed. No medical record contained flow sheets for CRC prevention reminders.
Fifteen months after the first recruitment letter was sent to subjects, a medical record review for each subject was conducted by the research team. The medical record review form developed for prior studies23,28 collected information about physician–patient discussion of CRC screening tests, and the date and reason of documented performance of CRC screening tests. Total visits to the office and number of physical exams in the past 26 months, height, weight, smoking status, most recent date of the following tests: mammography, Papanicolaou (Pap) smear, prostate-specific antigen (PSA) testing, and lipid tests; medical diagnoses; and medications were also collected.
Research assistants were trained by the principal investigator to use the form. During medical record review at each office, each form was checked for any missing items. In addition, a 10% sample was double-checked for accuracy.
The research presented here is based on the medical record review. In fact, colonoscopy screening recommendation was documented in the medical record progress notes by the health care provider. In the baseline questionnaire, subjects were asked if their physician ever recommended they undergo colon cancer screening. Of the 685 subjects, 255 self-reported on the baseline survey their physician had recommended a colonoscopy. Baseline questionnaire responses do not exactly match medical record review findings presented here. Comparison of patient CRC screening self-report with medical record review has been found to be inconsistent.1,23
Data Analysis
Medical record review forms were double-entered in Microsoft Access databases and verified by a SAS program. Initially, determination of eligibility was based on self-report of screening test completion and date. However, if subjects were deemed ineligible for the study after medical record review, they were excluded from the study, as denoted in Figure 1.

Study flowchart.
The 2 main outcome variables were dichotomous (yes/no). The initial outcome is whether the patient received a colonoscopy recommendation as recorded by the physician in the medical record for the 10 years reviewed. The second was whether the patient received a colonoscopy after the recommendation.
The following tests were recorded as dichotomous variables: whether mammography, Pap smear, and PSA testing were conducted within the past 26 months and lipid tests within the past 5 years as recorded on the medical record. The income variable was categorical starting at “less than $20 000” and increasing in $20 000 increments to “greater than $100 000.” The variable was collapsed to dichotomous of less than $40 000 to greater than or equal to $40 000. All medications listed in the medical record as active were counted, which included prescription and nonprescription medications. Polypharmacy is denoted as 5 or more prescription medication. As such, medications were dichotomized at “1 or no medications” versus “2 or more medications.” Medical diagnoses were reviewed for all subjects and were dichotomized at “1 or no diagnoses” versus “2 or more diagnoses.” Physician visits were also dichotomized after a review of the frequency of visits at “0 to 2 visits” or “3 or more visits.” Means and frequencies were calculated. Chi-square tests and t- tests were used as appropriate to compare the 2 groups. SAS was used for the analysis (SAS, version 9.1.3, SAS Institute, Cary, NC).
A Glimmix model was fit in SAS proc Glimmix for each binary outcome using the binary distribution and the logit link function. The Glimmix procedure estimates the parameters by applying pseudo-likelihood techniques. Based on these estimates, Glimmix also provides odds ratio estimates and 95% confidence intervals. Tests of hypotheses for the fixed effects are based on Wald-type tests and the estimated variance–covariance matrix. This procedure takes into account the 2-level hierarchical structure of the data: subjects clustered within clinics. Clinic effect was specified as random, and the variables with P values <.1 in the univariate analysis were included in the model. For the Glimmix model of recommendation for colonoscopy, the covariates were age less than 65 years versus 65 years and older, income $40 000 or more versus less than $40 000, physician gender, whether a nurse or physician talked about having a colon test, physical exam physician visit in the past 26 months, whether distant relative had cancer, whether a smoker, medical diagnoses less than 2 versus 2 or more, and whether had hyperlipidemia or rheumatoid arthritis. For the Glimmix model of having a colonoscopy after a recommendation, the covariates were age less than 65 years versus 65 years and older, gender, medical diagnoses less than 2 versus 2 or more, whether CRC screening was important to one’s health, perception of health, whether distant relative had cancer, and whether had gastroesophageal reflux. The intervention group variable was also included in the final models although it was not significant in the univariate analysis. Missing data were not imputed.
Results
From the 16 IRENE practices, 56015 patients were obtained to potentially invite into the study. In all, 530 (50% men and 50% women) were randomly selected from each office and invited to participate. Thus, a total of 8372 patients were randomly selected and invited to participate. A total of 743 persons were enrolled in the study and randomized to 1 of 4 groups. Medical record reviews were completed 15 months after the initial invitation. Of the 743 persons at the time of medical record review, 39 had medical records that could not be located, 9 died or moved away, and 10 were determined to be ineligible during medical record review. Of the remaining 685 subjects eligible to be in the study, 219 (32%) had a documented recommendation for colonoscopy in the medical record. Of those 219 persons receiving a recommendation for colonoscopy, 86 (39%) received a colonoscopy after the recommendation (see Figure 1).
A comparison of demographic characteristics, health care provider influence, patient family history related to CRC, and physical health will be provided next for those who received a colonoscopy recommendation. This will be followed by a comparison of demographic characteristics, health care provider influence, patient family history related to CRC, physical health, and patient health perception for those who followed through with the recommendation.
Colonoscopy Recommended
Demographic characteristics
The mean age of the 685 subjects was 61 years ranging from 52 to 79 years, 328 (48%) were men, 676 (99%) were white, 662 (99%) were non-Hispanic, and 532 (78%) were married. In total, 424 (62%) of the subjects had some college education or a college degree and 639 (93%) had health insurance. Annual combined income was provided by 641 subjects; 245 (36%) reported less than $40 000 per year. Younger subjects and those earning $40 000 or more per year were significantly more likely to be offered a colonoscopy (see Table 1).
Subjects’ Demographic Characteristics, Health Care Provider Influence, Health History, and Physical Health Comparisons for Those Recommended for a Colonoscopy and Those Not Recommended.

Abbreviations: FIT, fecal immunochemical test; CRC, colorectal cancer; PSA, prostate-specific antigen.
Health care provider influence
In total, 446 (65%) of the subjects had a male health care provider. If the health care provider was male, the patient was significantly more likely to be recommended a colonoscopy. If a doctor or nurse talked to a patient about a colon test, they were significantly more likely to be recommended for a colonoscopy. Subjects having 3 or more office visits or having a physical examination in a 26-month time period were significantly more likely to receive a recommendation for colonoscopy (see Table 1).
Patient family history related to CRC
If a patient or immediate family member had a history of colorectal cancer, there were no significant differences in the likelihood that a physician would recommend a colonoscopy (P = .830). However, having a distant relative with colorectal cancer significantly influenced the physician’s likelihood to recommend a colonoscopy (see Table 1).
Physical health
A total of 551 (80%) of the subjects had at least 1 medical diagnosis on their medical record, with a mean of 3, and a range of 1 to 10 medical diagnoses. Subjects with 2 or more medical diagnoses were significantly more likely to receive a colonoscopy recommendation. Of the 22 medical diagnoses reviewed in the medical record, the most frequently listed were hyperlipidemia and hypertension for 330 (48%), diabetes for 134 (20%), depression/anxiety for 129 (19%), gastroesophageal reflux for 94 (14%), osteoarthritis for 86 (13%), heart disease and hypothyroidism for 81 (12%), and rheumatoid arthritis for 14 (2%) subjects. Persons with a diagnosis of hyperlipidemia were significantly more likely to receive a colonoscopy recommendation than those without the diagnosis. Subjects without rheumatoid arthritis were significantly more likely to be offered a colonoscopy (see Table 1).
In all, 101 (15%) subjects smoked. Of the 357 women, 119 (33%) had a Pap smear and 182 (51%) had a mammography. Women were significantly more likely to receive a colonoscopy recommendation if they had either test. Of the 328 men, 154 (56%) had a PSA test on their medical record and were significantly more likely to be offered a colonoscopy. A total of 482 (70%) of the subjects had a lipid test on their medical record, and those persons were significantly more likely to receive a colonoscopy recommendation (see Table 1).
Ninety-three (14%) of the subjects had no medications listed on their medical record. Of the 592 (86%) subjects taking medication, the mean number of medications was 6 and ranged from 1 to 22. There was no significant difference in colonoscopy recommendation between those taking 0 or 1 medication and those with 2 or more medications (P = .115).
Weight and height for body mass index (BMI) were on the medical record for 512 (75%) subjects. Mean BMI was 31 kg/m2, ranging from 16 to 62 kg/m2. Mean BMI for the recommended colonoscopy group was 30.72 kg/m2 and for the not recommended group was 31.05 kg/m2 (P = .932). There was no significant difference in colonoscopy recommendation by BMI category of underweight, normal, overweight, and obese (P = .676).
No significant difference was noted in subjects’ perception of health status being good, very good, or excellent compared with poor or fair between those having a colonoscopy recommendation and those not (P = .156).
Colonoscopy Completed
Demographic characteristics
A total of 219 subjects had a recommendation for colonoscopy documented on their medical record, and 86 (39%) followed through with a colonoscopy after the physician recommendation. One hundred and nine (50%) subjects were men, 218 (99.5%) were white, 211 (98%) were non-Hispanic, and 175 (80%) were married. Mean age of persons having the colonoscopy was 70 years. Significantly more men than women had a colonoscopy after the recommendation. One hundred and forty (64%) of the subjects had some college education or a college degree, and 208 (95%) had health insurance. Annual combined income was provided by 203 subjects; 52 (24%) reported less than $40,000 per year. No difference in income level was noted between those having a colonoscopy or not (see Table 2).
Subjects’ Demographic Characteristics, Health Care Provider Influence, Health History, and Physical Health Comparisons for Those Completing a Colonoscopy After a Physician Recommendation.

Abbreviations: FIT, fecal immunochemical test; CRC, colorectal cancer.
Health care provider influence
Gender of health care provider was not associated with individuals following through on a colonoscopy (P = .176). Having the opportunity to ask their doctor about colon cancer screening did not indicate they were more likely to have a colonoscopy (P = .787). No significant differences in colonoscopy completion were noted between subjects having 3 or more office visits (P = .182) or number of physical exams (P = .737) in a 2-year time period and those having fewer visits.
Patient family history related to CRC
If a patient or an immediate family member had a history of CRC, there were no significant differences in their likelihood of having a colonoscopy following a recommendation (P = .229). If a patient had ulcerative colitis, there was also no significant difference in the probability of having a colonoscopy (P = .207). However, persons having a distant relative with CRC were associated with having a colonoscopy (see Table 2).
Physical health
Of the 218 persons having a colonoscopy, 187 (86%) had a medical diagnosis on their medical record, with a mean number of 3 and a range of 1 to 10 medical diagnoses. Having 2 or more medical diagnoses associated with obtaining a colonoscopy, but having a medical diagnosis of gastroesophageal reflux did not (see Table 2). Twenty-eight patients smoked, and there were no differences in colonoscopy completion between the smokers and nonsmokers (P = .695).
Of the 110 women, 57 (52%) had a Pap smear and these women were not significantly more likely to have a colonoscopy (P = .647). Seventy-one (65%) women had a mammogram and these women were significantly more likely to have a colonoscopy completed. Of the 109 men, 88 (81%) had a PSA test on their medical record, which was not significantly associated with having a colonoscopy (P = .556). In all, 179 (82%) of the subjects had lipid test results on their medical record which did not make a difference if they had a colonoscopy (P = .092).
The number of medications found on medical records included a count of prescription and non-prescription medications. Of the 218 subjects, 15 (7%) had no medications listed. Of the 203 subjects taking medication, the mean number of medications was 6 with a range of 1 to 18. Those taking 2 or more medications were not any more likely to have a colonoscopy than those taking fewer medications (P = .184).
Weight and height for BMI were included on the medical record for 180 (82%) subjects. Mean BMI was 31.51 kg/m2 for those having a colonoscopy and 30.14 kg/m2 for those not having a colonoscopy. There was no significant difference in having a colonoscopy after the recommendation among BMI categories of underweight, normal, overweight, and obese (P = .545).
Patient health perception
If CRC screening was important to the subject, they were significantly more likely to have a colonoscopy (see Table 2).
Glimmix Model Results
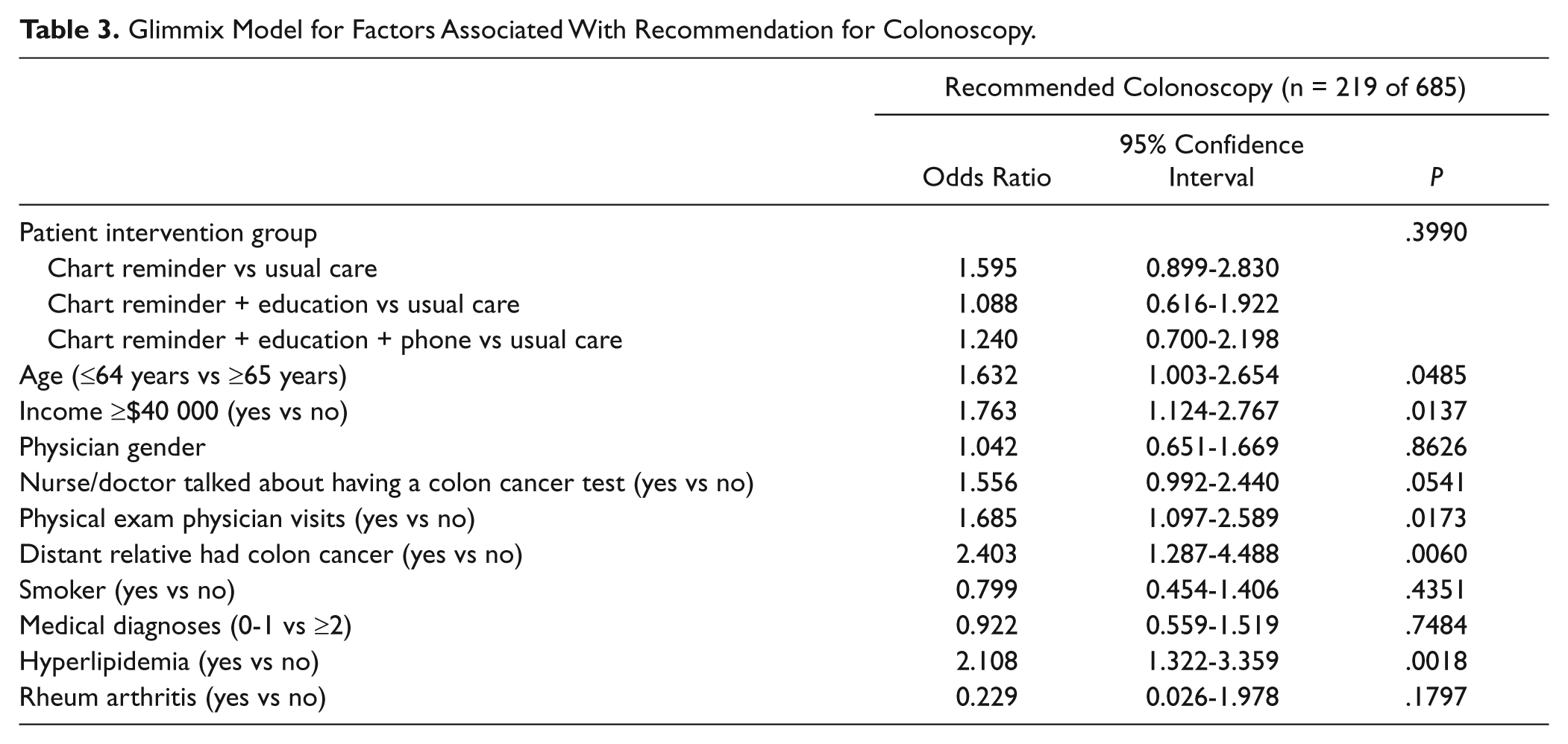
In the Glimmix model, significant factors associated with persons who receive a recommendation for a colonoscopy were age <65 years compared with those 65 years and older, having an annual income of $40 000 or higher versus less than $40 000, having a physician or nurse discuss colon cancer tests, having physical exam visits in the preceding 26-month period prior to medical record review, having a distant relative with colon cancer, and having a medical diagnosis of hyperlipidemia (see Table 3). In the Glimmix model, significant factors associated with a person who received a colonoscopy after a recommendation were being in the older age-group, being male, and feeling the colorectal cancer screening is very important (see Table 4 and Figure 2).
Glimmix Model for Factors Associated With Recommendation for Colonoscopy.
Glimmix Model for Factors Associated With Completion of Colonoscopy.


Major findings.
Discussion
In this group of subjects from a Midwestern practice-based research network, 32% had documentation of a written recommendation for a colonoscopy in their medical record. This recommendation percentage was higher than other studies at 8% 22 and 20% 18 but lower than another retrospective chart review at 53%. 21 Those persons who received a colonoscopy recommendation differed from those who did not. Individuals who received a recommendation for colonoscopy tended to be less than 65 years old with a mean age of 57 years, have higher incomes, and were more likely to have had a physician or nurse discuss CRC screening in the past, to have had a physical exam in the preceding 26 months, having a medical diagnosis of hyperlipidemia, and to have completed other recommended preventive services. They were more likely to report a distant family history of colon cancer. Education level was not associated with receiving a recommendation.
In the group of subjects receiving a colonoscopy recommendation, only 39% followed through with the recommendation similar to an earlier study at 31%. 21 Those persons proceeding to have the colonoscopy differed from those persons who did not. The typical persons following through with a colonoscopy recommendation were older, with a mean age of 70 years, male, and more likely to perceive colorectal cancer screening as very important. Another study found those who followed through on sigmoidoscopy or colonoscopy were older and male. 22
Provider recommendation to be screened with a colonoscopy influenced a third of the persons to adhere to that recommendation to have a colonoscopy, similar to other studies of a provider recommendation influencing persons to be screened.1-3 Education level did not influence provider recommendation for CRC screening in our study. This is in contrast to another study where those with high school education or less were not likely to receive a provider recommendation. 33
In our study, those with a higher income were more likely to have a colonoscopy recommended, but that was not the case in another study where income was not a predictor. 33 In the study by Ye et al, 33 income level was dichotomized at $25 000 with 20% nonresponders, whereas our income level was dichotomized at $40 000 with 6% nonresponders. It is unfortunate that persons with a lower income are not having a colonoscopy recommendation. There was a significant correlation between age and income in that the younger the person the higher the income, which is reasonable because young persons are more likely to be employed and older persons are more likely retired or on a fixed income.
However, in our current health care system, many cannot afford the copayment or lack insurance for a colonoscopy. Economic limitations should not influence a physician making a recommendation to have a colonoscopy and solutions for financial limitations need to be sought and resolved. External funding sources are available for persons who are uninsured or underinsured, such as David’s Fight organization (http://www.davidsfight.org) in Iowa. Unfortunately, it takes time to find these resources, which busy primary care settings do not have. Medicare does cover a screening colonoscopy and possibly that is why those following through on the recommendation were in the older age-group. The federal health law, the Patient Protection and Affordable Care Act (H.R. 3590) specifies that insurers must fully cover services such as the colonoscopy that have earned an A or B rating from the US Preventive Services Task Force. 34 Colon cancer is a disease that can be prevented or cured and numerous studies have demonstrated colonoscopy is cost-effective. 35
Nonadherence to having a colonoscopy after a recommendation was a younger age in this study, similar to the findings in an Hispanic population study identifying characteristics of patients who adherence to the physicians recommendation for a colonoscopy. 19 Griffin et al 36 studied medical records and self-report of CRC screening to determine if there was bias in self-reporting. They found no significant difference in colonoscopy completion by gender different from our finding of males more likely to have the colonoscopy. 36
The mean BMI for subjects in this study was in the category of obese and 70% had lipid test results on their medical record with 48% having the medical diagnosis of hyperlipidemia. In the univariate analyses, there were no significant differences in the outcomes by BMI categories and this maybe because the subjects in this study were for the most part overweight with only 17% in the normal weight category. Those with a diagnosis of hyperlipidemia were more likely to be recommended to have a colonoscopy, which may have to do with physician knowledge of obesity as a risk factor for colon cancer. In a recent study, overweight/obese women were found to be at increased risk for CRC and had a propensity not to screen for CRC. 37
This study has several limitations. The patient population is from practices in the Midwest who were willing to sign an informed consent to participate in a study about colon cancer screening. Thus, they may be more interested in CRC screening than the average American and may not be representative of populations in other parts of the United States. We relied on what was documented in the medical record to determine whether a recommendation for CRC screening was made. In some cases, physicians may have recommended screening but not documented it in the medical record. No real marker for pain was collected in the study and if abdominal pain influenced a recommendation or the follow-through to have a colonoscopy that is not known. Whether arthritic pain hindered the physician to refer a patient for a colonoscopy is also not known from these data.
Receipt and documentation of a physician’s recommendation for CRC screening is important and was suboptimally recorded in the medical records reviewed as 68% of the subjects had no documentation. In addition, patient follow-through with having a colonoscopy after a recommendation was also suboptimal, with only 39% completing a colonoscopy following a recommendation. A new finding was that those with a diagnosis of hyperlipidemia were more likely to be recommended a colonoscopy as 80% of subjects with a recorded BMI in this study were in the categories of overweight or obese.
Colorectal cancer screening interventions designed solely to increase health care provider recommendations for screening is not enough without addressing the CRC screening adherence rate. To know and provide interventions for the rate of adherence in a practice setting would have a greater significant public health impact in reducing the CRC burden.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article:
We gratefully acknowledge the support of the American Cancer Society (Research Scholar Grant Targeted-08-148-01-CPPB, BTL) and the University of Iowa, Department of Family Medicine, Iowa City, Iowa.