
Abstract
Introduction
Colorectal cancer (CRC) is the second most common cause of cancer related deaths in men and women. 1 In 1997, evidence-based CRC screening recommendations were published and endorsed by professional gastroenterology societies and the American Cancer Society. 2 The guidelines were last updated in 2010 3 and offer specific recommendations regarding the use of 4 different screening tests (annual fecal occult blood testing [FOBT], flexible sigmoidoscopy [FS], double-contrast barium enema [DCBE], and colonoscopy) that could be used alone or in combination. There have been multiple reports showing a wide variation in the choice of a CRC screening test. 4 This has been attributed to several factors, such as patient preferences, physician decision making, physician characteristics and specialty, and access to care (eg, geographic location and availability of subspecialty care). 5 However, it remains unknown if there could be factors related to the medical practices that may influence the choice of a screening test. For example, lower access to colonoscopy in a particular setting may lead to more reliance on FOBT.
The Veteran’s Health Administration (VHA) established the VA community-based outpatient clinic (CBOC) program in 1995 to enhance preventive care and early disease intervention for veterans through improved primary care access.6-8 Currently, there are more than 800 CBOCs operating nationwide; nearly all of which are administered by a parent VHA medical center. 9 Prior evidence suggests that CBOCs provide similar quality of care as the parent VA Medical Centers, evidenced by similar performance ratings in 6 domains—access, cost, provision of mental health services, quality of care, patient satisfaction, and utilization. 8 However, most CBOCs are not equipped to provide a wide array of diagnostic or interventional services. Access to advanced services for patients who receive primary care through a VA CBOC may be limited.
The current study evaluates differences in the choice of CRC screening test in patients receiving primary care at CBOCs and at a parent VHA medical center (VAMCs). Because most veterans receiving primary care in CBOCs have to be referred to VAMCs for gastroenterology procedures, we hypothesized that veterans in CBOCs would be less likely to undergo colonoscopy but more likely to receive FOBT. We also hypothesized that differences between CBOCs and VAMCs in the use of VA CRC screening procedures would be greater in older patients than younger patients, because older patients may have greater access to non-VA care through Medicare benefits 10 and because CBOC patients may be more likely to use non-VA services. 11
Methods
Data Sources
Study data were derived from 2 VHA administrative data files: The Patient Treatment File (PTF) captures information on all inpatient admissions to VHA facilities and the Outpatient Care File (OPC) contains data on all outpatient encounters at VHA facilities and community-based clinics. Data elements in the PTF and OPC include (a) demographic information, including residential zip code; (b) type of clinic (VAMC vs community-based); (c) clinic specialty (eg, primary care, mental health); (d) principal and secondary diagnoses codes based on the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM); and (e) procedure codes based on ICD-9-CM codes and the Current Procedural Terminology (CPT) coding system.
Patient Population
Patients were included if they met the following criteria: (a) aged 50 years or older as of October 1, 2009 and (b) 2 or more visits to a VHA primary care clinic in fiscal year 2010 (October 1, 2009 to September 30, 2010). These inclusions identified patients using VHA for primary care in 2010 and who were potentially eligible to receive one of the recommended procedures for CRC screening. Patients were excluded because of missing age, gender, or zip code (n = 67 124), yielding a sample of 2 837 770 patients.
Study Variables
The primary dependent variable was the receipt of a procedure (FOBT, FS, or colonoscopy) for CRC screening or surveillance in a VA facility in fiscal year 2010. All procedures were identified in the VA PTF and OPC files based on ICD-9-CM and CPT procedure codes and were categorized as being performed for diagnostic or for screening and/or surveillance using ICD-9 codes as described by El-Serag et al. 12 The primary independent variable of interest was the type of clinic where the patient received primary care (ie, a VAMC or CBOC). For patients with primary care visits at both a VAMC and CBOC, categorization as VAMC or CBOC was based on the site where the majority of primary care encounters occurred. Other independent variables that were used in the analysis included age, gender, distance between veterans’ residence and the nearest VAMC (based on the distance between zip code centroids), and comorbidity. Comorbid conditions were defined by using a widely available algorithm developed by Quan et al. 13 In addition, our study used zip code level approximation to census tract RUCA codes.14,15 Patients were also categorized as average-risk and high-risk for CRC based on CRC risk factors (including positive family history of CRC, personal history of polyps or inflammatory bowel disease) and validated ICD-9-CM-based algorithms. 16
Analysis
Bivariate analyses compared differences in demographic and clinical characteristics, in overall rates of screening, and in rates of each of the four screening procedures in patients receiving primary care in VAMCs and CBOCs using the χ2 or Wilcoxon signed rank test. Second, multivariable logistic regression analyses determined the relative odds of the use of individual procedures in CBOC patients, relative to VAMC patients, controlling for patient demographic and clinical characteristics. Patient characteristics included factors that were related to the use of individual procedures in bivariate analyses (P < .001) or that were identified in previous studies on factors impacting the likelihood of CRC screening (eg, race, gender, access, residential location).17-19 Multivariable models were estimated using a generalized linear logit function with random effects for individual VA CBOC and VAMC facilities. Additional multivariable analyses examined associations between the site of primary care (CBOC vs VAMC) and receipt of a screening procedure within subgroups of patients categorized according to CRC risk (high vs low) and according to age (<65 years and ≥65 years). All analyses were conducted using SAS statistical software, version 9.2 (SAS Institute, Inc, Cary, NC). The study was approved by the University of Iowa Institutional Review Board and the Research and Development Committee at Iowa City VA Medical Center.
Results
Overall, study participants had a mean age (SD) of 68.1 (10.7) years and 95% were male. Sixty-six percent of the patients were white and 13.2% were black; information on race was missing in 15.6%. Roughly half (50.5%) of patients were classified as receiving primary care in a CBOC and half in a VAMC (49.5%). CBOC patients were older, more likely to be white, male, reside more than 60 miles from a VAMC, and to reside in a rural area (Table 1). In contrast, CBOC patients were less likely to have chronic obstructive pulmonary disease, congestive heart failure, and diabetes (Table 1). In addition, CBOC patients were less likely to be categorized as high risk (9.5% vs 10.6%, P < .001).
Baseline Characteristics of Patients by Site of Primary Care: Community-Based Outpatient Clinic (CBOC) Versus Veterans Administration Medical Center (VAMC).

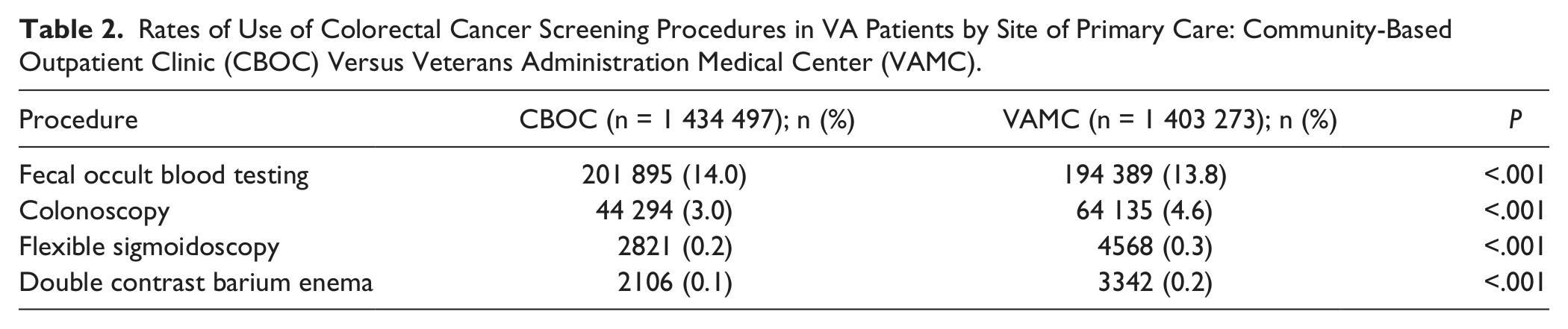
Community-based outpatient clinic patients were less likely to receive any of the 4 recommended CRC screening procedures than VAMC patients (17.4% vs 19.0%, P < .001); among the individual procedures, CBOC patients were less likely to receive colonoscopy, sigmoidoscopy, and DCBE, but were more likely to receive FOBT, although the magnitude of the difference was small (Table 2). The differences in use of colonoscopy in CBOC and VAMC patients and the relative similar use of FOBT were consistent in high- and average-risk patients, when examined separately (Figure 1).
Rates of Use of Colorectal Cancer Screening Procedures in VA Patients by Site of Primary Care: Community-Based Outpatient Clinic (CBOC) Versus Veterans Administration Medical Center (VAMC).

Rates of use of FOBT and colonoscopy by site of primary care (CBOC vs VAMC) and by risk for colorectal cancer.
In multivariate analyses accounting for the clustering of patients within individual CBOCs and VAMCs and adjusting for demographic factors, comorbidity, distance from a VAMC, and location of residence (urban vs rural), the adjusted odds of receiving a colonoscopy were lower in CBOC patients relative to VAMC patients (0.73; 95% confidence interval [CI] = 0.64-0.82; P < .001). The lower adjusted odds of colonoscopy in CBOC patients were consistent in high- and average-risk patients and in patients younger than 65 years and those 65 years and older (Table 3). As hypothesized, the magnitude of the difference in the use of colonoscopy in CBOC and VAMC patients was greater in patients 65 years and older than in patients younger than 65 years (Table 3). In contrast, the adjusted odds of receiving FOBT in CBOC and VAMC patients were similar in average-risk patients (adjusted odds ratio = 1.15; 95% CI = 0.95-1.39; P = .15) and high-risk patients (adjusted odds ratio = 1.13; 95% CI = 0.95-1.34; P = .17).
Odds of Colonoscopy a in Patients Receiving Primary Care in Community-Based Outpatient Clinics (CBOCs) Relative to Veterans Administration Medical Centers (VAMCs).

Adjusted for demographics, comorbidity, distance from a VAMC, and urban using logistic regression.
Discussion
The current study examined the variation in the use of CRC screening tests in veterans receiving primary care in CBOCs and parent VAMCs. Several key findings deserve emphasis. First, veterans receiving care at a CBOC were less likely to receive screening or surveillance colonoscopy, FS, and DCBE than veterans receiving care at VAMCs. This difference remained significant even after adjusting for rural location, distance from a parent VAMC, and other patient demographic and clinical characteristics. Second, these lower rates of screening procedures were not offset by higher utilization of FOBT and were consistent in patients at average and high risk for CRC. Finally, the difference in the use of colonoscopy in CBOCs and VAMCs was larger for patients 65 years or older than for patients younger than 65 years, suggesting that older patients who receive primary care through VA CBOCs may use more CRC screening services outside VA relative to those younger than 65 years.
The lower rates of CRC screening methods in patients receiving primary care at VA CBOCs as compared with VAMCs can be explained in several different ways. First, CBOC patients could be less likely to be offered CRC screening tests than VAMC patients. This seems contrary to a previous report by Hedeen et al, 20 who found that CBOCs did not perform significantly lower than their parent VAMC in most of the prevention indices, including CRC prevention and screening. Another possibility could be that CBOC patients face barriers in obtaining appropriate referrals for screening methods requiring subspecialty care, although Borowsky et al 21 found that CBOC patients were no more likely to report problems in care than veterans receiving care at VAMCs. A further possibility is that CBOC patients are more likely to choose not to obtain colonoscopies, which are largely performed in VAMCs, because of distance-related factors or other perceived barriers to access. Finally, it is possible that veterans receiving care at CBOCs may be are more likely to use non-VA resources for procedure-based CRC screening tests than veterans receiving care at VAMCs. Liu et al 10 recently reported that Medicare-eligible veterans receiving primary care at CBOCs had 22% fewer VA specialty care visits and 21% more Medicare-reimbursed specialty care visits than patients receiving primary care at parent VAMCs. Unfortunately, we did not have access to non-VA data and thus could not capture any care provided outside the VA. However, our indirect finding of a larger difference in VA colonoscopy use in patients 65 years and older (who are eligible for Medicare based on age) supports this possibility.
It is important to consider our findings in the context of recent publications on this topic. For example, the mean age (SD) of patients undergoing CRC screening by any of the approved methods at the VA in our study was 64.2 years (8.5), which is comparable to findings from prior studies. 12 We found that roughly a quarter of patients who underwent CRC screening in a single year underwent colonoscopy. This rate is much higher than previously reported by El-Serag et al, 12 who used VA data from 1998 to 2003. For example, among patients undergoing CRC screening in 2003, 90.4% patients received FOBT and 4.7% received colonoscopy in this prior study; however, the use of screening colonoscopy more than doubled between 1998 and 2003. Reports from the Medicare population 22 and endoscopic databases 23 have all documented temporal increases in colonoscopy as a screening modality. For instance, in a study evaluating trends of CRC screening among Medicare subpopulations, 3.9% underwent screening colonoscopy in 1995, and 9.4% in 2003 showing an increment of about 141%. 22 A recent study also showed that most primary care physicians (86%) strongly agreed that colonoscopy was the best of the available CRC screening modalities. 24 A previous study assessing the demographic variations in CRC screening in a Washington Medicare population 25 showed that rural residents were less likely to receive invasive tests (FS, DCBE, or colonoscopy) for CRC screening (odds ratio = 0.89; 95% CI = 0.85-0.93) and more likely to undergo FOBT than urban residents (odds ratio = 1.20; 95% CI = 1.17-1.23). The findings in our study from the VA population showed similar results. However, rural location and distance (more than 60 miles) accounted for only a small portion of the difference. For example, without adjusting for rurality and distance, the adjusted odds of colonoscopy in CBOC patients, relative to VAMC patients were 0.71 (95% CI = 0.63, 0.80); after adjustment, the odds were 0.73 (95% CI = 0.64-0.82).
It is important to acknowledge several potential limitations of our study. Importantly, our study relied on administrative data, which may not completely capture the use of CRC screening procedures, particularly FOBT. In addition, information on comorbid conditions was captured from ICD-9-CM codes, which may lack sensitivity and specificity. Moreover, administrative data may not adequately assess severity of illness or categorize patients according to their risk for colon cancer 26 and do not capture important domains, such as functional status, that may affect the use of CRC screening procedures. In addition, the study was unable to account for care that patients may have received from non-VA providers. Finally, the study used a cross-sectional design and did not account for CRC screening tests patients may have received prior to 2010. Thus, eligibility for CRC screening was not directly examined. Similarly, we were unable to assess other factors related to the clinical appropriateness of any of the procedures.
In conclusion, our study suggests that patients receiving primary care at CBOCs may be less likely to receive disease screening services that require referral to a VAMC. However, evidence suggests that patients in CBOCs may be more likely to receive such services form non-VA providers. These findings provide indirect evidence of the importance of examining data from non-VA providers when making judgments about adherence to VA performance measures.
Footnotes
Authors’ Note
The views expressed in this article are those of the authors and do not necessarily represent the views of the Department of Veterans Affairs.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article:
The research reported here was supported by the Department of Veterans Affairs, Veterans Health Administration, and Health Services Research and Development Service through the Center for Comprehensive Access & Delivery Research and Evaluation. Dr. Malhotra was supported by a VA Quality Scholar fellowship from the Office of Academic Affiliations, Veterans Health Administration.