
Abstract
American Indian (AI) and Alaska Native (AN) community stakeholder engagement has the power to transform health research. However, the engagement and dissemination process is challenging in AIAN communities due to the historical and current negative experiences of AIAN populations in health research (Dillard et al., 2018). Whereas there is a paucity of recommendations about how to engage stakeholders in health research, from agenda-setting to proposal development, study design, recruitment, data collection, analysis, results, and dissemination (Concannon et al., 2014), there is limited information about how these recommendations are operationalized within the context of AIAN health research and practice (Concannon et al., 2014; Forsythe et al., 2016). For the purposes of this article, stakeholders are individuals, organizations, or communities who have a direct interest in the process and outcomes of a project, research, or policy effort (Boaz et al., 2018). Stakeholder engagement is a systematic process involving stakeholders, which provides opportunities for consultation, input, reviews, reactions, support, and assistance with dissemination. Dissemination focuses on how, when, by whom, and under what circumstances evidence spreads throughout agencies, organizations, states, counties, communities, tribes, researchers, policy makers, and service organizations.
Keywords
Health Research, Health Disparities, and Aians
The American Indian/Alaska Native (AIAN) communities have endured systemic racism in health research for more than 400 years. Systematic racism prevents AI populations from achieving health equity and complete health (Sexton et al., 2021). The AI populations experience worse mental and physical health outcomes than whites and are more likely to experience discrimination in health care settings. Cultural barriers, historical trauma, racist policies, present-day racial trauma, microaggressions, and everyday racism, traumatization, and retraumatization contribute to the glaring health disparities that AI populations experience (Skewes & Blume, 2019). Unethical and racist research conducted on Tribal communities continues to affect how research is implemented and disseminated (Shanley et al., 2015). Some examples of systematic racism and historical research violations include the involuntarily sterilization of AI women by the Indian Health Service, the improper use of genetic material with the Havasupai Tribe causing cultural and group harm (Drabiak, 2010), and failure to document informed consent from research participants (Willison, 2005). Mistrust between AIAN communities and researchers continues to be a significant barrier in the translation of health research findings into practice and accepted community knowledge (Pacheco et al., 2013). One distinguishing factor in all research contexts within AIAN communities is the acknowledgment of self-determination. The Indian Self-Determination and Education Assistance Act of 1975 (P.L. 93-638) allows tribes and tribal organizations to contract directly with the federal government for health services and programs (Hiratsuka et al., 2017). Results of this Act uphold the sovereignty status of Tribes, but can also make them vulnerable to researchers, state and federal agencies, and others wishing to conduct research in tribal communities. Collaborative models of research are emerging as a potential way to build trust and address systematic racism and health disparities in health research (Fisher & Ball, 2003).
Multiple collaborative research methods and approaches serve as a guide, some examples include community-based participatory research (CBPR; Wallerstein & Duran, 2006), Indigenous-based participatory research, participatory action research (PAR; Baum et al., 2006), and community–academic partnership research (CAP; Drahota et al., 2016). A common theme is a focus on engagement through partnerships, honoring local context, and involving community members as stakeholders in the research and dissemination process (Wali et al., 2021). Community and stakeholder–engaged approaches also advocate for time and resources to disseminate research findings back to participants and communities (Legaspi & Orr, 2007). Stakeholder involvement in health research improves quality, increases health knowledge through the translation of research findings, and increases the likelihood that research findings will be accepted and utilized by the community (Patil et al., n.d.). Wali and colleagues (2021) authored a systematic review of community-engaged research with Indigenous communities conducting chronic disease research. They documented the level of community engagement used in each phase of the research process and found that research approval and intervention efforts were the most common ways that researchers engaged communities and that research dissemination was the least common (Wali et al., 2021). Although stakeholder engagement in the dissemination of research findings to various audiences is viewed as essential (Fernández, n.d.), it is somewhat rare. A recent study of U.S. and Canadian researchers reported that academic journals and conferences were the most common dissemination approach, followed by reports to funding agencies. Face-to-face meetings with stakeholders were the least common, but the most impactful on policy and practice (Knoepke et al., 2019).
A significant barrier is that the translation of research findings rarely reaches the intended audience or those who could do something with the knowledge to improve public health practice and policy. Some estimates indicate that it takes up to 17 years for 14% of published evidence to be fully incorporated into clinical practice (Westfall et al., 2007). Knowledge translation is emerging as a solution to this problem, with attention to synthesis, dissemination, exchange, ethics, effective health services and products, and strengthening the health care system (Edwards, 2015). Stakeholder engagement in the dissemination of research findings may help address knowledge translation and dissemination barriers.
This article documents how the Center for Native American Health (CNAH) and the Native-Controlling Hypertension and Risks through Technology (Native-CHART) study engaged stakeholders in the research and dissemination process and fills a gap in the current literature by outlining a collaborative model for stakeholder engagement that can benefit universities and communities.
Aims of The Native-Chart Study and the Cnah
The Native-CHART study was implemented by Washington State University from 2017 to 2022 (https://ireach.wsu.edu/nchart/). Native-CHART’s overall goal was to improve control of blood pressure (BP) and associated cardiovascular disease (CVD) and stroke risk factors among AIAN and Native Hawaiian Pacific Islander (NHPI) populations. The long-term goal of Native-CHART is to generate findings that can be translated into practical policy, organizational change, and treatment innovations that will optimize patient-centered health outcomes and reduce or eliminate hypertension-related health disparities in underserved minority communities. Specific Native-CHART study aims were to (1) expand and establish new collaborations with research partners across private, tribal, and public constituencies that address BP control within a multilevel intervention framework; (2) develop a multilevel, multisector infrastructure and related processes that ensure inclusion of local, regional, and national views on research priorities and approaches to controlling BP; and (3) promote a scientifically rigorous, culturally informed program of inquiry that acquires new knowledge at multiple levels to implement innovative approaches to increase BP knowledge and awareness, activate and motivate patients, increase medication adherence, and improve BP control in AIs, ANs, NHPIs.
The study communities ranged from big cities in populous states to frontier villages in the farthest reaches of Alaska. Native-CHART research projects included interventions at the individual, family, community, and policy levels, with an emphasis on environments where BP can be controlled. Native-CHART’s Consortium and Dissemination Cores led outreach efforts of various Native-CHART Intervention Projects to health care providers and systems, governmental agencies, and AI organizations, patients, and communities by using culturally congruent methods and materials at appropriate literacy levels. Examples of Native-CHART pilot research projects that were disseminated by the CNAH include the meal-tracking app and education, home BP monitoring, walkability app for Trail of Tears, and the Dietary Approaches to Stop Hypertension (DASH) diet commodity boxes.
The CNAH at the University of New Mexico Health Sciences Center (UNM HSC; https://hsc.unm.edu/cnah/) served as one of the Native-CHART research satellite centers, which was part of the Consortium and Dissemination Cores for the southwest region. The CNAH led efforts to communicate Native-CHART results, using culturally appropriate methods and materials to health care providers, government agencies, and AIAN, NHPIs, organizations, patients, and communities. The CNAH’s vision is a healthy, productive world for Indigenous peoples. Its mission is to ensure AI student success and support tribal workforce development, and to advance AI health discovery and innovation. The CNAH works to be inclusive of cultural core values and leads engagement in the areas of community-defined health interests while promoting tribal and urban AI public health development. The CNAH is the UNM’s flagship program for AI health sciences students and leverages resources to address the health priority needs of New Mexico’s 23 federally recognized tribes and off-reservation AI communities.
Method
Circles of Involvement
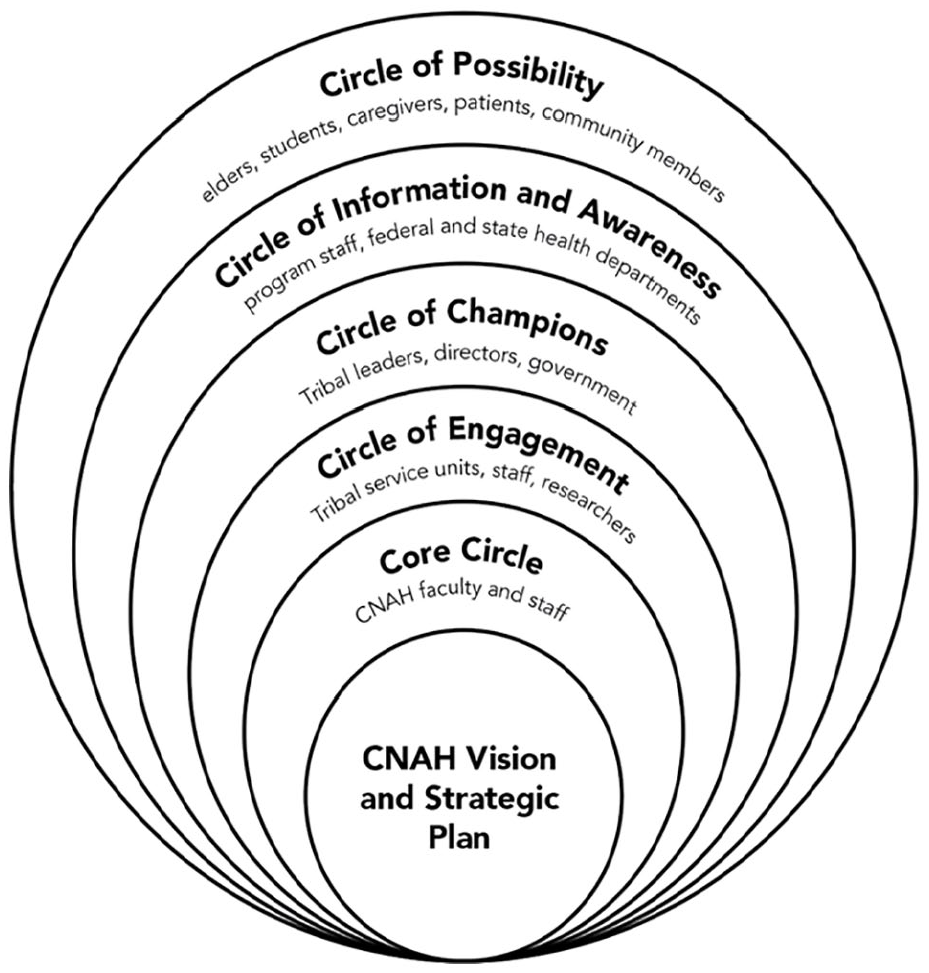
The CNAH utilized the Technology of Participation (ToP) secrets of implementation framework to guide stakeholder engagement and dissemination efforts (Institute of Cultural Affairs, n.d.). The ToP is grounded in the CNAH’s vision and strategic plan. A core circle of the CNAH faculty and staff serve as the foundation for all planning and outreach. Engagement then begins with Tribal staff and researchers. Each level of the circle is strengthened by the other and this is consistent with Tribal teachings and values where interdependence and strength come from collective participation.
Data Sources
The authors reviewed multiple data sources to enhance data credibility and comprehensively document the stakeholder engagement process (Baxter & Jack, 2008). Data sources included annual symposium agendas, publications, and resources disseminated during these events, presentations, notes from meetings, the CNAH’s strategic plan, and consultation with Tribal leaders and policy makers. Using an iterative process and critical reflection (Yin, 2003), the authors here explored the process in which the CNAH engaged with various stakeholders in the Southwest region using the ToP and Circles of Involvement framework. Authors reviewed data sources using aspects of qualitative methods to assess evidence of engagement based on the principles of consultation, collaboration, empowerment, information, and participation. The authors then documented the CNAH’s stakeholder engagement process and lessons learned from the data.
In July 2021, the authors explored how data sources and the ToP framework (Figure 1) could be used to organize the CNAH’s stakeholder engagement process. For example, the CNAH’s Core Circle did most of the day-to-day work to build authentic engagement opportunities. The CNAH’s Core Circle of faculty and staff members led outreach efforts, planning, symposia, communications, tracking dissemination efforts, and documenting perspectives about CVD and BP management. The Circle of Engagement included researchers and academic study team members who were mainly involved in sharing Native-CHART-related health research findings at annual conferences. The Circle of Champions included Tribal leaders, Tribal policy makers, and university leadership. The Circle of Information and Awareness included organizations that had previously partnered with the CNAH on health conferences, students enrolled at UNM, professors and researchers interested in AI health, and health clinic staff. The Circle of Possibility were people that the CNAH identified as potential partners and researchers in the field, but who were not yet involved in Native-CHART or the CNAH’s efforts.
CNAH Circles of Involvement Native-CHART Study
Results
The CNAH’s Core Circle developed key relationships with new and existing partners and individuals while utilizing multiple engagement methods to support the Native-CHART study and dissemination of study findings. Dissemination included sharing information during planning and engagement meetings and presenting Native-CHART results at the CNAH-hosted symposia. The CNAH also shared information widely from Native-CHART intervention pilot projects, including the BP-Improving Control Among AN People, the Chickasaw Healthy Eating Environments Research Study, and the Engaging NHPIs and Activating Communities to Take Steps (ENACTS) study.
During the first year, the CNAH’s Core Circle engaged in critical stakeholder conversations using in-person planning meetings, email communications, and individual communications. Some stakeholders felt that cultural topics were most important. Several felt that focusing on the strengths and being positive rather than negative was essential for the Native-CHART study. Other critical conversations focused on values, such as helping, communicating information in relatable ways, building local knowledge, sharing knowledge in relatable ways, and being inclusive of all age groups. Importantly, symposiums offered continuing education units for those needing education credits for their licensures. The CNAH provided a certificate of attendance for tribal staff, program directors, and leaders, which provided a sense of participation and contribution to the discussion(s) they attended. Several tribal individuals requested a certificate to validate their participation. The CNAH’s Core Circle utilized several engagement methods, including clinical provider partnerships, in-person meetings with the State Department of Health, and Native-CHART; Table 1.
Description of the CNAH Stakeholder Engagement Methods and Outcomes Native-CHART
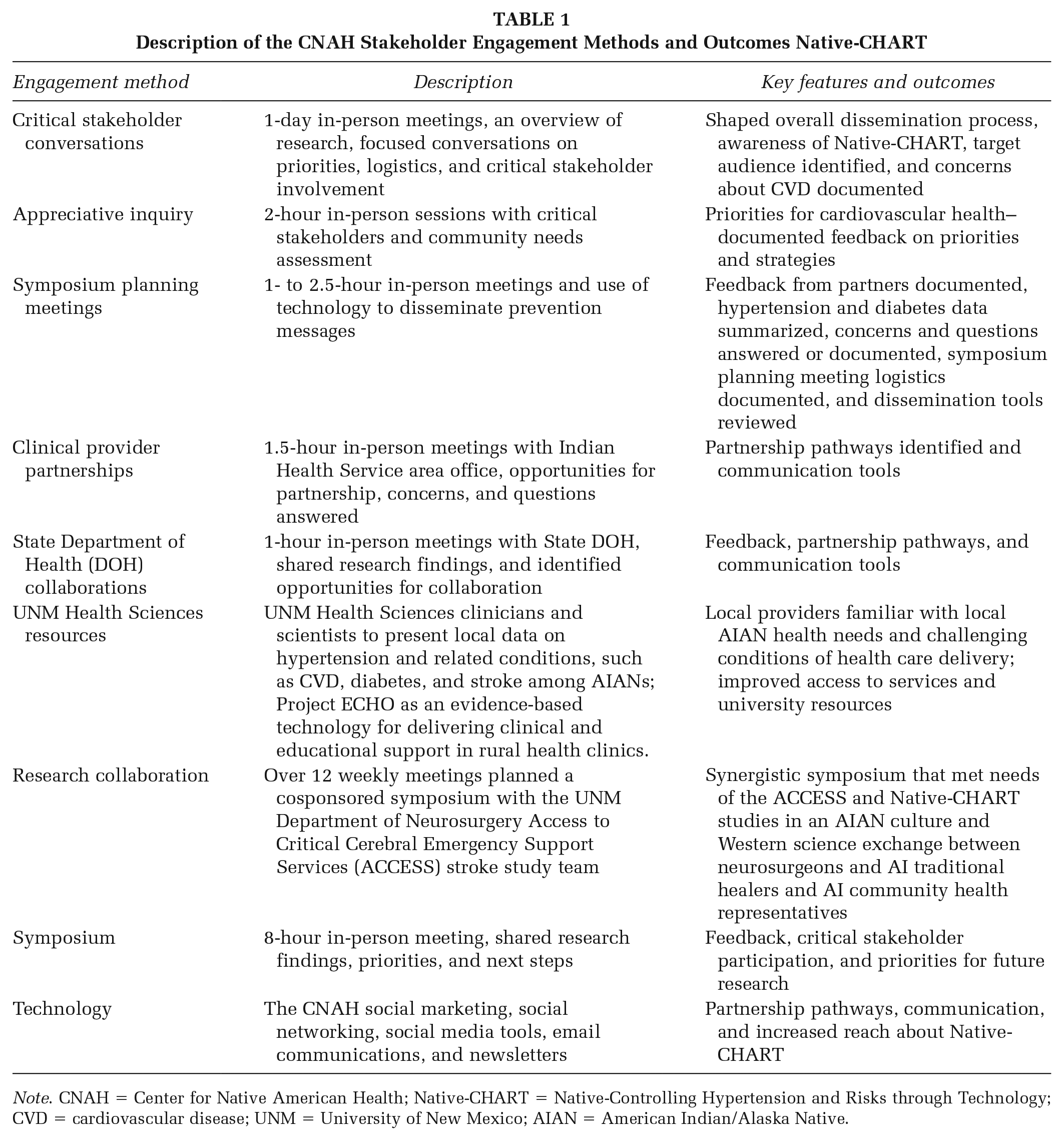
Note. CNAH = Center for Native American Health; Native-CHART = Native-Controlling Hypertension and Risks through Technology; CVD = cardiovascular disease; UNM = University of New Mexico; AIAN = American Indian/Alaska Native.
A specific time line of how the CNAH engaged stakeholders and the focus of engagement efforts is presented in Supplemental File Box 1.1
During the first Native-CHART community stakeholders’ introductory meeting in Albuquerque NM on April 7, 2017, the focus was on introducing the Native-CHART study and identifying stakeholder groups, using appreciative inquiry and having critical stakeholder conversations. Participants identified the following stakeholder groups as potential dissemination partners for Native-CHART: Medicaid, food banks, behavioral health, community health workers and health representatives, convenience store operators, health and fitness centers, mental health care professionals, prevention and awareness programs, UNM Project—Access to Critical Cerebral Emergency Support Services (ACCESS), eye professionals, senior centers, local nonprofits, dental health professionals, private sectors such as Walgreens, Indian Health Service, caregivers, tribal liaisons of New Mexico Department of Health, tribal leaders, state and federal legislators, clinics, private primary care centers, local youth groups, American Heart Association, and employers. The CNAH’s Core Circle worked to engage these groups in various Native-CHART research and dissemination activities throughout the study.
The stakeholder groups engaged in the Native-CHART health research dissemination process varied throughout the 5-year study. Notably, when Native-CHART was first funded in 2017, this was pre-COVID-19. In March 2020, when COVID-19 affected the world, and the CNAH/Native-CHART operations, this shifted everything at the CNAH and how the Core Circle worked to engage stakeholders and disseminate research findings. The CNAH’s use of technology (Project ECHO) supported health care providers and introduced telehealth technology to communities and clinics that had not used it before. Stakeholders involved in Native-CHART relied on virtual platforms instead of in-person meetings; this unexpected benefit helped stakeholders and communities become more familiar with technology and may promote the uptake of at-home health monitoring in the future. The CNAH’s Core Circle was responsible for organizing a diverse group of stakeholders who would assist the dissemination of Native-CHART pilot studies and educational materials. The CNAH reached out to education specialists who provide care to AI patients and others; education topics included the prevalence of hypertension and related conditions, local interventions, clinical care, prevention, and use of technology to support rural health care providers, and individual in-home monitoring. Table 2 shows that most persons involved in the CNAH’s Native-CHART dissemination effort were community members (n = 14) or researchers (n = 6).
Stakeholder Groups Represented at the CNAH Native-CHART Meetings and Symposia
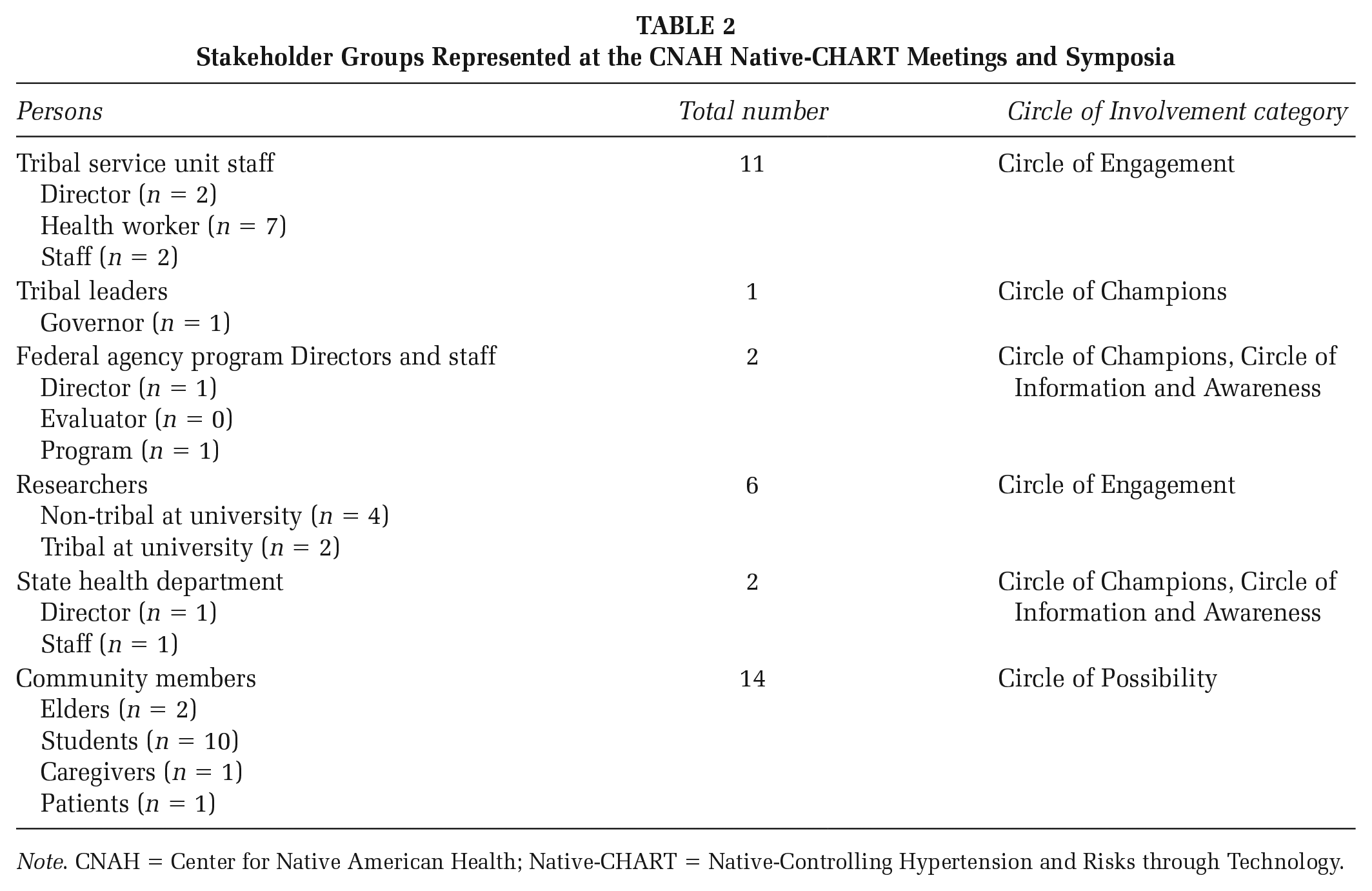
Note. CNAH = Center for Native American Health; Native-CHART = Native-Controlling Hypertension and Risks through Technology.
Cnah’s Stakeholder Engagement Process
Developing Key Relationships
The first step in the engagement planning process was to define key relationships for the Native-CHART study. As the CNAH’s role was mainly related to research engagement and collaboration, their focus was on building relationships that would assist them in engaging tribal communities, health care professionals, and tribal policy advocates throughout the southwest. Key relationships assessed in this review included the voluntary sector, informal sectors, policy partners, practitioners, beneficiaries, resource partners, and the public and private sectors. The CNAH’s vision and strategic plan guided this relationship-building process.
Exploring Possibilities and Doing the Work
The second step in the engagement process was conceiving possibilities and doing the work. This included the CNAH’s Core Circle of relationships where individuals would attend meetings, hold meetings, make decisions, coordinate communications, initiate program efforts, plan for new work, and bring on new partners or leaders.
Closing or Continuing
The third step in the engagement process was continuing the stakeholder engagement process or closing out the process. Presently, the Native-CHART study is in a 1-year, no-cost extension period. The CNAH’s Core Circle has shifted, with some staff members leaving the university or taking different jobs and positions. The implementation of Native-CHART research was stalled by the COVID-19 pandemic, and the CNAH quickly adapted engagement and dissemination methods to meet local requirements. For example, the CNAH Core Circle met weekly using Zoom rather than in person and used interactive web-based applications (i.e., Zoom whiteboard, Miro, and Jamboards) to communicate and share ideas with stakeholders. Dissemination of research information transitioned from printed posters and flyers to mostly online, using social media platforms, such as Facebook, Instagram, and Snapchat.
Implications For Practice and Research
The CNAH learned several lessons about stakeholder engagement from the Native-CHART study. First, stakeholder input early in the research process is essential. The CNAH engaged stakeholders early in the Native-CHART study and this helped with the dissemination and recognition of research findings. Second, the CNAH’s model for engaging various stakeholders at multiple levels (from the Core Circle to the Circle of Possibility) ensured that dissemination efforts would reach multiple audiences while cultivating the CNAH’s presence in the southwest as a resource for Native American health. However, not all stakeholders identified during the initial planning meeting in April 2017 were engaged over the 5-year study period. The reasons for this might be related to COVID-19, challenges with building new partnerships in communities, or it is possible that stakeholder involvement was not fully documented in the administrative documents reviewed. Third, research priorities and ideas are different at the community level and within each circle of engagement. It was difficult to address all stakeholder priorities and needs in a large-scale research effort like the Native-CHART Study. Fourth, AIAN stakeholder–engaged research and dissemination has the power to transform, connect, and validate health research findings. The benefits of engagement are far-reaching and include building social capital, community capacity, empowering communities, and supporting communities as they achieve their goals (Cyril et al., 2015).
Discussion
The CNAH’s approach presented here is subject to a few limitations. First, stakeholder engagement and dissemination varies by tribal affiliation, university conditions, existing relationships, and staffing. This approach may not work in all university-community settings. Second, the Native-CHART study was implemented during the COVID-19 pandemic; this influenced how outreach, communication, and relationships were established because the team relied more on technology than preferred in-person methods. Even with these limitations in mind, the CNAH’s approach to engaging stakeholders and disseminating research is a model that may benefit others, as they plan and conceptualize engagement in research.
The CNAH recognizes current critiques of the term “stakeholder.” Some feel that banishment of the term stakeholder is necessary because the term is related to the settler practice of “staking a claim” and this may be particularly offensive to Indigenous communities (Sharfstein, 2016). Use of this term in research and practice may convey an abuse of power, ownership, or control over something or someone (Kujala et al., 2022; Sharfstein, 2016). The CNAH recommends that future work and publications consider replacing the term stakeholder with partners, collaborators, interested/affected groups, relatives, or relevant parties.
The CNAH expanded and strengthened stakeholder engagement throughout the 5-year project. Ultimately, the CNAH’s efforts supported Native-CHART study aims to expand and establish new collaborations, develop multilevel and multisector infrastructure related to BP control, and promote scientifically rigorous, culturally informed program approaches that increase knowledge, awareness, and health outcomes in AIANs. Considerations for the dissemination of health research findings and health resources with AIAN populations must be communicated at the beginning of any research endeavor. Stakeholders have unique knowledge about what dissemination should look like. Almost 70% of AIANs get information about CVD on the internet (Boyd et al., 2020), but internet connectivity and access are still the number one issue in rural and remote tribal and non-tribal communities. In addition, even if connectivity and access are available, not every household has access to a working computer to browse the internet for additional information. Finally, available health information is not always culturally relevant or appropriate for tribal community members.
Dissemination of health research information and materials must include cultural and traditional ways of disseminating information, such as visual, auditory, storytelling, language, symbols, and imagery. Looking toward the future, it will be essential for researchers, academics, health educators, and policy makers to engage AIAN stakeholders in the development of health information and disseminate information using multiple methods, including the internet and other platforms that are readily available to AIAN people. Engagement and information dissemination can empower, uplift, build equity, and give voice to communities that have been historically marginalized and oppressed by researchers. The CNAH’s model for stakeholder engagement may be helpful to other universities and communities as they make decisions about who to engage and the circles of possibilities that exist.
Supplemental Material
sj-docx-1-hpp-10.1177_15248399231160563 – Supplemental material for A Model of Stakeholder Engagement with American Indians and Alaska Natives from the Native-CHART Study
Supplemental material, sj-docx-1-hpp-10.1177_15248399231160563 for A Model of Stakeholder Engagement with American Indians and Alaska Natives from the Native-CHART Study by Tassy Parker, Norman James Cooeyate, Nathania Tsosie and Allyson Kelley in Health Promotion Practice
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.