
Abstract
Introduction
In the United States, nonprofit hospitals are important institutions that not only provide acute medical services and collaborate with a spectrum of health care providers, but increasingly address nonmedical community health needs through their population health programs. Although nonprofit hospitals have long been required to provide services to benefit their communities in exchange for tax-exempt status, the 2010 Patient Protection and Affordable Care Act (ACA) introduced new reporting requirements to encourage hospitals to identify and address critical population health needs in their surrounding communities. 1 Prior to the ACA, the majority of community benefit dollars were directed to providing uncompensated patient care. 2 But with more individuals gaining health insurance through various mechanisms of the ACA, especially through the Medicaid expansion, new requirements in the ACA were added to establish new community benefit reporting guidelines and encourage hospitals to expand their efforts to identify, understand, and address nonmedical, population health needs. 3
Preliminary evidence after the ACA, however, suggests that nonprofit hospitals were not spending more money on community benefit activities despite the new reporting requirements. 4 While spending has not shifted dramatically, important case studies have emerged demonstrating hospital investments in critical public health and new partnerships between hospitals and a range of public health departments and community-based organizations.5,6 Given this evidence, we may need alternative ways to measure the contributions that hospitals are making toward community and public health.
One promising mechanism for studying hospital community benefit activities to address opioid abuse is analyzing the community benefit documents that hospitals are required to report to the Internal Revenue Service (IRS) every 3 years. These documents help us understand what needs hospitals are identifying in their communities and which they are choosing to address in their formal implementation strategies. Preliminary evidence suggests that hospitals have been less likely to address social determinants of health and behavioral health, as compared with other health needs.7,8 Very little is known, however, about the extent to which specific needs are being met by hospitals, especially issues that are critical to public health in communities across the United States such as opioid abuse. Hospitals stand to play a critical role in providing treatment, preventive, and harm reduction services given their interaction with patients with opioid use disorder in their facilities and in community-based partnerships.9-11 Evidence from small pilot studies, however, suggests that many hospitals have not been including this need in their implementation plans, even as community members identified this as a top population health need. 12
Understanding hospital efforts to address opioid abuse is critical given the public health impact of this epidemic. Deaths related to opioid abuse have skyrocketed in the past decade, with 72 000 Americans dying of a drug overdose in 2017; two-thirds of these deaths resulted from the use of illicit or prescription opioids. 13 To put this into perspective, nearly 50 000 individuals died per year at the height of the HIV epidemic in the United States. 14 Despite highly publicized mobilization efforts by state governments and communities, drug overdoses have become the leading cause of death for Americans younger than 50 years; overall life expectancy in the United States has declined for several years in a row.15,16 Complications as a result of opioid abuse have also increased, including viral infections such as HIV (human immunodeficiency virus) and HCV (hepatitis C virus), endocarditis, injection site infections, and neonatal abstinence syndrome.17-19
More information is needed regarding the extent to which hospitals are addressing opioid abuse as part of their community benefit responsibilities as well as the types of programs that are being developed. Using a national sample of nonprofit hospitals, we assess whether nonprofit hospitals are changing their opioid-related initiatives and strategies after the ACA by developing new programs and partnerships to combat opioid abuse. The aim of this article is to elucidate the specific contributions that hospitals are making toward addressing one of today’s most critical public health challenges.
Methods
The analytic sample for this study consists of a random selection of 20% of the nonprofit hospitals that responded to the 2015 American Hospital Association Annual Survey. We then constructed a dataset of IRS community benefit documents for the entire national sample (n = 597). We began by evaluating the most recent publicly available community health needs assessments (CHNAs) and implementation strategies developed by each of the selected hospitals in our sample. The reports ranged from 2015 to 2018, depending on when hospitals began their first ACA-mandated reporting cycle which must be undertaken once every 3 years.
Using primary and/or secondary data, hospitals must identify the top health needs in their communities and prepare an implementation strategy outlining which local health needs they commit to address in the following cycle. The IRS does not require hospitals to address each need identified in their CHNA but gives hospitals the opportunity to select which needs they would like to address. Hospitals who are part of larger systems may collaborate with other member hospitals to complete the CHNA and carry out programs outlined in their implementation strategies. Each hospital, however, must publish an independent report.
Although there is some variation in the structure of reports, hospitals typically follow a specific pattern in these community benefit reports. In the CHNAs, hospitals list the top community health needs (such as the top 5) and in implementation strategies list the health needs they commit to address, along with specific programs that will be implemented. For this study, the first author and a research assistant reviewed the implementation strategies developed by each hospital and coded the total number of strategies that each hospital adopted to address opioid abuse. Strategies were coded as addressing opioid abuse if the hospital had identified opioid abuse or substance abuse as a need in their CHNA and if they listed specific strategies to address this need in their implementation strategy. Based on the descriptions provided of each strategy, we coded whether each included strategy was new, existing, an expanded strategy, or primarily a partnership. Binary indicators were used to code each of these variables (0 = no, 1 = yes).
Independent variables included the type of strategy, with strategies coded into 7 groups: clinical approaches (consisting of substance abuse treatment, primary care, and emergency department services), harm reduction, prescriber guidelines, risk education, social determinants, policy advocacy, and community coalitions. We also included hospital characteristics from the American Hospital Association 2015 Annual Survey 20 : system membership (0 = no, 1 = yes), teaching hospital (0 = no, 1 = yes), and bed size (fewer than 50; 50-199; or 200-399; with 400 and greater as reference group). County-level data were obtained from the American Community Survey 2015 5-year estimates 21 and included the following: poverty rate quartile, uninsured rate quartile; rural community (0 = no, 1 = yes); and region (Northeast, Midwest or West, with South as reference group).
State opioid policies were coded for each state using the dataset and categorization process used and described by Wickramatilake and colleagues. 22 They collected data on state opioid initiatives through a web-based survey administered to state alcohol and drug agency directors and/or senior agency managers by the National Association of State Alcohol and Drug Abuse Directors. Their framework established 7 broad categories of policy: targeted risk education, provider education, prescriber guidelines, naloxone training and access, prescription drug monitoring programs, medication-assisted treatment funding, and laws and regulations. We used these 7 categories as variables and added an eighth policy variable of whether the county was in a state that had expanded Medicaid.
Analytic Strategy
In addition to assessing descriptive statistics, we used 2 different analyses to address both the nature of current strategies and the number of strategies hospitals are committed to implementing. We first employed binomial logistic regression to assess whether each strategy included in an implementation plan was new, existing, an expansion of an existing strategy, or primarily a partnership. Each binomial logistic regression model also included the type of strategy, hospital characteristics, and county characteristics. Each strategy is assessed independently. Due to hospitals having multiple strategies to address these issues, a hospital may be represented in more than one outcome.
The second analysis employed negative binomial regression to assess the factors related to the count of total activities, our dependent variable. We included hospital and community characteristics as independent variables, as well as which state policies were in place at the time of the implementation plans. All statistical analyses were conducted using Stata 15. 23
Results
Figure 1 reports the number of strategies that hospitals committed to adopt, which ranged from 0 to 14. The most common number of strategies was one, with 76 hospitals committing to adopt just one strategy, 67 hospitals each outlined two to three strategies, 41 hospitals outlined four strategies, and 44 hospitals outlined 5 or more strategies.

How many strategies are hospitals implementing to address opioid abuse? N = 295.
Table 1 reports the results from our analysis of the number of strategies using negative binomial regression. In counties where uninsurance rates are higher, hospitals proposed new strategies at a lower rate (incidence rate ratio [IRR] 0.89; 95% confidence interval [CI] 0.79-1.00). Hospitals in the Northeast, as compared with the South, proposed new strategies at a higher rate in their most recent implementation plan (IRR 1.44; 95% CI 1.04-1.99). Hospitals in states with policies regulating pain clinics (IRR 1.37; 95% CI 1.05-1.77) and providing prescriber guidelines (IRR 1.25; 95% CI 1.03-1.53), as compared with hospitals in states without these policies, proposed new strategies at a higher rate. Hospitals located in states with funding for targeted risk education proposed new strategies to address opioid abuse at a lower rate than hospitals in states without this policy in place (IRR 0.82; 95% CI 0.68-0.99).
Negative Binomial Regression: Number of Strategies Hospitals Implement Associated With Opioid Use (N = 296).

Table 2 reports the focus of each hospital approach as well as hospital, community, and state policy characteristics. Nearly three-quarters of strategies proposed by hospitals (73%) were clinical in nature. More than three-quarters of hospitals (77%) proposed at least one strategy that was new, 41% of hospitals had an existing opioid-related strategy in place that they planned to either continue or expand. Slightly over half of all hospitals (54%) proposed a strategy that involved partnering with others in their community to address opioid abuse. See Supplementary Materials for examples of hospital programs in each category.
Descriptive Statistics N = 296.

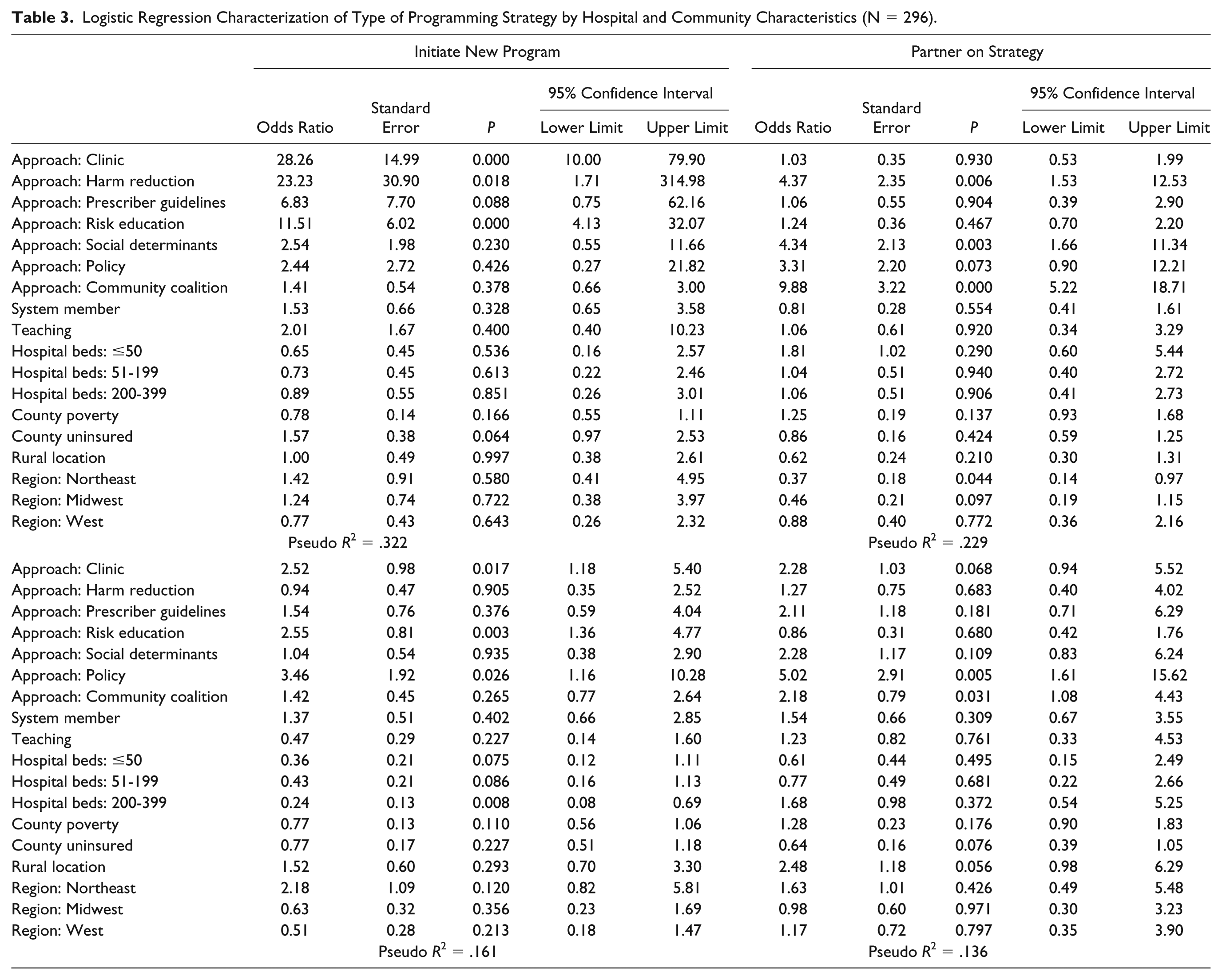
Table 3 reports the results from the four logistic regression models for each type of new strategy (new, existing, expansion, or partnership). We find that new programs proposed by hospitals have higher odds of being clinical (odds ratio [OR] 28.26; 95% CI 10.00-79.90), harm reduction (OR 23.23; 95% CI 1.71-314.98), or targeted risk education as compared with strategies that are not in these areas (OR 11.51; 95% CI 4.13-32.07). Hospital strategies that include partnering with another organization had higher odds of being harm reduction in nature (OR 4.37; 95% CI 1.53-12.53), focused on addressing social determinants (OR 4.34; 95% CI 1.66-11.34), or community coalitions (OR 9.88; 95% CI 5.22-18.71) as compared with other types of strategies. Hospitals in the Northeast were less likely to propose partnership strategies than hospitals in the South (OR 0.37; 95% CI 0.14-0.97). Hospital strategies that were a continuation of previous programs were more likely to involve policy advocacy (OR 5.02; 95% CI 1.61-15.62) or community coalitions (OR 2.18; 95% CI 1.08-4.43) as compared with other types of strategies. Hospital strategies that were expanded in the most recent implementation strategy were more likely to be clinical in nature (OR 2.52; 95% CI 1.18-5.40), offer targeted risk education (OR 2.55; 95% CI 1.36-4.77), or involve policy advocacy (OR 3.46; 95% CI 1.16-10.28) as compared with other types of strategies.
Logistic Regression Characterization of Type of Programming Strategy by Hospital and Community Characteristics (N = 296).
Discussion
Hospitals are developing a variety of programs to address opioid abuse, a critical health need in many communities in the United States. Through an analysis of hospital community benefit reports, we were able to identify patterns in the types of activities hospitals are likely to adopt and institutional, community, and state policy factors that relate to the implementation of different types of activities. Opioid abuse is a critical public health need nationally and therefore is an important test of whether hospitals are being encouraged to move beyond their traditional expertise in acute patient care to address critical population health needs.
The fact that most strategies related to opioid abuse were new suggests that many hospitals are responding to expanded community benefit requirements with novel strategies to address substance abuse. Still, 41% of strategies already existed and were either continued or expanded, suggesting that many hospitals were already addressing substance abuse to some extent. These hospitals potentially had successful strategies already in place that could simply be continued or expanded, or were not able to invest in developing new strategies related to substance abuse.
Overall, the strategies adopted by hospitals were most likely to be clinical in nature. Hospitals, in other words, may prefer to stick closer to their traditional expertise when committing to address local public health needs. The type of strategy selected varies, however, when looking at whether the strategy was new, existing, or primarily through a partnership. Harm reduction services were most likely to be new strategies or those carried out primarily with a community-based partner. This approach may suggest that hospitals are willing to develop new harm reduction initiatives as a result of the growing evidence base around the effectiveness of naloxone distribution and syringe exchange services.24-26 Hospitals were also more likely to engage in community coalitions and address the social determinants when partnering with other organizations. These findings suggest that hospitals feel more comfortable supporting such services when they are led by a community-based partner with more expertise in that area.
Our analysis of the number of strategies hospitals adopted revealed that most hospitals had at least one strategy to address opioid abuse. Several factors increased the rate at which hospitals adopted strategies, including regional location and state opioid policies. Hospitals in the Northeast adopted more strategies, potentially because opioid overdoses are the highest in this region. 27 Hospitals located in states with laws regulating pain clinics and prescriber behavior also adopted additional strategies, suggesting that states may provide important encouragement for hospitals to address critical health needs. Although our data do not allow us to investigate the extent of each strategy or their effectiveness, the number of strategies does represent a certain level of commitment to addressing opioid abuse. Up to a certain point, adopting a greater number of strategies could ensure that hospitals are able to intervene at multiple points, addressing opioid abuse through treatment services, preventive efforts, and harm reduction. It is possible that an extremely high number of strategies could indicate fewer resources invested in each strategy or potential duplication of efforts within an organization or community. Nonetheless, we argue that the number of strategies provides an important indication of hospital effort and investment to address opioid abuse.
Limitations and Future Directions
Our research approach has several limitations. For instance, while we are able to identify and assess different strategies in hospital implementation plans, we did not have the ability to verify the extent to which strategies are evidence-based or how many resources each hospital is willing to commit resources to a particular strategy. This information is important given the number of evidence-based interventions that exist for engaging individuals with opioid use disorders. Many of these evidence-based interventions have been implemented successfully in hospitals and could be a focus of community benefit efforts. Furthermore, implementation strategies only indicate an intention to complete a program and do not guarantee hospital fidelity to these plans. We should also note that having only one measure of hospitals and community characteristics is a limitation in that we are not able to see change over time or assess what might be causing an outcome. The ability to see what hospitals are doing over time can provide important insights to this policy-relevant area of study.
Based on our findings, we believe further research is needed on how markets (rather than individual hospitals) approach these needs collectively. We recognize that if one hospital is taking a particular approach, it may affect the likelihood of a neighboring hospital doing so as well, or of going in a different direction. Additionally, there may be effective partnerships between facilities or in conjunction with health departments that are not clearly conveyed within hospital implementation plans. In particular, follow-up qualitative studies are warranted to assess barriers to adopting new strategies, how hospitals make decisions to adopt one or more strategies, the extent to which strategies are evidence-based, and how strategies are evaluated after each CHNA cycle.
Public Health Implications
Our findings offer evidence that hospitals are taking steps to address critical health needs in their local communities. Variation exists, however, between hospitals and some factors may affect the potential effectiveness of strategies chosen and the robustness of hospital responses to address opioid abuse. The fact that institutional and state policy characteristics predicted involvement suggests that policymakers should consider ways to encourage hospitals with varying amounts of resources to address pressing health needs. Because of their unique position as anchors in many communities, hospitals may be an underutilized resource to develop and strengthen community-based initiatives to address opioid abuse and other critical health needs.
Footnotes
Acknowledgements
We wish to acknowledge Ciara Martin for her assistance constructing the dataset.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We also wish to acknowledge the Honors Tutorial College at Ohio University for supporting a summer research assistantship related to hospital programs to address opioid abuse.