
Abstract
Postpartum depression (PPD), self-reported in 11.7% to 20.4% of mothers, 1 is a serious illness that negatively affects both mothers and infants. For the mother, PPD can produce significant mental and physical symptoms that adversely affect her general quality of life, 2 work performance, and productivity. 3 For the infant, PPD can disrupt mother–infant interactions, bonding, feeding, and sleep, and interfere with scheduling/keeping well-child visits. 4 Given these adverse outcomes, and consistent with the US Preventive Services Task Force recommendation for depression screening, 5 it is important that providers screen for depression across the perinatal period and offer treatment, together with staff-assisted depression care supports, for women who are diagnosed.
Previous research has shown that PPD responds to antidepressants and psychotherapy.6-9 However, many women are unwilling to use these treatments because of postpartum-related or other barriers, such as concern about medication effects on nursing infants, lack of time, treatment costs, and social stigma. 10 Therefore, it would be helpful to have other treatment options for women who refuse or do not respond to traditional treatments.
Prior research has documented a positive relationship between social support and mothers’ postpartum mental health,11-18 so it seems possible that social support interventions might play an important role in PPD treatment and recovery. Two reviews on preventive therapy for PPD concluded that there was little evidence that prenatal group interventions 19 or professional or lay home visits 20 helped reduce the risk of developing PPD, although peer telephone support was recently found to be helpful for preventing PPD in a study of 701 at-risk Canadian women. 21 In studies that evaluated the benefit of support groups for the treatment of PPD, outcomes were also mixed.22,23
A form of one-on-one support that has been highly successful and well received by mothers is the labor doula. A review on labor doulas showed that this form of personal support shortens labor and decreases the need for cesarean deliveries, forceps and vacuum extraction, oxytocin augmentation, and analgesia. Eight of the 12 trials also reported early or late maternal psychosocial benefits.24,25
Postpartum doulas, an extension of labor doulas, provide in-home support and services to mothers after delivery. These services include emotional support, physical comfort, self-care, infant care, information, advocacy and referral, partner support, infant and sibling care, and household organization/work. 26 Therefore, postpartum doulas could potentially provide all or nearly all the 4 primary categories of social support previously described in the literature: informational, material, emotional, and comparison support, that is, help given by someone in a similar situation. 27 Furthermore, postpartum doulas can give this multidimensional support face-to-face, within a woman’s home—a known preference for depressed mothers. 28 There are currently no postpartum doula outcome data available, to our knowledge.
The purpose of this study was to pilot a peer support intervention trial for mothers with postpartum depressive symptoms. Specifically, we sought to test the feasibility of recruiting postpartum doulas, peer telephone supporters, and depressed mothers for a trial, and began to evaluate the impact of postpartum doula and peer telephone support as adjunctive treatments for depressive symptoms.
Methods
Participants
After approvals were given by the University of Minnesota and HealthEast institutional review boards, depressed mothers were recruited from October, 2009 to July, 2010, from 3 St. Paul hospitals, local practices, mothering Web sites, and Early Childhood and Family Education. Women who delivered at 3 community hospitals in St. Paul, Minnesota, were asked to complete a 2-question depression screen, and if positive, the 9-item Patient Health Questionnaire (PHQ-9), within approximately 24 hours of delivery. PHQ-9 negative women were given a flyer requesting their permission to be called in 2 to 4 weeks for a follow-up PHQ-9. Women with positive PHQ-9 scores from either of 2 these sources were informed of their positive score, referred to their primary care provider for usual depression treatment, and if eligible, invited to participate and consented.
Eligibility criteria included the following: English literate women, age 16 years and older, with a 0- to 6-month-old infant, living in the Minneapolis/St. Paul metropolitan area, and a positive PHQ-9 score (≥10). Figure 1 illustrates recruitment and other study procedures.

Flowchart of study progress
Randomization and Intervention
Women were randomly assigned to 3 groups: postpartum doula, peer telephone support, and a control group. Unblinded random assignment was performed by the support coordinator, who used random number tables. Women in the postpartum doula group were offered 24 hours of study-sponsored postpartum doula services by trained, certified doulas over 6 weeks (usually 4 h/wk).
Women in the peer telephone support group were offered telephone support over a period of 3 months, at times and frequencies preferred by the mother. Peer telephone supporters were unpaid volunteers who had previously had PPD and had recovered, and they were recruited through nurses, a parish nurse program, and study personnel. Calls were usually initiated by supporters.
All groups, including the control group, were mailed a PPD brochure and a PPD resource list that included contact information for support groups, classes, therapists, and other providers. We expected that women in all 3 groups would receive usual depression treatment from their health care providers and that our support interventions would serve as adjunctive treatment.
Supporter Training
Postpartum doulas were recruited through DONA (Doulas of North America) and CAPPA (Childbirth and Postpartum Professional Association), and had received standardized didactic and hands-on training and certification through these national organizations prior to the time of the study. In addition, the doulas and the peer telephone supporters received a study-sponsored half-day training session on PPD diagnosis and treatment, suicidal ideation, and techniques for supporting women with PPD. Support group meetings for study personnel were also offered periodically throughout the study, to give supporters opportunity to share their experiences and learn from one another.
Surveys and Measures
The survey measured demographic and work characteristics, social support, mental health, illness days, and health state today, a single-item global health measure taken from the EQ-5D. 29
Social support measures include available support, importance of support, and satisfaction with support. Available support is a 5-item scale that assesses how often various kinds of functional support (someone to confide in, get together with, help with chores, turn to for advice, and love you) were available, if needed. 30 Importance of Support, a 7-item scale created for this study, asks about mothers’ perceptions of the importance of emotional support from partner, family, and friends; help with childcare and housework; telephone support; educational support; and support group. Mothers were also asked about their satisfaction with these forms of support, as well as other types of support, including hired help with housekeeping and online support.
Mental health measures include the PHQ-9, history of mental health disorder (depression, anxiety, bipolar, schizo-phrenia, or other), postpartum and current depression/ treatment, duration of treatment, number of depression-related visits, CES-D (Center for Epidemiologic Studies–Depression Scale), and suicide ideation (from PHQ-9). In a recent study of 506 mothers of infants, the PHQ-9 had 82% sensitivity and 84% specificity for detecting postpartum (major) depression. 31 The 20-item CES-D has been widely used in research to measure change and response to depression treatment, 32 so was used here to measure mental health outcomes. Finally, surveys contained open ended questions or opportunities for making further comments.
Participants completed mailed surveys initially, and again at 3 and 6 months. Women who gave a positive response to a suicide ideation question (n = 9) were contacted by the principal investigator and were triaged and referred appropriately. Mothers received a $10 gift card for their participation.
Analyses
Descriptive analyses assessed participants’ demographic characteristics. Using intent-to-treat analysis, one-way analyses of variance were used to compare groups on general health, mental health, and social support at baseline and at 6 months, and to compare groups on 0- to 6-month change scores, in order to control for baseline group differences. Qualitative data were extracted and analyzed by undertaking a content analysis of responses, using NVivo9 software.
Results
Recruitment and Enrollment
Figure 1 illustrates the number of women recruited through various strategies, and participants’ progress through the study. Of 41 eligible women identified from hospital based flyers, our largest recruitment source, 22 (54%) agreed to participate. These women, together with 17 recruited from other sources (hospital screens, 9; midwife referrals, 3; Web sites, 2; Early Childhood and Family Education, 1), resulted in a total sample of 39 PHQ-9 positive mothers. Twelve participants were randomized to the postpartum doula group, 13 to the peer telephone support group, and 14 to the control group. Of the 39 enrolled mothers, 2 dropped out after the initial survey, 1 from the postpartum doula group and 1 from the peer telephone support group.
We also recruited 9 postpartum doulas and 9 peer telephone supporters; 3 of each dropped out before they were paired with a mother, leaving 6 doulas and 6 telephone supporters who worked with the 25 women assigned to the intervention groups.
Mothers’ Demographic Characteristics
Demographic characteristics for the group as a whole were as follows: mean age of 29.7 years (SD = 5.7); 37 (95%) white; 32 (84%) married; 17 (44%) had only one child; 29 (74%) had 4-year degree or more; 25 (66%) had a total family income of $20 000 to $79 999, and 10 (26%) had total family income of >$80 000. Thirty-four (87%) women had been employed during pregnancy, 29 (81%) were employed at 3 months, and 28 (78%) were employed at 6 months.
Support Provided Through Interventions
Postpartum doulas made an average of 6.9 (SD 2.6) home visits per assigned mother and spent an average of 23.4 (SD 8.1) hours with each mother overall. Services provided by postpartum doulas included education regarding infant care and feeding, practical support (eg, help with childcare, light housekeeping, and assistance with errands), and emotional support (eg, listening and affirmation).
Peer telephone supporters made an average of 5.6 (SD 4.6) calls per assigned mother, and spent a total of 1.06 (SD 0.99) hours, on average, in telephone conversation with each mother. Types of support provided through telephone calls included educational, emotional, and comparison support (provided by a person with similar experiences). The qualitative data suggest that phone calls might be more challenging to integrate into daily life, in comparison with the home visits made by doulas.
I really don’t have time for phone calls. Life is hectic. (3-month survey)
Baseline Group Comparisons
Baseline demographic and selected health characteristics categorized by group assignment reveal that a higher percentage of women in the postpartum doula group had a previous history of depression. There were also trends for more current depression and a lower health state among women in the postpartum doula group, and a higher level of education among controls (Table 1).
Baseline Group Comparisons on Demographic and Selected Health Characteristics
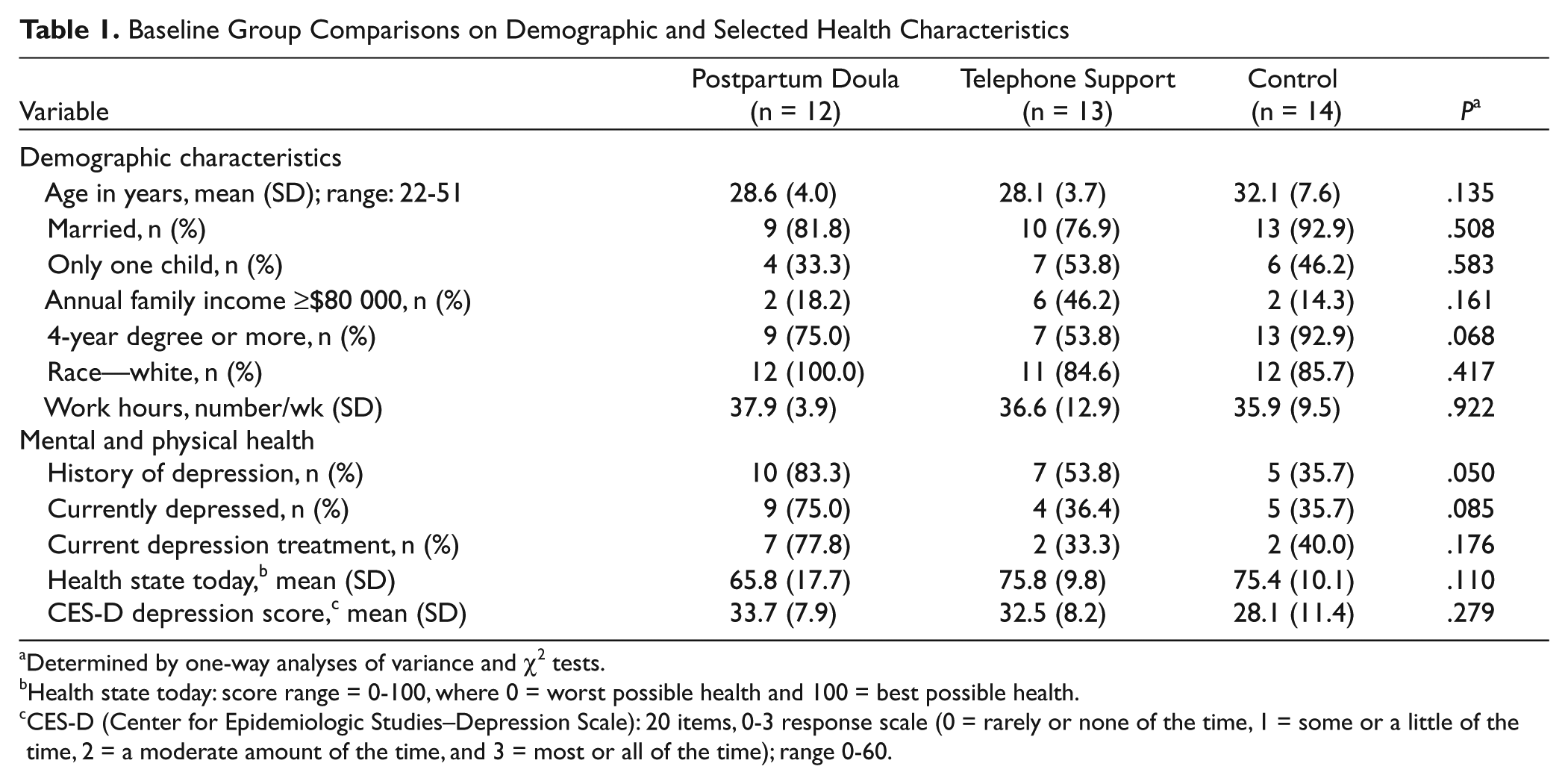
Determined by one-way analyses of variance and χ2 tests.
Health state today: score range = 0-100, where 0 = worst possible health and 100 = best possible health.
CES-D (Center for Epidemiologic Studies–Depression Scale): 20 items, 0-3 response scale (0 = rarely or none of the time, 1 = some or a little of the time, 2 = a moderate amount of the time, and 3 = most or all of the time); range 0-60.
Six-Month Group Comparisons
At 6 months, the postpartum doula group had a higher proportion of women who were currently depressed (82% vs 21% to 64%; P = .008) and currently receiving depression treatment (100% vs 25% to 50%; P = .019); in addition, their duration of depression treatment was longer (24 weeks vs 9-12 weeks, P = .003). There were no significant group differences in CES-D scores, general health, or social support at 6 months (Table 2).
Six-Month Group Comparisons on Health and Support

Differences were determined by one-way analyses of variance or χ2 tests.
CES-D (Center for Epidemiologic Studies–Depression Scale): 20 items, 0-3 response scale (0 = rarely or none of the time, 1 = some or a little of the time, 2 = a moderate amount of the time, and 3 = most or all of the time); range 0-60.
Available support: 5 items assessing how often various types of functional support (someone to confide in, get together with, help with chores, turn to for advice, and love you) are available; 1-5 scale (1 = none of the time, 5 = all of the time).
Importance of support: importance of emotional support from partner, family and friends; help with childcare and housework, telephone support, educational support, and support group; 6 items, 1-5 scale (1 = not at all important, 3 = somewhat important, and 5 = extremely important).
Overall satisfaction with support: single item, 1-5 scale (1 = very dissatisfied, 3 = somewhat satisfied, 5 = very satisfied).
The bold-faced entries in above table 2 are headings and significant p-values.
When group differences in 0- to 6-month change scores on health and support variables were investigated, the postpartum doula group showed greater (but nonsignificant) improvements in health state (change scores = 15.0, 3.6, and 8.1 for doula, telephone support, and control groups, respectively; P = .193) and CES-D depression scores (change scores = −16.3, −14.5, and −10.1; P = .397).
Satisfaction With Interventions
Satisfaction with study-sponsored support was greater in the postpartum doula group (mean 4.5, SD 0.7) than in the telephone support group (mean 3.2, SD 1.7; response scale 1-5; t = 2.514; P = .026; data not shown in table). The qualitative analysis showed high levels of appreciation and gratitude for the assistance provided by the doulas.
My postpartum experience has been the hardest thing I have ever had to deal with in my entire life. Yet despite all of the pain, sorrow, anxiety, guilt and sadness I refuse to give up hope that things will get better. I also want to thank (doula) for all of her support and hard work. It was a joy looking forward to her visit each week. As they say, PPD is temporary, treatable—I just wish the end result would come sooner. (3-month survey)
Participants described the doulas providing much emotional support alongside practical help, whereas the telephone peers provided emotional support with no practical help. This highlights the potential importance of emotional support in conjunction with practical assistance.
Having someone come to help was wonderful. It made getting through the week 100% easier just knowing someone was coming to help. (6-month survey)
It appeared that women were less satisfied with the telephone peer support, and that it might have been because of the lesser training of the phone peers, and the challenges in establishing rapport with some women over the phone.
I still feel unable to talk to peer not because of anything wrong with her, but I’ve never really voiced a lot of my feelings, especially to someone I don’t know. (3-month survey)
Discussion
Results of this study show that it is feasible to recruit certified, experienced postpartum doulas through national doula organizations, and peer telephone supporters through professional (eg, nurse) referrals. It is also feasible to recruit mothers with depressive symptoms for a peer support trial, though recruitment efforts for this particular study required a broad, multifaceted approach. In-hospital recruitment was more difficult than anticipated because of the low rate of positive PHQ-9 results (2.5%) in the immediate postpartum period. 33
Group differences seen at 6 months were unexpected: the postpartum doula group had a larger proportion of depressed women, women currently receiving depression treatment, and longer duration of depression treatment. These differences reflect baseline group differences (the doula group had larger percentage of women with a depression history), which suggests the presence of allocation bias, likely because of the small sample size. We hypothesize that the postpartum doula group was assigned more women with chronic depression, which would explain their persistent depressive symptoms. Although it may be difficult to distinguish PPD (onset within 4 weeks after delivery) from chronic depression (persistent major depression for at least 2 years) in the absence of an interview, chronically depressed women will eventually distinguish themselves by their protracted course and need for longer maintenance treatment. 34
Another explanation for the doula group’s greater prevalence and duration of depression treatment is that the doulas, who were trained to monitor mothers’ depression, reinforced the need for ongoing treatment. Indeed, in a previous PPD trial, depressed mothers who had regular care manager contacts appeared to be more aware of their depression diagnosis and more likely to receive treatment. 10
It is noteworthy that mothers in the postpartum doula group (vs telephone support and control groups) showed greater 0- to 6-month improvements in health state and depression scores, though these differences were not statistically significant. If one considers a 5% to 10% score change to be clinically meaningful, based on previous work suggesting that changes of 5% to 10% in health-related quality of life scores are clinical meaningful, 35 the doula group’s 0- to 6-month changes in health state and CES-D, as well as group differences in these changes, might be considered clinically meaningful.
Mothers who received postpartum doula support were significantly more satisfied with study-sponsored support than were mothers who received peer telephone support. Recognizing the previously demonstrated positive impact of telephone support on at-risk mothers, 21 there is reason to believe that postpartum doula support, with its more intense level of support and greater maternal satisfaction, might be even more beneficial for depressed mothers than telephone support. Further research is needed to determine exactly why mothers with doula support were more satisfied: For example, was this because of the in-home nature of doula support, the doulas’ greater training and experience, or the fact that doulas spent considerably more time with mothers (23.4 vs 1.1 hours)?
Peer telephone supporters reported difficulty contacting mothers, which, together with their inability to provide in-home practical support, may have contributed to the lower degree of satisfaction with this form of support. Other researchers have reported on the challenges of initiating and establishing contact between mentors/supporters and mothers, 36 so this concern should be taken into consideration when planning a peer support intervention study.
Strengths and Weaknesses
Strengths of the study include its randomized controlled design, longitudinal follow-up, use of general and mental health outcome measures, evaluation of both quantitative and qualitative data, and most important, evaluation of postpartum doula support (not previously studied, to our knowledge), which, if proven cost-effective, could conceivably be funded by insurers.
Weaknesses of the study include its small sample size (though this was designed as a pilot study) and thus limited ability to detect certain group differences, selection bias (resulting in a homogenous sample, which impairs generalizability), allocation bias (producing baseline group differences), use of a self-assessment tool (PHQ-9) for PPD diagnosis, and differences in the amount of support provided by the 2 interventions. In addition, more than half of participants had had a history of a mental disorder, so it is possible that several of our cases represent chronic depression, rather than true PPD, making it more difficult to assess the benefit of various treatments or interventions. We recommend that the potential benefit of postpartum doula support for PPD be evaluated in a larger randomized controlled trial that includes a more diverse sample, and either excludes or controls for women with chronic depression.
Conclusions
We found that it is feasible to recruit postpartum doulas, peer telephone supporters, and depressed mothers for a peer support intervention trial. Study results showed greater maternal satisfaction with postpartum doula vs. peer telephone support. We recommend a larger follow-up trial to investigate the benefit of postpartum doula support for PPD.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by a Grant-in-Aid from the University of Minnesota Graduate School.