
Abstract
In our otorhinolaryngology walk-in clinic, we estimate more than 70% of the patients present with sore throat. A large proportion would have been to their general practitioners or outpatient departments and were prescribed with at least a gargle to soothe the discomfort.
Commercially, gargles and sprays are made easily available, and even the basic salt water gargles, made by mixing 1 teaspoon of salt in 1 cup of warm water, is commonly used to improve symptoms. 1 However, many patients resort to seeking a second opinion at our clinic as they find their symptoms not improving. On further questioning, we find that some patients rinse their mouths instead of gargling with the prescribed solution because they either were not aware of the proper technique or found it uncomfortable to gargle.
We were then interested in assessing the efficacy of oral rinse, gargle, and spray, as well as the effect of the Friedman palate position. This classification was introduced by Friedman et al to assess sleep-disordered breathing. 2 By using this classification, our pilot study was able to study the effect of gargles and sprays on a narrow oral airway and whether anatomy is an important factor in deciding on the treatment modality for a patient.
Method
Ten subjects participated in the study. Each had his or her oral cavity and oropharynx visualized with the 70° 4-mm rigid Hopkins rod, and the Friedman palate position was documented. The subjects were requested to rinse their mouths with 1mL of food coloring (Star Brand, true blue color) diluted to 14 mL of water for 30 seconds. The oropharynx was then inspected, and photographic records were taken of the oral cavity up to the base of the tongue using the same 70° rigid scope to assess dye distribution. The dye in the oropharynx was then rinsed off thoroughly.
Two hours later, the oropharynx was inspected to ensure there were no traces of residual dye. Another 15 mL of the solution was then gargled by the subject for 30 seconds. A second set of photographs was taken from the oral cavity to the base of the tongue.
After another 2 hours, once satisfied that there was no residual dye, they were asked to spray 4 squirts of the similar dye from a commercially made available oral spray bottle. Photographic records were taken.
The photographs were later analyzed to assess the distribution of the dye. Areas of interest were the soft palate, uvula, anterior tonsillar pillar, tonsils, posterior tonsillar pillar, posterior pharyngeal wall, and base of tongue. One score was given to each area if there was dye seen, which gave a maximum score of 7 for each modality (Table 1).
Scores for the Distribution Rinse, Gargle, and Spray With the Respective Friedman Palatal Position

Results
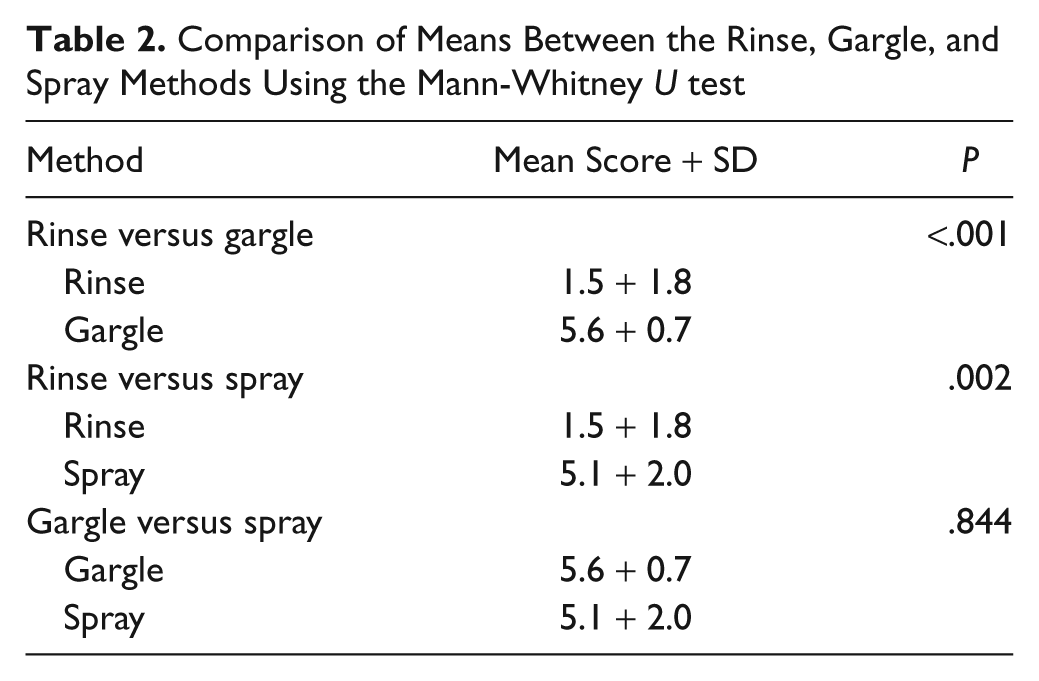
The Friedman palate position and the scores of the different modalities are shown in Table 1 with the mean scores and SD tabulated. Comparison of the means using the Mann-Whitney U test showed both gargles (P < .001) and sprays (P = .002) were significantly better than were the rinses. However, there was no difference in efficacy between the sprays and gargles (Table 2).
Comparison of Means Between the Rinse, Gargle, and Spray Methods Using the Mann-Whitney U test
We also found that anatomy did not play an important role in terms of the efficacy of the different methods. There was no significant difference in the mean scores between Friedman 1 and 2 compared to Friedman 3 and 4 (Table 3).
The Effect of Friedman Palatal Position on the Mean Scores of the Different Modalities Using the Mann-Whitney U Test

Discussion
Any painful sensation arising from the pharynx and its surrounding area is described as sore throat. Causes are varied and may be due to infection such as a cold or flu, pharyngitis or tonsillitis, allergic reactions, irritation, dryness, or trauma. 3 Treatment of something as simple as sore throat is usually symptomatic and plays a crucial role in patient satisfaction and reducing health care costs. In the Western world, about 6.7 million visits are made annually by adults to a medical practitioner for sore throat. In the United Kingdom, the National Health Service estimated that about £60 million per annum is spent on consultation for sore throat alone, and this is excluding investigation or treatment. 4
In Malaysia, it was reported that 44.1% of all pediatric admissions were due to acute respiratory infections, and in another separate study, around 91% of the acute respiratory infections were due to upper respiratory tract infections. 4 What is alarming is that the antibiotic prescription rates for upper respiratory tract infections are 46.7% and 27.8% in private and public primary care clinics, respectively, whereas the bacterial etiology in upper respiratory tract infections cases only ranged from 2.4% to 14%. 5
As most of the uncomplicated sore throats will resolve without treatment, what the patients really need is symptomatic relief. Paracetamol or ibuprofen is found to provide adequate pain management. Anesthetic gargles, salt water gargle, lozenges, eating soft foods and frozen desserts, and drinking cool or warm liquids have also been recommended.6,7
Our interest was in topical therapy, specifically oral rinses, gargles, and sprays. This emphasis is placed on topical therapies because it acts by direct application to a targeted area and reduces risk of toxicity compared to systemic administration. Oral rinses and gargles may also be used for oral hygiene with disinfectant and anesthetic ingredients commonly used, such as benzydamine, cetylpyridinium chloride, and benzocaine, although throat sprays may contain local anesthetics such as benzocaine and disinfectants such as chlorhexidine gluconate and phenol. 3
This study focused on the distribution of the topical preparation. The blue food dye allowed us to assess which modality had better distribution. We demonstrated that rinsing was clearly inferior when compared to gargling and spraying if the intent is to have the medication coat the oropharynx. This finding is noteworthy as in most cases of sore throats, prescribed topical medication should reach the oropharynx effectively as it is where the inflammation is usually located.4,8,9
Similarly, Patel et al concluded that oral rinses should be used to treat diseases of the oral cavity, whereas the oral sprays and gargles gave better results for ailments of the oropharynx. 10 However, the authors also found that sprays were more effective when compared to gargling. Our results instead showed the sprays comparable to the gargles. This then provides more options for the patients as they can now choose either method, whichever is more comfortable or economical as they are equally effective. What we have witnessed in our clinics is that some patients do not understand the technique of gargling and may rinse instead, thus giving rise to poor improvement of symptoms. Time should be taken by the prescribing doctor to educate the patient to avoid confusion. If gargling cannot be achieved, we then recommend oral sprays.
In our study, we were fortunate enough to have an equal distribution of patients with an adequate oral airway (Friedman palate position 1 and 2) compared to a narrow oral airway (Friedman palate position 3 and 4). Using the Mann-Whitney U test, we compared the mean distribution scores of each modality of those with adequate oral airway versus those with narrow oral airway. Surprisingly, we found that there was no significant difference between the efficacy among the 2 groups, which means a narrow oral airway did not deter the distribution of dye as one would expect. However, ours is a pilot study with a small sample size. In the future, we may carry out a larger-sized sample to study its significance.
In conclusion, we find the oral gargles and sprays significantly better than oral rinses if the oropharynx is the targeted site. The size of the oral airway does not impede their efficacy if the patients know how to gargle and spray adequately.
Footnotes
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) received no financial support for the research, authorship, and/or publication of this article.