
Abstract
Keywords
As adolescents transition from childhood to adulthood, they engage in many risk-taking behaviors that lead to preventable morbidity and mortality.1-3 Therefore, the annual physical examination for adolescents is a perfect opportunity for primary care providers to offer preventive services such as to counsel adolescents about abuse, depression, suicide, and violence, as well as to determine their risks for sexually transmitted diseases (STDs), pregnancy, cigarette smoking, and use of recreational drugs. However, adolescents are well known to have poor adherence to their annual health assessment.4-6 McInerny et al reported that annual adolescent visit rates were only 34% compared to 59% to 60% for infants and 3- to 6-year-old children. 4 As a result, many adolescents are missing out on important preventive services.
Many factors prevent adolescents from seeking health care.7-13 Both qualitative and quantitative data exist that assess why adolescents do not seek health care when they should. However, most of these studies target specific barriers such as access to confidential care or mental health services or lack of knowledge of rights to health care and do not include the array of barriers adolescents may encounter when seeking health care. Further, none of these studies targeted the barriers encountered by adolescents who were already in a health system such as adolescents who have insurance, who have identifiable primary care providers, and who have been regularly attending health centers. Thus, some insights into these barriers may guide health care providers and policy makers to develop health systems that could improve adolescents’ adherence to health services.
The purpose of this study was to determine from adolescents who were already using a health care system about (1) their perceptions of barriers to obtaining health services, (2) their views on how to overcome the barriers, and (3) their views on how to create an adolescent-friendly primary care practice.
Methods
Study Population
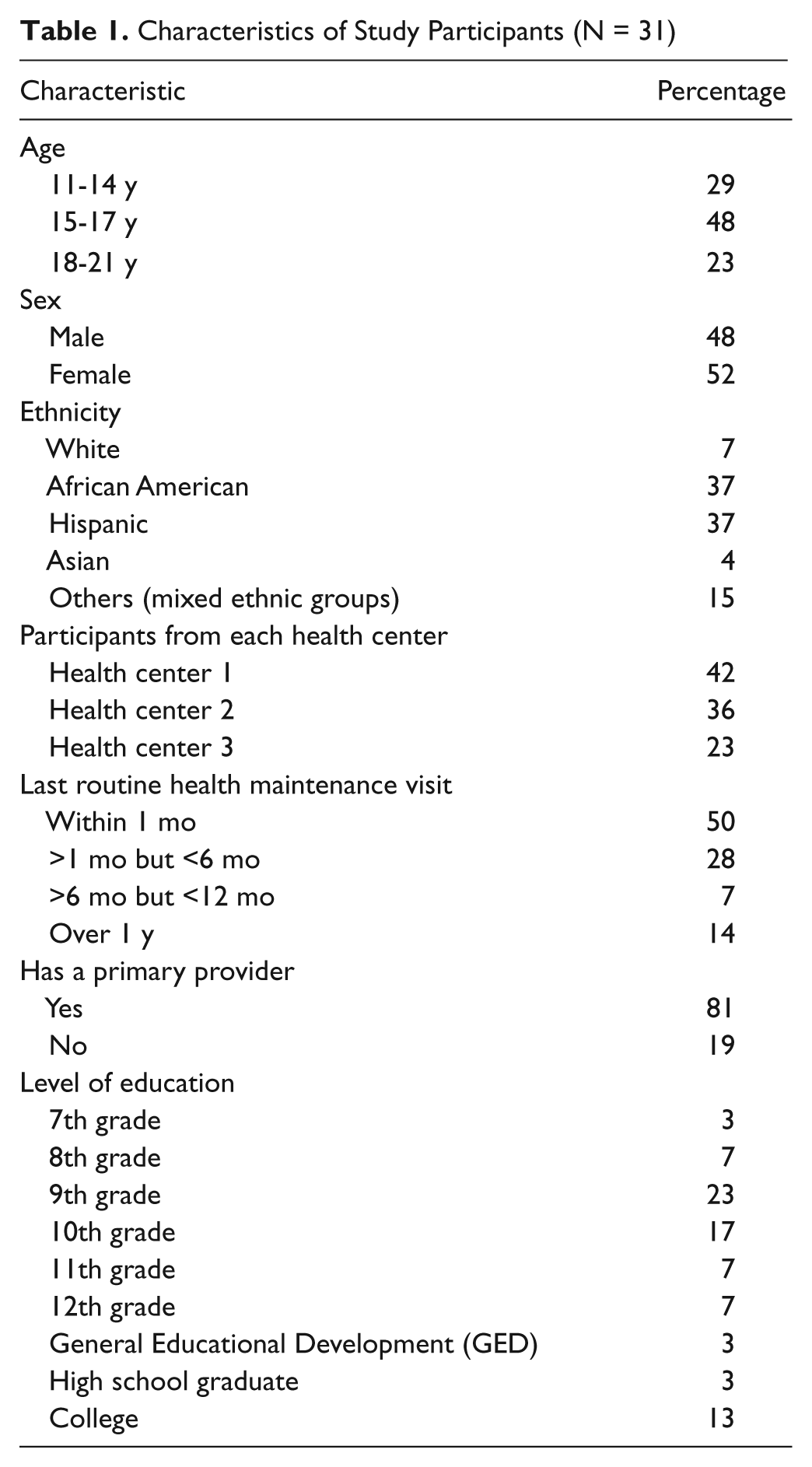
Adolescents, 11 to 21 years old from 3 health centers in the Bronx, were recruited to participate in focus groups when they came for a scheduled appointment. The majority of adolescents who utilize these health centers are of Hispanic and African American and many are from low income families.
Two focus groups were conducted at each center for a total of 6 focus groups. Focus groups were stratified by age: 11 to 14 years old, 15 to 17 years old, and 18 to 21 years old. The rationale for stratification was based on the assumption that younger adolescents might be intimidated by the presence of older adolescents in a group discussion. Each participant received $10 plus food and transportation expenses.
Measures
A set of questions was developed by the authors to guide the discussion and to ensure a similar agenda was followed at each focus session. Open-ended questions were used to invite group discussion. Some were formatted as vignettes so that participants would not feel threatened when the question dealt with sensitive issues. The questions were field tested with a group of 5 adolescents aged 15 to 17 years old prior to conducting the actual focus groups. A total of 8 questions covered the following domains: (1) discussing barriers to accessing health care such as insurance, language, transportation, and making an appointment and their thoughts on how to overcome these barriers; (2) identifying barriers related to issues of consent and confidentiality; (3) exploring barriers to accessing mental health and related issues; and (4) defining key elements of an adolescent-friendly office. A moderator (an investigator) who was experienced in focus studies led the discussion at each meeting. Further, two additional investigators were present at each session to take notes and to discuss each focus session. The discussions were audio taped with the permission of the focus group participants. The sessions lasted approximately an hour. The study was funded by an American Academy of Pediatric Community Access to Child Health (CATCH) grant and approved by the Institutional Review Board of Montefiore Medical Center.
Data Analysis
A professional consultant transcribed audiotapes from all 6 focus group discussions. The 3 investigators who were present at each of the focus sessions generated multiple themes from focus group discussions. In addition, a consultant who is an expert in qualitative studies independently recoded the transcribed materials into multiple themes and frequencies. Frequency was then reported as “most” or “many” and “some” or “few.” One of the 3 investigators (the principal investigator) who was present at the focus session then reviewed the themes and frequencies developed by the consultant for accuracy and consistency with the themes developed by the investigators. Any discrepancies between the 2 themes were then rediscussed and re-reviewed among the 3 investigators. Quotations were selected from the transcripts to illustrate certain themes. To the extent possible, we attempted to compare and contrast the age groups, older adolescents (18-21 years old) and younger adolescents (11-17 years old), and to analyze differences among groups from each of the 3 health centers.
Results
Demographic Data of Participants
Thirty-one adolescents, aged 11 to 21 years old, participated (Tables 1 and 2). Fifty percent of them reported a routine visit to their primary care provider within the past month.
Characteristics of Study Participants (N = 31)
Focus Group Participants

Barriers to Accessing Health Care
Most adolescents reported experiencing barriers to making an appointment, saying they were told the next available was 4 weeks or longer. Additionally, they complained about waiting more than an hour to be seen by providers on the scheduled appointment day. In fact, this was one of the strongest reported deterrents to visiting a physician, and they suggested that there should be more providers at the centers. The following quotations illustrate their experiences:
“I don’t like going to see my doctor . . . ’cause we just wait too long.” (male teen) “Yeah . . . they put you in a room, or whatever, and then they tell you . . . yada, yada . . . and then you sit there for, like, another 20 minutes wondering where the doctor is. Like, the other day, I came, and I was sick, and I waited there half an hour in the lobby . . . . Then I waited another 20 minutes in a room, and she said, ‘Drink water.’ If I wanted to drink a lot of water, I could have done that.” (male teen) “Just recently, I called for an appointment in June or July, and they said I had to wait to December.” (male teen)
Most adolescents denied experiencing barriers related to insurance, language, or transportation to their site of heath care. No differences were found when the results were compared by age and by health center.
Barriers Related to Issues of Consent and Confidentiality
In this study, many younger adolescents (17 years old and younger) were not aware of their rights to receive care related to pregnancy, STDs, and drug use without their parents’ knowledge or consent. Further, most of them (both younger and older adolescents) did not trust their providers to keep these issues from their guardians. The following quotations illustrate their expectations:
“And if the doctor doesn’t ask them to leave, I can’t tell my mom to leave. She’s going to be like, ‘What you going to do that I can’t be here?’” (female teen) “I feel like if my mom goes up to my doctor and asks her, ‘Is my daughter a virgin?’ she’s going to tell her.” (female teen)
However, some adolescents reported that if they know the physicians well, then they might discuss these issues.
Barriers Related to Mental Health
Many adolescents reported that they would not discuss with their providers issues such as feeling depressed or thoughts of hurting themselves. They felt that their primary providers had little interest in this topic and limited knowledge about it. The following are typical quotes:
“Don’t feel medical providers are knowledgeable about mental health.” (female teen) “They wouldn’t understand it.” (male teen) “They really don’t know what to do about it. They know about your body, but they don’t know much about your mind.” (female teen) “The counselor knows what he or she’s doing more than the doctor does.” (male teen)
Instead, many adolescents felt more comfortable discussing these issues with mental health professionals, such as counselors. No differences were found when the results were stratified by age and health center.
Visions of Adolescent-Friendly Offices
When adolescents were asked what they would want if they were to design an office they would like to go to, almost all adolescents said they wanted a separate waiting area from children, friendly staff members, entertainment units, and food. The following quotations illustrate their expectations:
“I think that . . . there should be, like, a separate space for the teenagers and separate thing for the little kids.” (female teen) “There’s so much noise with a lot of kids crying, and you got the mothers yelling . . . and it is very irritating.” (male teen)
Discussion
In this qualitative study, almost all participants in the focus groups reported experiencing barriers in making an appointment in general or getting an early appointment with their providers. These problems may be related to an inadequate supply of staff to meet the demand or inefficiencies in systems operations, a challenge for health care administrators. Contrary to our expectation that adolescents would rather discuss mental health problems with physicians they know than with strangers, we learned that many of these adolescents preferred to talk with mental health specialists. This finding should be followed up in view of current recommendations that in order to compensate for the shortage of mental health providers, primary pediatricians should provide mental health services to adolescents.14,15
Issues of confidentiality and trust in the providers were revealed as key barriers to access in this study. Similar findings have been reported elsewhere.16-18 However, some of our adolescents reported that they might confide in their physicians if they knew them well, a point that underscores the importance of continuity of care in the ambulatory setting.
We also learned that many of the younger adolescents in our study were unaware of their right to receive care in certain health situations without their parents’ consent. This finding reinforces the importance of clinicians informing youth and their parents about confidentiality of care at visits starting with the earliest stages of adolescence and repeated at every opportunity.
When these adolescents were given the opportunity to design an office that they would like to attend, they were very definite about wanting a facility where they would be treated with respect, kindness, and privacy. Further, they wanted to be entertained and occupied with activities while waiting to receive care.
This study uses a convenience sample of adolescents who are already in the health care system, and some of the findings may not be generalizable to all adolescents.
Conclusions
Even adolescents who had health insurance, were registered for care in a system, and already had primary providers still reported barriers to accessing needed health services. Therefore, it is not enough that adolescents should have identifiable providers and be in the health care system, but it is also important to understand how the system could be accessible. An additional important finding is that many adolescents in this study were uncomfortable discussing mental health issues with their providers, a matter that raises concerns and should be looked at further in future studies. If changes are going to be implemented to better serve the adolescent population, it is important to listen to the views of adolescents and seek their opinions on what they consider to be barriers to accessing health services and what they consider to be an ideal health center.
Footnotes
Acknowledgements
We would like to thank Maya Ilowite (medical student from Albert Einstein College of Medicine) for her help with recruiting study participants. We are also grateful to Dr. Katherine Lobach and Dr. Celia Alfalla for their advice on the development of the project and the writing of the manuscript.
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) declared the following financial support for the research, authorship, and/or publication of this article. This research was funded by the American Academy of Pediatrics Community Access to Child Health (CATCH) grant.