
Abstract
Keywords
Introduction
Community health workers (CHWs) “offer promise as a community-based resource to increase access to health care.” 1 CHWs can serve as patient advocates, bridging cultural and social gaps between patients and health care providers by working with multidisciplinary teams to reduce health disparities.2-4 Their role is multifunctional; they have been identified as community health advisors, lay health advocates, promotoras, outreach educators, community health representatives, peer health promoters, and peer health educators. 5 Interventions integrating CHWs in the health service delivery team have been shown to improve adherence, blood pressure control and appointment keeping. 6-10
Health care providers’ and organizations’ attainment of cultural competency have been proposed as complementary strategies to improve the quality of care delivered to patients from diverse groups in an effort to reduce health care disparities.11-14 Interpersonal cultural competency has been defined as the “ability of individuals to establish effective interpersonal working relationships that supersede cultural differences.” 4 Organizational cultural competency allows a health care organization and its providers to understand the strengths and weaknesses and the unique needs of the population being served. 15 Characteristics ascribed to organizational cultural competency include having health care practitioners, leaders, and staff who are ethnically or socially similar to the community served; collecting and tracking data on quality of care, stratified by race; and engaging communities (eg, using advisory boards, hiring CHWs) in the design and delivery of health care facilities and services. Provider and organizational cultural competency may have synergistic effects on health care disparities and health outcomes.16,17
The extent to which cultural competency of heath care providers may influence the incorporation of CHWs into chronic disease care is unknown. We performed a cross-sectional study to examine the association of provider and staff self-reported cultural competency (cultural motivation, power and assimilation attitudes, and behaviors) and preparedness to deliver cross-cultural care with attitudes regarding the effectiveness of CHWs in reducing health care disparities.
Methods
Study Design
Project ReD CHiP (“Reducing Disparities and Controlling Hypertension in Primary Care”) and the ACT Study (“Achieving Blood Pressure Control Together”) are clinical trials of interventions to overcome barriers to hypertension control among patients receiving care at 6 community-based primary care practices in metropolitan Baltimore, Maryland, including 3 practices located in medically underserved areas of the city. 18 The proportion of patients with uncontrolled blood pressure (≥140/90 mm Hg) at each of these site ranged from 31% to 51% for African Americans and 24% to 44% for whites at the start of the trials. Prior to implementation of the study interventions (from April to December 2011), we invited 200 health care providers (physicians and nurse practitioners) and clinical staff (nurses, medical assistants, and others) from the participating practices to complete a questionnaire assessing attitudes toward several hypertension quality improvement strategies. In the survey, respondents also assessed their cultural competence in the following domains: motivation to learn about other cultures (cultural motivation), attitudes toward power and assimilation, frequency of culturally competent behavior and self-reported preparedness to deliver cross-cultural care. Because the ACT Study was designed to test a CHW intervention, the questionnaire also included items assessing perceptions of how a CHW intervention would affect health care quality and patient outcomes. Study protocols were approved by the Johns Hopkins Medicine Institutional Review Board.
Study Measures
Independent Variables
Provider and staff cultural competence and preparedness
We evaluated cultural motivation, power and assimilation attitudes, culturally competent behaviors, and cultural preparedness using self-reported summary measures from previous studies.16,19-22 Several of these measures have been associated with greater patient satisfaction and involvement in care.12,19 Similar self-report measures of cultural competence have been linked to quality and equity of HIV care. 13 Items for cultural preparedness were drawn from the Cultural Competence Assessment Instrument, which has been shown to reliably and validly 20 assess reported preparedness to deliver cross-cultural care.
We assessed provider and staff motivation to learn about other cultures by asking them to select their level of agreement with two items on a 5-point Likert-type scale (strongly disagree to strongly agree; Table 2). We assessed provider and staff attitudes regarding power and assimilation (awareness of racial inequities and privilege and acceptance of a cultural group’s choice to retain distinct customs and values by their level of agreement with items on a 5-point Likert-type scale (Table 2). Prior to analysis, negatively worded items were reverse coded so a higher score indicated a more favorable attitude. To measure culturally competent behaviors, we asked providers and staff to report the percent of time they performed the culturally competent behaviors (Table 2).
We assessed cultural preparedness using items measured on a 5-point Likert-type scale. All survey items are shown in Table 2. We examined mean scores on individual cultural competence and preparedness items as well as mean scores on the 4 summary measures.
Outcome Variables
Provider and staff perceived effectiveness of CHWs
To measure perceptions of the helpfulness of CHWs for reducing health disparities, we adapted a single question from an existing measure of health professionals’ motivation to improve quality of chronic illness care. 22 Agreement with this question was measured on a 5-point Likert-type scale. We categorized provider and staff responses as “higher” perceived usefulness (including those responding “strongly agree” and “agree”) versus “lower” perceived usefulness (all other responses). The survey item is shown in the footnote to Table 3.
Statistical Analysis
Provider and staff characteristics were summarized using descriptive statistics and the groups were compared using Fisher’s exact tests and 2-sample t tests. A higher score on most items indicated more positive cultural competence and preparedness attitudes. However, we reverse-coded items on the power and assimilation scale so that a higher score reflected awareness of racial inequities and acceptance of the choices of ethnic minorities to retain customs and values distinct from those of the racial majority. We calculated scale scores by taking the mean of the nonmissing responses for each participant. We used 2-sample t tests to compare provider and staff responses on the individual cultural competence and preparedness items and the scale scores. We performed multivariable logistic regression analysis adjusting for factors believed to be associated with the outcomes to evaluate the associations of aspects of cultural competency and preparedness with perception of CHWs. We also assessed potential moderation of independent variables (cultural competency and preparedness) by provider/staff status. The logistic regression analysis was repeated adding a term for the interaction of provider/status and the independent variable of interest. Analysis was performed using SAS version 9.3 (SAS Institute, Inc, Cary, NC). All tests were 2-sided and P < .05 was considered statistically significant.
Results
Study Population
We invited 200 providers and clinical staff and 119 (60%; 63% of nonresident providers, 32% of residents and 77% of clinical staff) participated in the survey. Overall, the majority of the participants were women (77%). Compared with providers, a higher proportion of staff were women (95% vs 57%). Provider participants included allopathic and osteopathic physicians and nurse practitioners. Clinical staff participants were registered nurses and medical assistants or licensed practical nurses. Additionally, the racial and ethnic distributions of provider and staff differed significantly, with a higher proportion of Asians among providers and a higher proportion of African Americans among staff (Table 1).
Characteristics of the Providers and Staff.

n = 54 for providers and n = 59 for staff.
n = 56 for providers and n = 59 for staff.
Provider and Staff Ratings of Cultural Competence and Cultural Preparedness
Provider and staff ratings of cultural competence and cultural preparedness are compared in Table 2. Provider and staff had similarly high ratings of willingness or motivation to learn about other cultures (4.4 vs 4.2). However, providers had significantly greater power and assimilation attitudes than clinical staff (3.5 vs 2.7). Culturally competent behaviors were reported with similar frequency among providers and staff (3.1 vs 3.1). Overall, staff rated themselves as more culturally prepared than providers did (3.8 vs 3.5). The largest difference between providers and staff in self-rated preparedness was about care for patients with low health literacy; staff felt more prepared than providers did (3.8 vs 3.1).
Mean (Standard Deviation) of Responses to Cultural Competency and Cultural Preparedness Questions by Provider/Staff Status.
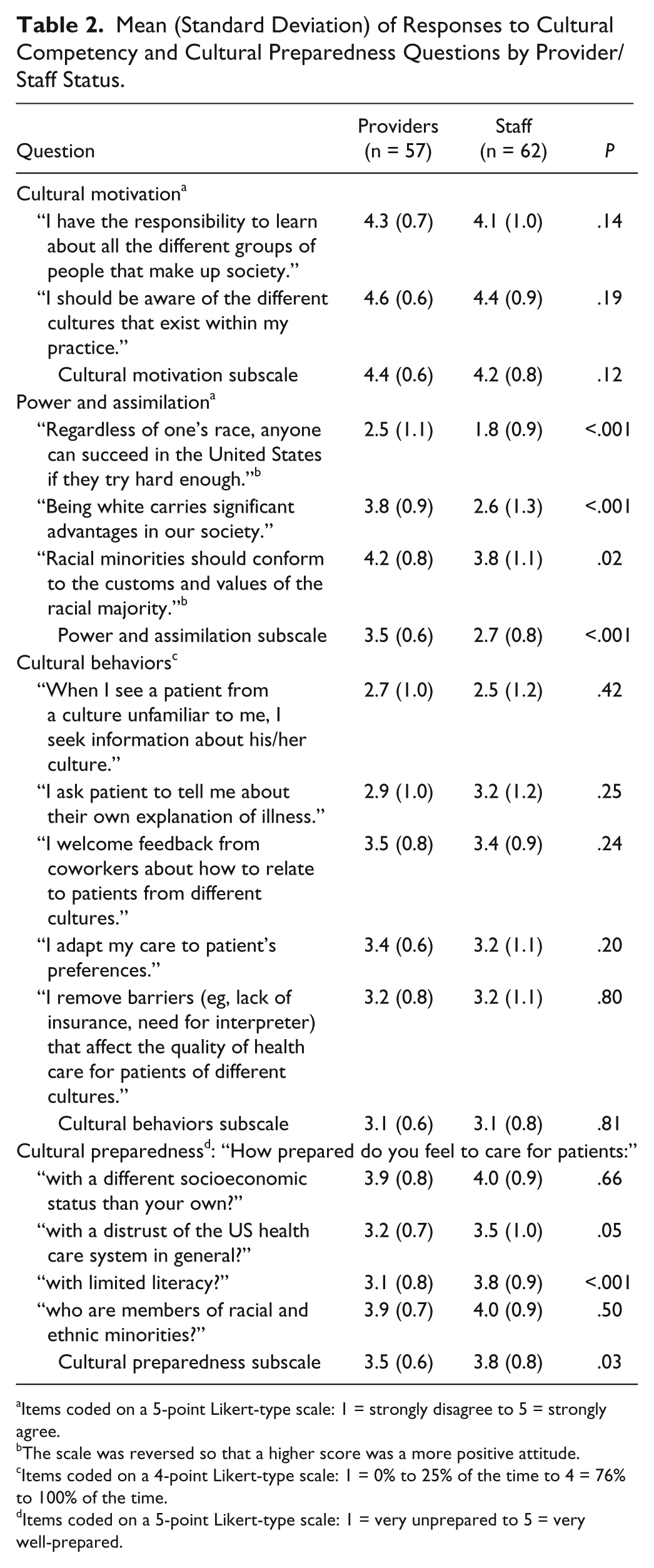
Items coded on a 5-point Likert-type scale: 1 = strongly disagree to 5 = strongly agree.
The scale was reversed so that a higher score was a more positive attitude.
Items coded on a 4-point Likert-type scale: 1 = 0% to 25% of the time to 4 = 76% to 100% of the time.
Items coded on a 5-point Likert-type scale: 1 = very unprepared to 5 = very well-prepared.
Provider and Staff Perceived Helpfulness of CHWs
Overall, 52 out of 110 respondents (47%), agreed or strongly agreed that CHWs would be helpful for reducing health care disparities. The responses differed by provider status; 58% of providers and 37% of the staff agreed with the statement. Nine persons (8%) did not respond to the perceived helpfulness of CHWs to reduce racial health care disparities question.
Associations of Cultural Competency and Preparedness With Perceived Helpfulness of CHWs
Table 3 shows the associations of cultural competency and preparedness with provider and staff perceptions of CHW helpfulness.
Association of Cultural Competency and Cultural Preparedness With Perception of Community Health Worker (CHW) Role in Improving Patient Outcomes and Reducing Disparities. a

Abbreviations: OR, odds ratio; 95% CI, 95% confidence interval.
Respondents were asked to state their level of agreement with the following statement: If there were a Community Health Worker (trained para-professional who provides, via phone and/or home visit, education and outreach to improve adherence to high blood pressure care and treatment) available to patients, this would: “help reduce racial disparities in care.” Models are adjusted for respondent’s age, sex, race (coded as black, white, other, unknown), years at practice, and provider/staff status.
Items coded on a 5-point Likert-type scale: 1 = strongly disagree to 5 = strongly agree.
Providers and clinical staff reporting higher cultural motivation had significantly higher odds (odds ratio [OR] = 9.66, 95% confidence interval [CI] = 3.48-28.80), as well as those reporting more frequent culturally competent behaviors had significantly higher odds (OR = 3.58, 95% CI = 1.61-7.92) and perceived CHWs as helpful for reducing health care disparities. Provider and staff power and assimilation attitudes were not significantly associated with their attitudes regarding CHWs’ utility for reducing health care disparities. However, provider and staff reporting higher cultural preparedness had significantly higher odds (OR = 2.33, 95% CI = 1.21-4.51) of believing CHWs’ would reduce health care disparities. For perceptions of CHWs’ utility in reducing health care disparities, the interactions of provider status with cultural motivation and power and assimilation were significant. In stratified models, greater cultural motivation was significantly associated with higher odds of perceiving CHWs as helpful for reducing racial disparities for both provider (OR = 3.17, 95% CI = 0.99-10.14) and staff (OR = 14.44, 95% CI = 2.78-75.2) subgroups. Greater power and assimilation attitudes were associated with lower odds of perceiving CHWs as helpful for reducing disparities among staff (OR = 0.40, 95% CI = 0.15-1.08),
Discussion
To our knowledge, this is the first study to examine the association between provider and staff self-reported cultural competence, cultural preparedness and perceptions regarding the usefulness of CHWs in reducing health disparities. Although 58% of providers perceived CHWs as helpful for reducing health care disparities, only 37% of staff felt the same. These findings merit further investigation since there must be buy-in from frontline staff as well as providers to successfully implement a CHW intervention.
Our findings could be explained, in part, by the possibility that providers and staff with greater cultural motivation, more frequent culturally competent behaviors and increased cultural preparedness, have increased cultural humility, recognize their own limitations in addressing barriers to care, and are willing to use outreach approaches, such as CHWs, that improve health care delivery for underserved populations. 23
Among staff, power and assimilation attitudes were actually negatively associated with perceived helpfulness for reducing disparities. Acknowledging racial inequities and the importance of minorities maintaining customs and values distinct from the dominant culture may not necessarily translate into perceiving that CHWs would help to address health disparities.
Our study has limitations. Because this was a cross-sectional study, we are not able to determine whether increased cultural competence and preparedness improves perceptions of CHW effectiveness or vice versa. Additionally, self-reported measures are subject to recall and social desirability bias. Self-reported cultural competence does not necessarily correlate to true cultural competence. Since only 60% of eligible providers and staff responded to the questionnaires, our findings may not be representative of all providers and staff at the sites. Another potential limitation is the lack of generalizability to those practicing outside of large metropolitan areas or serving less diverse patient populations. Of note, our study sites varied considerably in the ethnic and socioeconomic profile of the patients they served. There might also be unmeasured confounding. Though we accounted for years in practice at the current site, we did not account for the overall number of years of clinical experience, previous cultural competence training, and experience working with diverse patient populations or in underresourced settings. Additionally, we could not account for provider and clinical staff’s prior exposure to CHWs; however, to our knowledge, none of the sites were using CHWs at the time of the survey. Finally, the extent to which individual provider or staff attitudes and perceptions influence whether an organization ultimately employs a CHW is unknown.
Because CHWs are not health care providers, but agents from the community trained to interface with the health care community, CHWs are able to bridge cultural gaps between a diverse patient population and the health care system. Their incorporation into a health care delivery team can enhance both interpersonal and organizational cultural competency. Therefore, providers and clinical staff need to be more aware of the value added by CHWs to a delivery team. The Institute of Medicine calls for the “integration of cross-cultural education into health professions education to reduce health care disparities.” 4 A review identified the following changes to enhance sustainability of CHWs: integration into health care practice; organizational support for their role as part of the delivery team; and education of health care staff, administrators, and payers in order to improve understanding and acceptance of CHWs. 2
Primary care clinics employing CHWs could consider provider and staff education about the important roles CHWs play in order to improve services to diverse populations.21,24 Moreover, fostering cultural motivation and incentivizing cultural behaviors could enhance provider and staff willingness to incorporate CHWs in primary care delivery models. Health care policy actions should also provide frameworks that allow for the successful integration of CHWs interventions as part of the delivery team. These measures should include the following: provision of increased financing mechanisms for reimbursement of CHW services, allocation of resources for CHW training and clinic-community linkages, as suggested by the Affordable Care Act. Additionally, future research should identify the most effective ways to promote the use of CHWs within the social and organizational values and infrastructure of primary care clinics and communities.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is supported by grants from the National Heart, Lung, and Blood Institute (P50HL0105187 and K24HL083113).