
Abstract
Depression affects 5% to 9% of adults in primary care. 1 The US Preventive Services Task Force recommends routine screening for identification and treatment of depression 2 ; however, up to half of patients with significant symptoms go undetected. 3 Multiple factors, such as patient race/ethnicity and provider gender, affect detection of depression.4-8
American Indian/Alaska Native (AI/AN) people are more likely than the general US population to use the primary care provider (PCP) as their default source of behavioral health care,9,10 making screening for depression in primary care particularly relevant. Only 3 studies have considered the mental health status of AI/AN primary care patients,10-12 and of these, only 1 was specific to depression. 11
To more effectively respond to behavioral health needs of AI/ANs, Southcentral Foundation, a tribal health organization in Anchorage, Alaska, implemented a comprehensive depression screening initiative in 2001. 13 This screening, designed to occur once per year in the Alaska Native Medical Center Primary Care Center (ANMC-PCC) within a patient-centered medical home model of care, 14 uses the Patient Health Questionnaire as the screening instrument given its brevity and correspondence with Diagnostic and Statistical Manual–IV diagnostic criteria. 15 Although considered an administrative and programmatic success, not all AI/ANs are screened according to protocol. In this study, we examined patient and provider factors associated with depression screening coverage. Determining if certain patients are missed by certain types of providers will add to the general literature in which factors associated with the presence or absence of screening have not been sufficiently detailed.
Methods
Study Design and Setting
Cross-sectional clinical encounter data were extracted from the Resource and Patient Management System electronic records of AI/AN adults visiting the ANMC-PCC between March 2002 and August 2003. All services are prepaid with no limitations based on insurance status or copayment by the patient. The study period maximized number of eligible patients due for annual screening assuming 2 visits per year per patient. The project received tribal approval and approval from the Alaska Area Institutional Review Board.
Procedures
Each patient has a PCP who works with an integrated primary care team including a certified medical assistant or licensed practical nurse, a case manager who is a registered nurse, and a co-located behavioral health consultant shared across several teams. Each patient has a integrated primary care team at any single time, and all clinic visits involve multiple members of the team. If the patient is due for depression screening, an electronic reminder prompts the certified medical assistant or licensed practical nurse to administer and score the screening at the beginning of the primary care visit. The certified medical assistant or licensed practical nurse documents the depression score on a progress note prior to the patient being evaluated by the PCP 13 ; the depression score is entered electronically into the medical record.
Measures
Depression screening
The outcome was the presence or absence of 1 or more Patient Health Questionnaire–9 depression screening scores over the study period.
Patient factors
Demographic variables included age and gender. Clinical factors included previous antidepressant dispensation, depression diagnoses, substance abuse or dependence diagnoses, total number of chronic conditions determined by International Classification of Diseases–9 clinical modification code (hypertension, heart disease, diabetes, liver disease, renal disease, and pulmonary disease), and total number of visits in the year before the first visit of the study period. Antidepressants were identified according to the Healthcare Effectiveness Data and Information Set. Prior depression was indicated by an International Classification of Diseases–9 clinical modification code for major depression, dysthymia, or adjustment disorder with depressed mood.
Provider factors
Gender and length of employment with Southcentral Foundation, calculated as years between date of hire and the patient’s first visit in the study period, were PCP factors.
Statistical Analyses
Screening frequencies were calculated across patient and provider factors. A multilevel model approach similar to that of Hox 16 was performed to address nesting of patients within primary care teams. Models were fit separately for men and women due to significant gender interactions. First, an unconditional random-intercept model with no patient or provider factors was fit; we calculated the intraclass correlation from the provider variation estimated in this model. Next, patient factors were added, followed by provider factors. As provider tenure varied according to patient’s first visit date, this variable was entered with patient factors. The deviance test and Akaike and Bayesian information criterion values were used to compare models. Data analysis was performed with STATA statistical software package version 11.0, and P values less than .05 were deemed significant.
Results
All patients (N = 18 625) were AI/AN; 62% (n = 11 580) were women; ages ranged from 18 to 97 years. There were 51 PCPs, 18 (35%) of whom were men. Length of employment ranged from less than 1 to 16 years of service.
Table 1 presents the frequency of screening according to level of each patient and provider factor, stratified by gender. Forty-seven percent of AI/ANs were screened at least once during the study period. More women were screened than men (50% vs 43%, P < .001). Intraclass correlation was 0.09 for male patients and 0.08 for female patients, indicating 9% and 8% of variation in screening rates, respectively, were attributable to variation across PCPs.
Alaska Native and American Indian Male and Female Primary Care Patients Screened for Depression by Patient and Provider Factors

At patients’ first visit during study period of March 2002 to August 2003.
Chi-square significant (men vs women), P < .001.
Includes hypertension, heart disease, diabetes, liver disease, renal disease, and pulmonary disease.
Patient n = 665, 4% of all patients.
Table 2 shows random-intercept models evaluating odds of screening according to patient and PCP factors. For both genders, patients older than 35 years, with a physical condition, and with more primary care visits had higher odds of being screened. Among women, previous depression diagnosis was associated with higher odds of screening.
Random-Intercept Logistic Regression Models Evaluating Odds of Depression Screening Among Alaska Native and American Indian Male and Female Primary Care Patient by Patient and Provider Factors
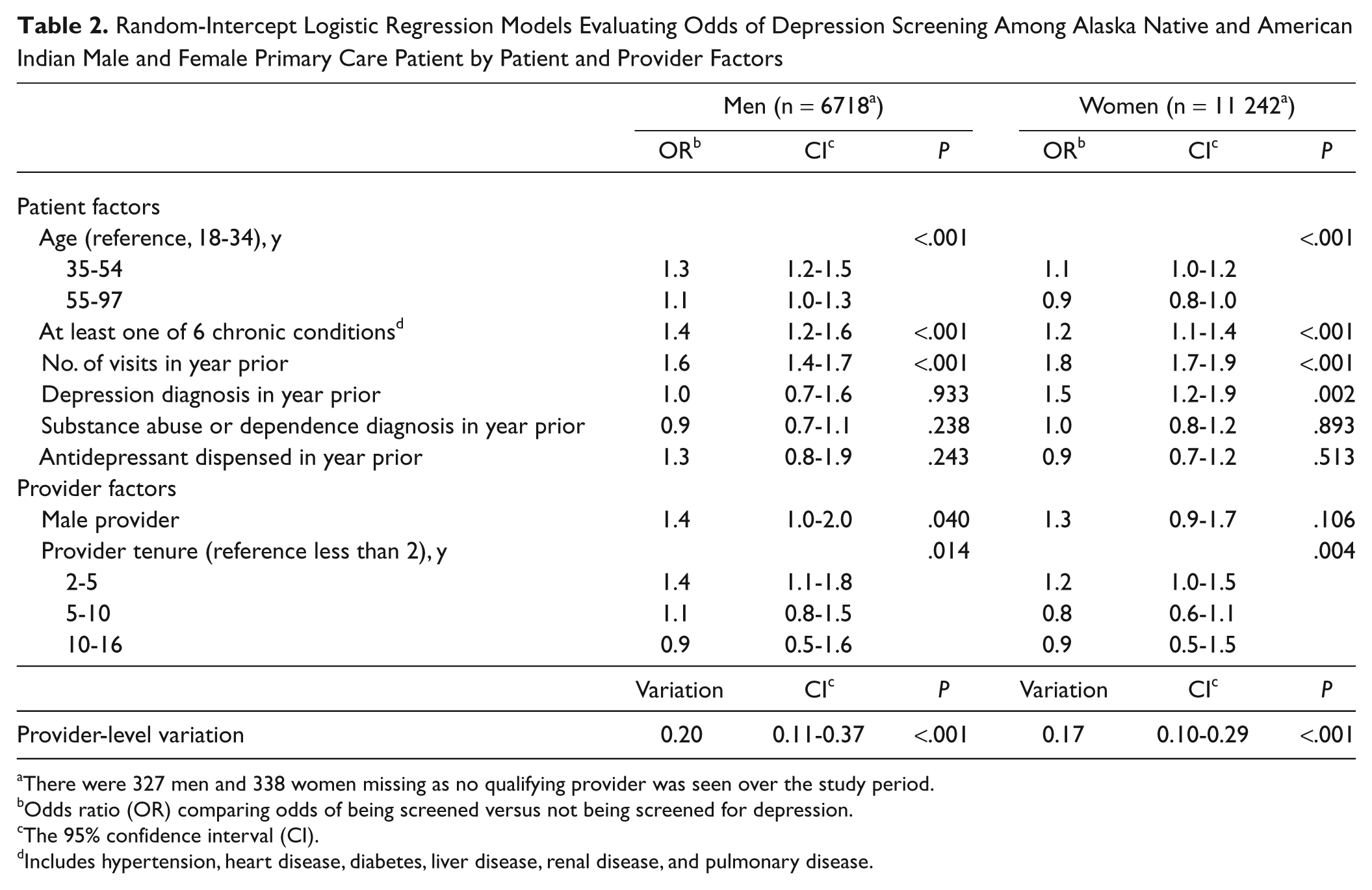
There were 327 men and 338 women missing as no qualifying provider was seen over the study period.
Odds ratio (OR) comparing odds of being screened versus not being screened for depression.
The 95% confidence interval (CI).
Includes hypertension, heart disease, diabetes, liver disease, renal disease, and pulmonary disease.
There was a moderate peak in screening rates for PCPs with 2 to 5 years of tenure. Male patients seen by male PCPs had higher odds of screening than did those seen by female PCPs. After adjustment for PCP characteristics, variation across PCPs remained significant.
Discussion
This study of AI/ANs is an important step toward understanding depression screening in a large AI/AN primary care setting. Almost half (47%) of the AI/AN patients seen over the study period were screened for depression, with higher screening rates observed among individuals with more annual visits and at least 1 chronic condition. Screening has the potential to increase opportunities for successful treatment, allow for more efficient resource use, and improve health outcomes.7,17,18
Characteristics of the patient affected odds of screening. Those with lowest odds were the youngest patients and men. Although the effect of age was modest for women, only 37% of young men aged 18 to 34 years were screened, compared to 48% of men aged 55 to 97 years. Depression may be more common among AI/AN women, 10 but mortality due to suicide, which is strongly associated with depression, is high among AI/AN males aged 15 to 24 years.19,20 Thus, the opportunity to address depression may have been missed for a critical group of patients, although men and the young may have differentially declined screening. Specifically, men appear to be less inclined to participate in depression-related research than are women. 21
In addition to variability in screening according to patient factors, PCPs varied systematically in their propensity to screen patients: up to 10% of the variation in screening coverage was due to the PCP. Other studies have shown that PCPs differ in training and comfort in addressing mental health concerns.22,23 Provider gender and tenure had a significant effect on likelihood of screening for some patients; that is, male patients were less likely to be screened by female PCPs than by male PCPs. Some studies have found that female PCPs self-report more difficulty in diagnosing depression in male patients than do their male PCP colleagues 24 ; however, other efforts have found no effect for gender match between PCPs and patients on the detection of depression. 8 In terms of tenure, there was a mild peak in the odds of screening for patients of PCPs with 2 to 5 years of tenure. Possible explanations for this finding are PCP familiarity with Southcentral Foundation, PCP knowledge of patient’s symptomatology, and timing of hire in relationship to the 1999 shift to a patient-centered medical home.
Integrated management and follow-up systems are recommended within any primary care system screening for depression in adults to facilitate both detection and follow-up. 25 The ANMC-PCC’s patient-centered medical home offers such support, including electronic reminders of overdue screening on day of visit as well as in monthly reports, an interdisciplinary team environment, and same-day access to follow-up care. Given that roughly half of the patients were not screened, our findings also indicate that additional supports are needed to successfully screen AI/AN patients who were missed in annual depression screening.
Our study had some limitations. The sample is restricted to ANMC-PCC primary care patients who received care from 2002 to 2003, and results may not generalize to other regions or practices. Data were queried from an electronic medical record of unknown reliability. Socioeconomic information, such as income, was not available, precluding assessment of whether screening varied according to other social determinates of health. Patient comfort in sharing mental distress or mood changes may also vary according to length of the patient-provider relationship. We also did not compare results to other routine screenings, so we cannot decipher if variations in screening were unique to depression.
Despite these limitations, understanding what factors affect depression screening could inform changes to screening protocols, facilitate enhanced PCP training, or spur greater efforts to reach patients missed within ANMC-PCC and other tribal health settings. Future efforts should compare depression to screenings for other health conditions and assess provider and patient attitudes toward depression screening, potential case load differences, and the impact of patient sociodemographic variables. Improving screening coverage could increase the recognition of AI/ANs with depression and improve health status with treatment. This first large-scale investigation of depression screening among AI/ANs suggest men and patients with infrequent primary care visits may require additional outreach. Efforts to improve depression screening in primary care settings may involve providing additional training or support to groups with lower screening rates among some segments of the AI/AN patient population. Lack of insurance and other access factors that were not relevant in this setting may influence screening rates in other primary care settings and warrant further study.
Footnotes
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this study was provided by the National Center on Minority Health and Health Disparities Grant P60 MD000507.