
Abstract
Abdominal aortic aneurysms represent both an individual risk of mortality and a socioeconomic burden for health care systems worldwide, but screening is not performed in all countries. Here, the authors summarize the pros and cons of screening to reduce abdominal aortic aneurysm–related mortality.
Background
Abdominal aortic aneurysm (AAA) is defined as a focal dilation to more than 150% of the normal transverse diameter of the abdominal aorta 1 or, more recently, as a maximum diameter of more than 3 cm.2,3
Abdominal aortic aneurysms represent both an individual risk of mortality and a socioeconomic burden for health care systems worldwide as they occur in 4% to 8% (Table 1) of the male and 1.3% of the female population over 65 years. 4 The most dangerous complication is rupture, representing a surgical emergency with a mortality rate of 50% to 70%. Ruptured AAAs rank at the 15th, even at the 10th, position of the most common causes of death in the United States in men older than 75 years. 5
Prevalence of Abdominal Aortic Aneurysms in Previous Randomized Screening Studies

MASS, Multicentre Aneurysm Screening Study; US, ultrasound; NA, not applicable.
Risk of Rupture and Risk Factors
The best established risk factors for the development of an AAA are increased age and a positive smoking history6,7 (90% of all AAA patients have a history of smoking). 4 Positive family history,8,9 male gender, 6 coronary artery disease, 7 arterial hypertension,7,10 arteriosclerosis, 7 hypercholesterolemia,6,7 and cerebrovascular disease 11 have been reported as risk factors. Recent genome studies showed that a genotype of rs7025486[A] in the DAB21P gene (a variant on chromosome 9p21) is associated with a 20% risk increase for AAA. 12 However, routine testing for this genetic variant is not routinely available at present.
Currently, the maximum transverse diameter is the most important clinical risk determinant for AAA rupture (Figure 1).1,13 Rapid expansion rates (more than 5-10 mm/y) are also associated with an increased risk. 2 Smoking has been found to accelerate aneurysm growth. 3 Other factors enhancing the risk of rupture are female gender, arterial hypertension, a positive family history, and certain morphological forms of the aneurysm. 14
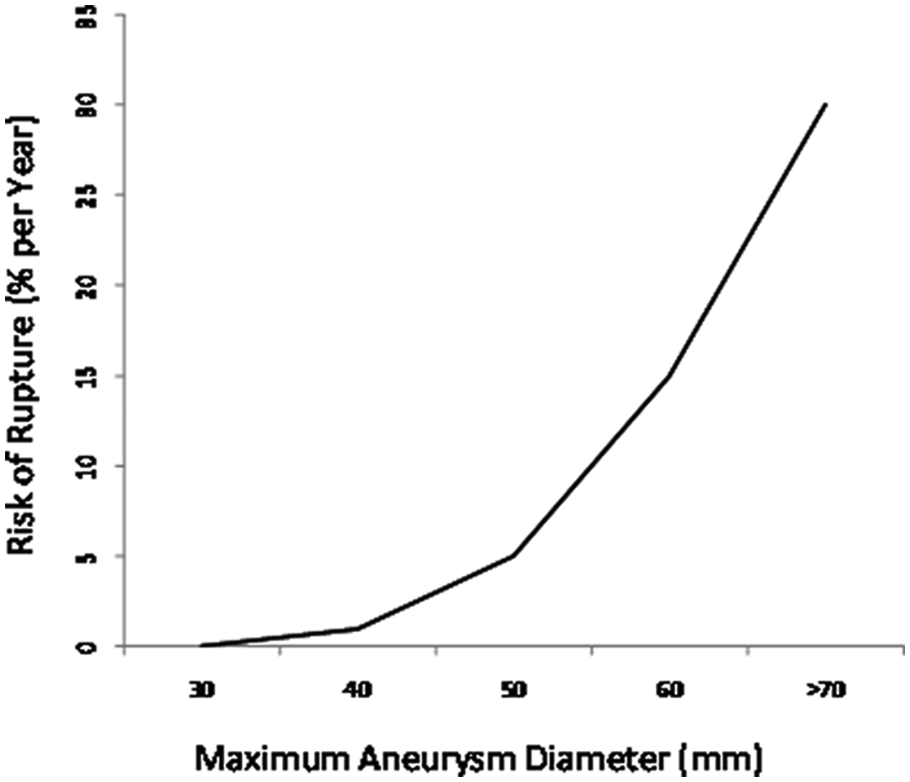
Risk of aneurysm rupture. 2
Screening Techniques
Ultrasonography represents a widely available, inexpensive and noninvasive safe procedure to detect AAAs. With a sensitivity of 87.4% to 98.9% and specificity of 99.9%, ultrasonography has a good diagnostic value. 15 The maximum aortic diameter should be assessed from both a transverse and a longitudinal section (Figure 2). No final agreement exists on whether the maximum external or the internal diameter of the aneurysm should be assessed. Although the threshold of 55 mm for the recommended treatment of AAAs relates to the external diameter, 16 and the majority of screening trials was also based on this parameter, the largest population-based trial, the Multicentre Aneurysm Screening Study (MASS), referred to the maximum internal diameter. 17 Ultrasonography also allows for evaluation of the topographic relation to the renal, mesenteric, and iliac arteries, and the size of both the intraluminal thrombus and the arterial wall can be studied.
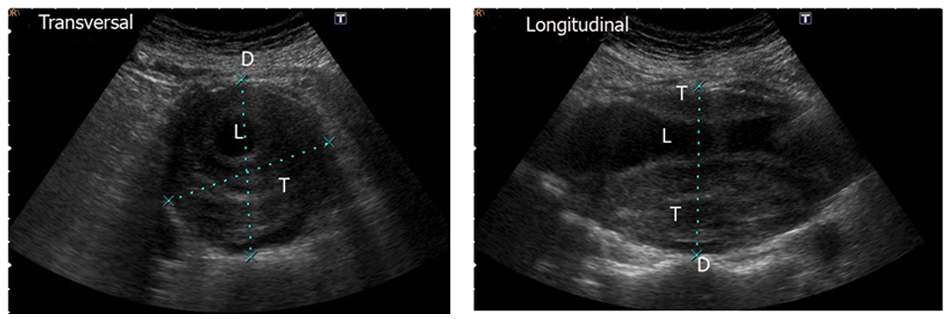
Transverse and longitudinal section of an infrarenal abdominal aortic aneurysms. D, diameter; L, lumen; T, thrombus.
Other diagnostic procedures, including contrast-enhanced computerized tomography and magnetic resonance imaging, are not recommended for screening of AAAs because of their higher costs, less availability, potential adverse reactions against contrast media, and radiation exposure for computerized tomography.
Evidence of Screening Studies
To date, 4 randomized population-based AAA screening trials have been performed: the Chichester trial, 18 the MASS, 17 the Western Australia trial, 19 and the Viborg trial 20 (Table 2). All 4 were randomized into a group that was offered ultrasound screening for AAA versus a group that was not offered abdominal imaging. The mean odds ratio in favor of screened men concerning aneurysm-related mortality was 0.6 (95% confidence interval, 0.47-0.78). 21 However, all cause mortality was not reduced, and no benefit of screening was found for women. Current guidelines recommend a 1-time ultrasound screening for men at the age of 65 years.2,22 Screening at age 60 years in men may be considered if risk factors like a positive family history or positive smoking status apply.
Evidence of Screening Studies
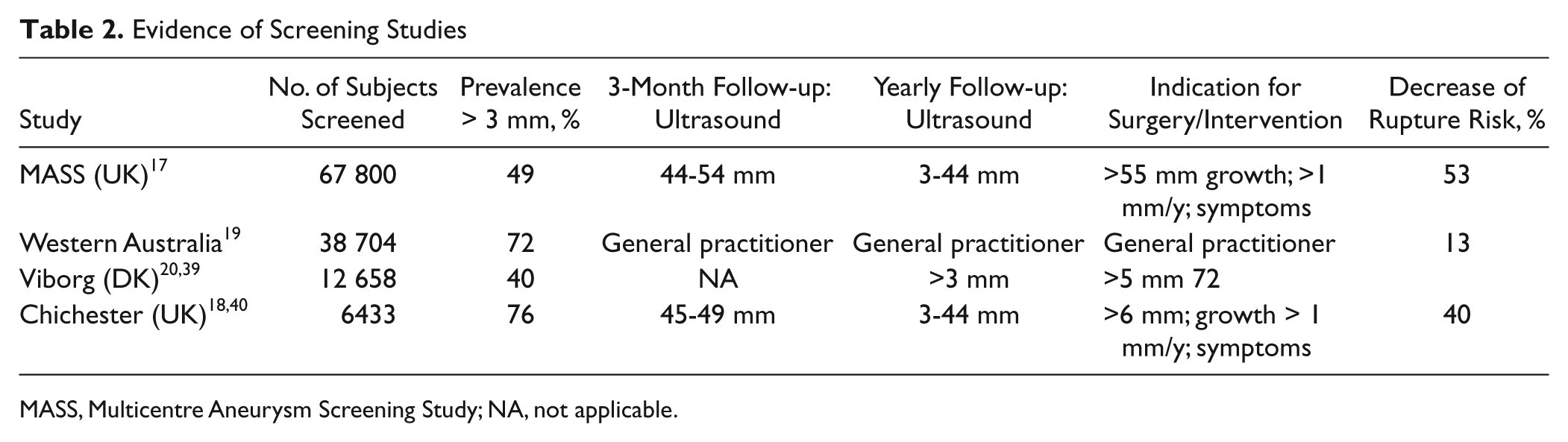
MASS, Multicentre Aneurysm Screening Study; NA, not applicable.
Management of Patients With AAAs
The management of patients with known infrarenal AAAs should balance the risk of rupture against the risk of treatment, taking into account the general medical condition and life expectancy of the individual. Because of the negligible risk of rupture for aneurysms smaller than 40 mm, general consensus exists that affected patients should be included into a surveillance program. Two small aneurysm trials, the American Aneurysm Detection and Management trial and the UK Small Aneurysm Trial, randomized open surgery versus surveillance of AAAs 40 to 54 mm (American Aneurysm Detection and Management) or 40 to 55 mm, respectively. A recently published meta-analysis of these trials concluded that early surgery was not beneficial for patients with aneurysms 40 to 55 mm in diameter. 23 Also, an early endovascular repair showed no benefit for patients with small aneurysms. 24 Guidelines from the American Heart Association 22 and from the European Society of Vascular and Endovascular Surgery 2 recommend surgical treatment of aneurysms ≥55 mm in diameter or if a diameter increase >10 mm per year is observed or symptoms develop. 2 A threshold of 52 mm may apply for women. 2
Management of Patients With Small Aneurysms
All patients with aneurysms 30 to 55 mm in diameter should undergo periodic sonographic follow-up. Although the optimal follow-up interval still needs to be established, consensus exists that the maximum diameter has to be taken into account when planning the next visit. For the MASS and Chichester trials, follow-up intervals of 3 months applied for aneurysms 45 mm or larger, whereas intervals of 1 year were considered sufficient for smaller aneurysms.17,18 Based on the population of the UK Small Aneurysm Trial, Brady et al recommended intervals of 36, 24, 12, and 3 months for aneurysms 35, 40, 45, and 50 mm in diameter, respectively. 3
Previous investigations have demonstrated a higher probability of cardiovascular events in patients with AAA. 25 However, optimal medical treatment of patients with AAA is also important with respect to aneurysm progression. Although there is good evidence that the concentration of total blood cholesterol is associated with the presence of AAA, 26 no direct association between serum cholesterol and aneurysm expansion has been established.3,27 A recent meta-analysis found a protective effect of HMG-CoA reductase inhibitors (statins) concerning aneurysm growth in addition to its cholesterol-lowering effects, which may be associated with pleiotropic effects of statins, such as reduction of matrix metalloproteinases, as well as antioxidative and anti-inflammatory effects. 28 The same anti-inflammatory effect is postulated for angiotensin-converting enzyme inhibitors for which a growth inhibition has been demonstrated in animal models. 29 However, there is no proof for a corresponding effect in humans yet, only patients deemed unfit for repair may profit from angiotensin-converting enzyme inhibitors (30). Only minor evidence from small randomized trials suggests that roxithromycin or doxycycline decreases the rate of aneurysm expansion. 30
There is also evidence that low-dose aspirin may reduce aneurysm expansion, especially in patients with medium-sized AAA (40-49 mm). 31
Smoking has been shown to play a role in development and in progression of AAAs.3,6 Brady et al reported a 20% to 30% reduction of aneurysm growth rate after smoking cessation. 3 Therefore, nicotine abstinence would be essential in AAA patients.
Treatment Options for Patients With AAA > 55 mm
Conventional open AAA repair is typically performed in general anesthesia. Access can be accomplished via a transabdominal or a left-lateral retroperitoneal approach. The procedure includes infrarenal cross-clamping and replacement of the aorta with a dacron or polytetrafluorethylene tube or bifurcated graft, depending on the anatomical configuration and extent of the disease.
Endovascular aneurysm repair is usually performed via a bilateral access to the common femoral arteries. The grafts consist of a main body, including 1 iliac limb and a contralateral limb that have to be inserted separately. The endovascular procedure can also be performed under spinal blockade or in local anesthesia.
The EVAR 1 trial compared open surgery with endovascular repair: 1082 patients older than 60 years with an AAA larger than 55 mm and no contraindications for surgery were randomized into a conventional open versus an endovascular repair group; 543 patients were allocated to the EVAR group and 539 to the open surgery group. The 30-day mortality was higher after open surgery compared to the EVAR group (4.6% vs 1.6%). However, after a 4-year follow-up, there was no difference concerning overall mortality between the 2 groups (26% EVAR vs 29% open repair). Also, in these 4 years of follow-up, considerably more complications were observed in the endovascular group (graft thrombosis, graft stenosis, renal infarction, etc) compared to the open surgery group (41% vs 9%). Accordingly, the reintervention rate was higher in the EVAR group than in the surgery group (20% vs 6%). 16
The EVAR 2 trial compared intervention and no intervention in patients unfit for open repair. Survival of these patients was not improved by intervention. 32
Costs and Efficiency
Analysis of total costs includes costs of 1-time screening and secondary costs for follow-up, surgery, and possible complications. A total sum of 16050 € was calculated in the Viborg study to prevent 1 AAA death. 33 After 5 years of follow-up, a sum of 9057 € was calculated for each obtained life year (2708 € after 10 years and 1825 € after 15 years). 33 The MASS study calculated a total sum of 7600 GBP after 10-year follow-up. 34 Direct comparison of these studies is difficult due to different study methodologies (Table 3). 35
Incremental Cost-effectiveness Ratios (ICER)
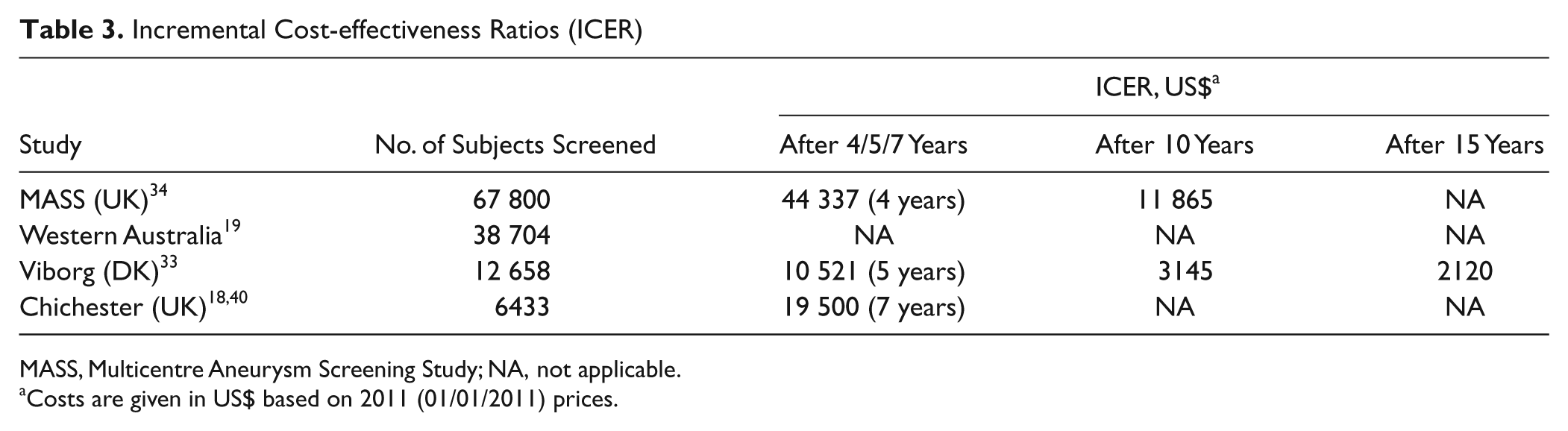
MASS, Multicentre Aneurysm Screening Study; NA, not applicable.
Costs are given in US$ based on 2011 (01/01/2011) prices.
The number needed to screen to prevent a single AAA-related death is used to evaluate the efficiency of AAA screening via ultrasonography. Screening of 350 persons is necessary to prevent 1 AAA-associated death during a follow-up of 7 to 15 years. This compares favorably to established screening programs like those for breast cancer (2451 persons over 5 years) or colorectal cancer (862 persons over 13 years).36,37
Screening Recommendations
Population to be screened
Men older than 65 years and men older than 60 years with history of smoking or with AAA family history. 8
Pro screening
Abdominal aortic aneurysm is an underdiagnosed disease with a high mortality after rupture. Most AAAs are asymptomatic unless they rupture, and patients rarely present with unspecific symptoms like lower back pain or diffuse abdominal pain. 6
Given its availability, noninvasiveness, and lack of radiation exposure, ultrasonography is the most valuable tool for AAA screening programs. A Web-based clinical decision support may result in improved delivery of AAA screening of eligible patients by primary care physicians. 38
Detection of a small aneurysm should result in periodic follow-up and optimization of medical treatment. For AAAs with maximal diameter of 55 mm at the least, rapid growth (0.5-1 cm/y), or eccentric constellation, guidelines (American Heart Association) recommend surgery or stent-graft intervention. 22 Abdominal aortic aneurysm screening in men reduces rate of ruptures and resulting mortality in up to 40%.
Contra screening
From the physicians’ perspective, it should be kept in mind that patients who have been confronted with AAA diagnosis, and potentially fatal subsequent effects, very often experience anxiety and decrease in quality of life. 2 Acceptance of screening decreases with age: 80% of 65-year-old people but only 66% of those older than 76 years accept screening. 18
When offering screening for AAA, vascular surgery centers also have to provide surgical capacities with short waiting lists. 2 The mortality rate should be less than 5% for open surgery and less than 2% for stent-graft intervention. 2
Footnotes
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors received no financial support for the research, authorship, and/or publication of this article.