
Abstract
Keywords
Although diabetes self-management education is a cornerstone of diabetes care, 1 only about half of patients with diabetes receive formal diabetes education. 2 Patients who are poor or underinsured, who come from racial/ethnic minority groups, who live in rural communities, or who have limited literacy skills frequently receive inadequate diabetes education.3-7
Providing education and counseling in resource-poor community clinics, where many low-income patients seek care, is challenging.4,8,9 These clinics often have fewer financial resources and commonly lack funds to formally train staff to provide comprehensive diabetes education.10-12 If patient diabetes education materials are available, they are often written at too high a level for vulnerable populations, and they tend to aim at increasing patients’ knowledge rather than helping them set goals and change behavior. 13
The purpose of this pilot study was to evaluate the implementation of a literacy-appropriate diabetes self-management intervention in resource-poor community clinics. Since the intervention was designed to engage patients in the process of behavior change, our primary outcome was patients’ success setting and achieving behavioral goals.
Methods
Setting
A pilot study was conducted between August 2009 and August 2010 in 3 federally qualified health centers, which are federally supported clinics that provide medical care to patients regardless of insurance status. Nationally, federally qualified health centers are engaged in a Health Disparities Collaborative to improve chronic disease management; the most frequent target of the collaborative is diabetes control.8,10,14
The study protocol was approved by the Institutional Review Board at our institution.
Training and Intervention
Three part-time nonmedical research assistants (RAs) were based in each clinic. A fourth RA, located at an academic medical center helped perform telephone follow-up. All RAs were college graduates. Each received a 2-hour training session focused on teaching core diabetes principles using information contained in a patient diabetes guide, as well as skill building in facilitating patient-centered goal setting for behavior change.13,15-19
The intervention was structured around a diabetes self-management guide, Living With Diabetes: An Everyday Guide for You and Your Family (http://www.acpfoundation.org/hl/diabguide.htm). The guide, written at a fifth-grade level, uses simple language and descriptive photographs to teach core diabetes concepts and empower patients to engage in health behavior change. It covers 5 topics: diet, physical activity, blood glucose monitoring, medication adherence, and insulin use.13,18,19 The accompanying goal-setting technique calls for facilitating a patient’s creating an action plan, or a short-term, easily achievable behavioral plan. The technique stresses that it is the patient who chooses a specific behavioral goal; that is, the RA acts as a coach helping the patient fine-tune a specific strategy for reaching the goal (eg, “I want to lose weight” becomes “I will walk 2 blocks after work 3 times next week”). The action plan must be short-term (eg, 1-2 weeks) and easy to achieve, thus avoiding the “failures” that frequently discourage future attempts at behavior change. Patients rate their confidence in their ability to achieve their action plan using a scale from 0 to 10; if lower than 7, the RA helps them further refine their plan to make it more achievable. 16
Recruitment and Protocol
Participants were English-speaking adults 18 years and older with a diagnosis of type 2 diabetes. All were receiving ongoing primary care at 1 of 3 participating federally qualified health centers and had regular access to a telephone. Clinic nurses referred patients waiting for appointments with their primary care provider to the RA; 50 (17%) declined to participate. A total of 247 patients were enrolled in the study.
After a structured interview to determine demographics, the RA introduced the guide pointing out key diabetes self-management principles and calling attention to the worksheet at the end of each chapter designed to facilitate behavior change. The RA then asked participants, “Is there anything you are willing to do next week to improve your health?” After a participant identified an area, the RA coached him or her in creating an action plan and recorded it verbatim. This education and coaching framework was designed to be completed in 10 to 15 minutes. Two telephone follow-up calls were conducted: one at 2 to 4 weeks and one at 6 to 9 weeks. All calls were initiated at the academic medical center. Patients at the city clinic were called by the RA who had facilitated their initial action plan. Patients in the 2 distant rural clinics were called by a fourth RA, who had no previous contact with the patient due to cost constraints.
During the follow-up phone call, participants were asked if they (1) remembered receiving the guide, (2) recalled their action plan, and (3) achieved and/or sustained their action plan. If participants did not remember their action plan, the RA would remind them of the domain (eg, diet). If this failed to trigger the participant’s memory, the RA would read the action plan created by the participant. RAs coded success with action plans as one of the following: completely achieved and sustained, completely achieved but not sustained, action plan not achieved but engaged in some behavior change, or no behavior change.
At each contact, RAs encouraged participants to make a new action plan or extend their current one and recorded the new plan verbatim. The second follow-up call assessed recall and completion of the second action plan.
Data Analysis
The proportion of participants who recalled their action plans and who were successful with their plans at each of the 2 follow-up calls is described. Differences in follow-up, recall, and success rates are compared with χ2 tests. Data on challenges and successes, to facilitate further dissemination of the intervention and describe these results quantitatively and qualitatively, were systematically collected.
Results
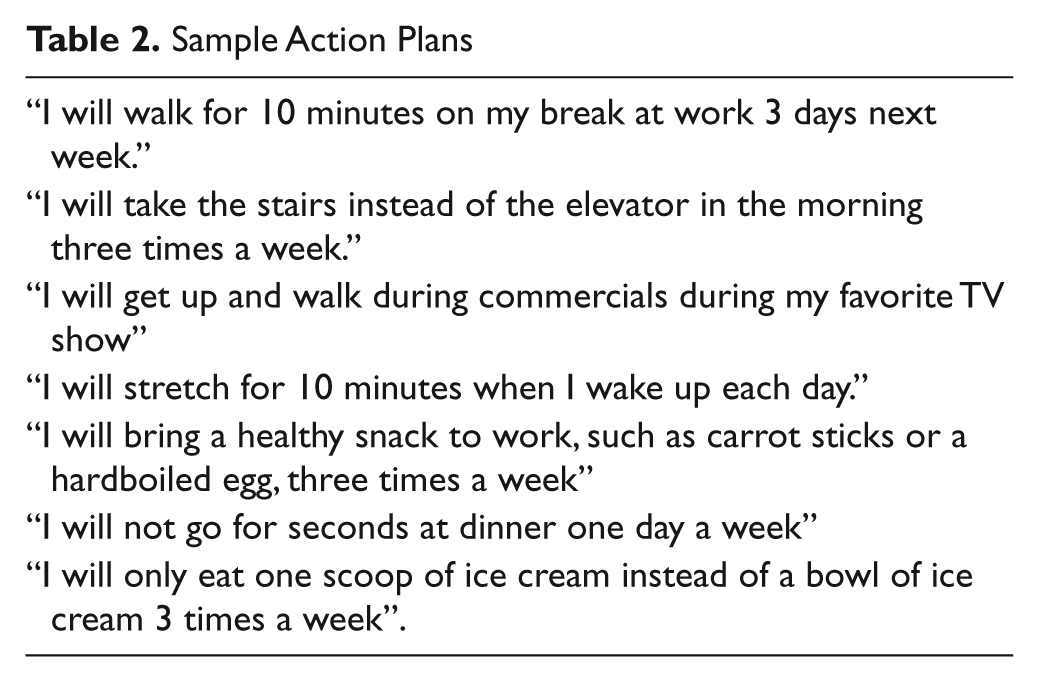
Participants were predominantly female, African American, and uninsured and ranged in age from 18 to 86 years (Table 1). The initial self-management support session took an average of 15 minutes, with a range of 9 to 20 minutes. All participants generated an initial action plan (Table 2). Most focused on physical activity (66%) or diet (31%); 7% chose to focus on monitoring blood sugar more closely; and 2% chose to focus on medication management.
Patient Characteristics a
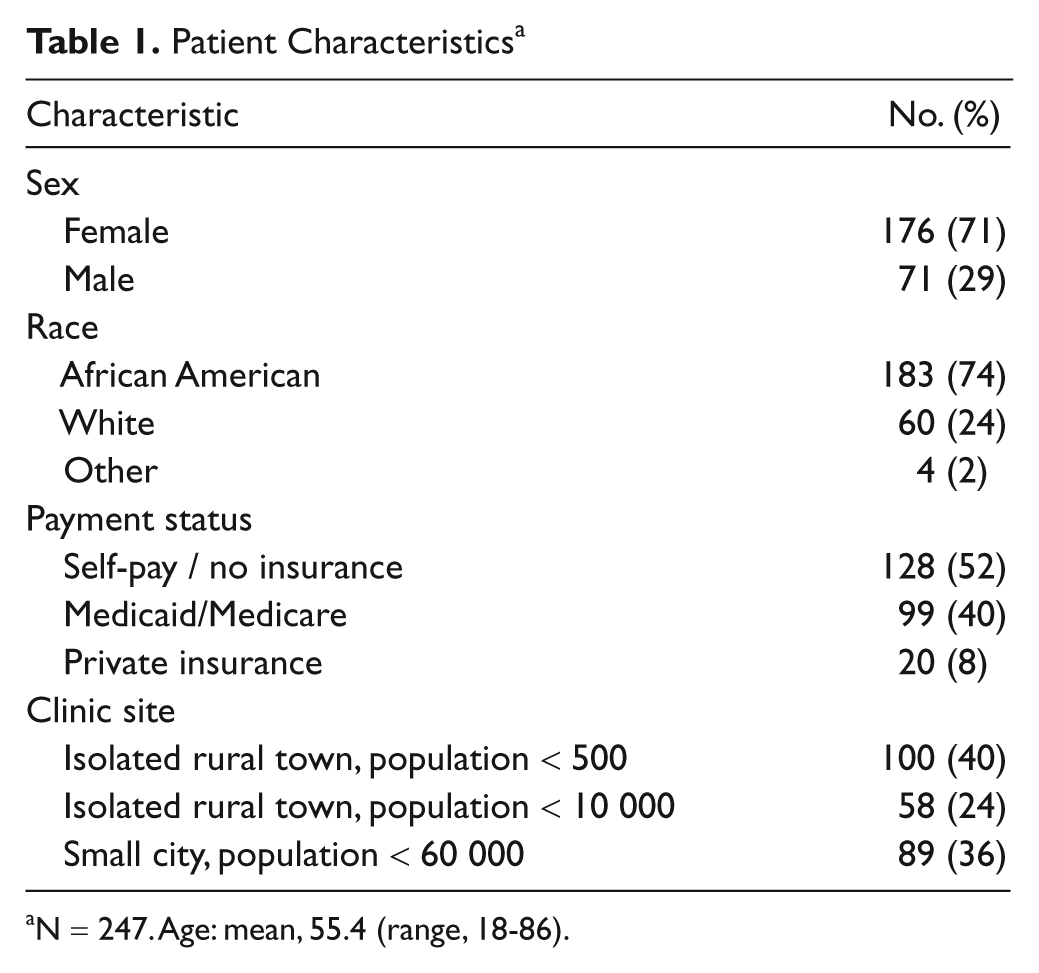
N = 247. Age: mean, 55.4 (range, 18-86).
Sample Action Plans
We were unable to reach 44 participants for the initial follow-up call; 3 withdrew informed consent. Of the remaining 200 participants, 95% remembered receiving the guide, and 86% reported that they had reviewed the guide at home. Participants were most likely to report that the diet and physical activity chapters were helpful (80% and 67%, respectively). Approximately half (54%) found the remaining chapters helpful (blood glucose self-monitoring, insulin use, and medication adherence). Two-thirds (68%) recalled their action plan, and 84% of these reported achieving it. Eighteen percent declined to make a new action plan, generally preferring to continue work on their original plan. In addition, 31 participants (15%) chose not to continue the study; all were from the rural federally qualified health centers in which follow-up telephone calls were made by an RA whom they had not met face-to-face.
Approximately half (n = 104) the participants who completed the first call were reached for the second follow-up call; 13% of these chose not to continue. All of these participants were called by an RA whom they had not met. Of the 90 participants who completed the second follow-up session, 79% recalled their action plan from the previous call—80% of these reported achieving it and 58% made a new action plan.
At the end of the study, 62% of the 247 participants initially enrolled reported some behavior change, and 54% reported completely achieving and sustaining behavior change. Participants who recalled their action plan were more likely than those who did not recall it to make a subsequent action plan (92% vs 65%, P < .0001). The follow-up calls were completed in 5 to 10 minutes. The median number of attempts per completed telephone interview was 3 (range, 1-8).
Discussion
Participants in our pilot study responded positively to self-management support in the clinic with nonmedical personnel using the patient-centered guide and action plan framework. As in previous studies using diabetes action plans, participants most frequently chose to focus their action plans on diet and exercise.18,19Although telephone follow-up was challenging, patients who participated were likely to report behavioral changes.
Attempts to contact participants were time-consuming, and ongoing engagement was difficult if follow-up was conducted by an RA with whom they had not had face-to-face contact. This suggests that self-management strategies in resource-poor settings may benefit from making patient contact during office visits.
Limitations
The limitations of this pilot study included a lack of control group, low follow-up rate, and self-reported outcomes. Longer-term studies are needed to determine effects on glycemic control and diabetes-related complications.
Conclusion
Many diabetes education interventions studied in urban academic settings would be difficult to implement in rural and/or resource-poor settings.10,12,20 This pilot study provides important insight into initiating brief diabetes self-management strategies in resource-poor community clinics. We found that using the self-management guide and action plan helped focus participants on behavioral change, particularly during the initial visit. However, continued follow-up and engagement were challenging. It is important to continue to explore creative methods that are feasible to implement in resource-poor clinics to help low-income, uninsured patients remain engaged in the behavior change process.
Footnotes
Acknowledgements
We would like to acknowledge Willie White, Emma Tarver, Rosie Kye, and Dr Larry Daniels for their willingness to participate in clinical research to investigate strategies to implement diabetes education in their clinics. We appreciate David Neal in Sicily Island and Annie Miller, BSW, in Tallulah for their skill in counseling patients to make achievable action plans.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Office of Minority Health. The American College of Physicians Foundation supported the Living With Diabetes self-management books and video training tool (Ready, Set, Action Plan: How to Effectively Use the Diabetes Guide).