
Abstract
Across the country, there is an outcry for new solutions that can reduce health care costs.1,2 Woven within the debate of viable solutions are complex issues including cost, access, quality, clinician-patient communication, and patient health literacy.3,4 Technology has also added another complex layer to the health care environment, including the availability of online health information. 5 Recent increased use of Web-derived health information has created another communication channel for providing health information, expanding clinician-patient communication, and potentially increasing patient health literacy rates.6-8 However, the availability of such information has not assured better health outcomes9,10 or increased patient health literacy.5,11
The physician- or clinician-patient relationship and quality of communication have been identified as a crucial component of health literacy.4,12-14 Methods to improve communication and facilitate a trusting relationship have been described such as improved space and interface tools 15 and simpler health information materials. 14 However, the need remains for a universal online tool to provide health information about multiple diseases/conditions to patients. 16
Through demonstration, information therapy (Ix) has been defined as “any set of treatment guidelines as long as it is evidence-based, independently derived, peer-reviewed, nationally recognized, and relevant” that is prescribed by a physician and consumed by a patient.17,20 It has also been defined as “the therapeutic provision of information to people for the amelioration of physical and mental health and well-being” and includes helping patients through access to information and patient education.18,19 Recently, experts have included Ix 19 as a method for increasing clinician-patient communication, patient adherence, patient understanding of diagnosis and treatment options, and reduction in hospitalizations.6,19,20
MedEncentive
The Web-based Ix program (hereafter “the program”) has several years’ experience in development and successful testing of providing Ix to both physicians and patients.19,21 Unlike other health information sources, this product has included using financial rewards for providers and patients to encourage “mutual accountability” (ie, both parties are financially compensated, are acting on the evidence-based Ix provided, and agree to confirm each other’s adherence) (Figure 1). The program has made an important contribution toward transforming health and health care as evidenced through previous pilot studies.19,20,22 The first installation of the program was in 2004 and has been previously described in the literature. 19
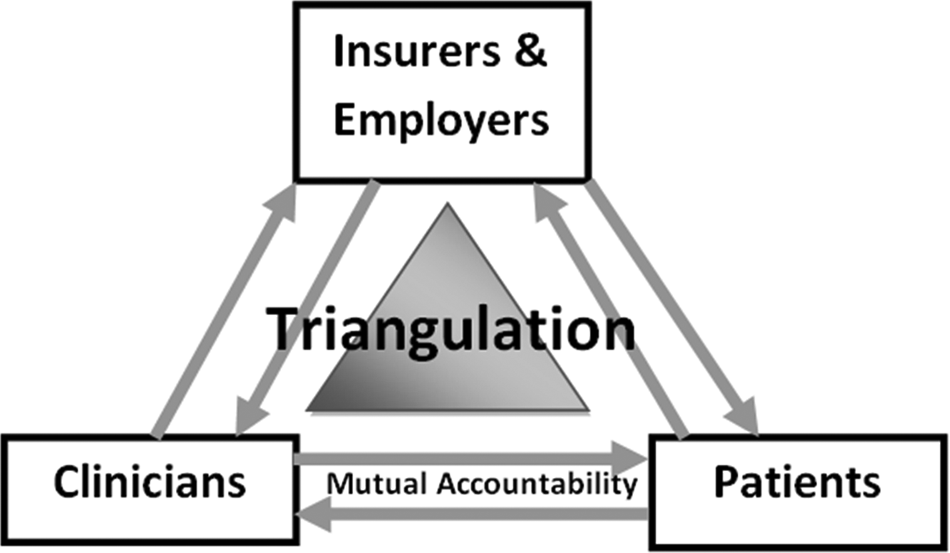
Conceptual model of “mutual accountability”.
Information therapy can be prescribed to patients/members through the program in 3 ways: (1) by the physician on a real-time basis while the patient is in the office or shortly thereafter, referred to as point of service; (2) by the physician after the fact as the result of a claim for the office visit being submitted by the physician, referred to as claims initiated; and (3) by the program computer system based on the diagnosis listed by the physician on the office visit claim, referred to as system generated.
Physicians are most commonly introduced to the program through patients at the time of service. The program is designed to be adaptable to any set of treatment guidelines as long as it is evidence based, independently derived, peer reviewed, nationally recognized, and relevant. Once the Ix has been prescribed, either by the physician through the online system or automatically, patients are directed to the program’s online Website to review their Ix independently. The Ix is in the form of online articles, primarily text. Physicians receive notification through the system when Ix prescriptions have been read.
Improving clinician-patient communication through the use of financial incentives and evidence-based information programs may result in increased health literacy rates for patients, increased patient adherence, increased motivation to improve health literacy and health behaviors, and improved physician-patient communication. We examined this hypothesis by utilizing the program’s unique financially incentivized program and data from participating patients.
Methods
This study independently examined participating patient perceptions of the program from two employers with pilot demonstrations. A secondary, retrospective cohort analysis was conducted of survey questions administered to patients after they received each Ix and before receiving a financial reward.
Participants
Employer 1 involved employees and dependents of a municipality in a Midwestern community with an approximate population of 25,000 people and began the program in 2004. Employer 2 involved employees and dependents in a Midwestern community with an approximate population of 350,000 people. The employees and dependents of Employer 2 were from an outpatient, multispecialty group practice owned and operated by physicians and began the program in June 2007.
Survey
The survey measured participating patient perceptions of the program. Data from the survey were administered through an online platform (ie, Website) for Employer 1 (N = 4105) from January 1, 2006 through December 31, 2009 and Employer 2 (N = 8123) from June 1, 2007 through December 31, 2009. The survey initially included 13 questions. In August 2008, 2 questions were added to the survey, and 5 more questions were added in November 2009. The questions were offered as forced-choice, 5-point Likert scales, and 3 open-ended qualitative questions were included in the survey.
Incentives
Due to the nature of secondary data analysis, no participant incentives were provided for this study. However, physicians were paid for prescribing Ix prescriptions to participating patients; the amount of the incentive was determined by the timing of the Ix prescription. Physicians most commonly earned $15 for their activity if completed before the insurance claim was filed. If the physician needed to be reminded by a system-generated fax or email to practice from the system, the reward was half that amount. Patients were also financially rewarded for participating. Employers/insurers choose to offer rewards as a rebate/refund of an office copayment, a reduction in insurance costs, or a credit to a health savings account (this was predetermined through the contracting employer/insurer and the program). Employer 1’s financial incentive increased by $5 during the 5 years the program was implemented from $25 to $30. Employer 2’s financial incentive remained constant over 2 years at $15. A fuller description of the program has been described previously. 20
Results
Participation in the program was 66.9% for Employer 1 and 68.1% for Employer 2. The average monthly health plan members were 527 and 1275 for Employer 1 and 2, respectively. Participation was defined as the number of Ix prescriptions completed by health plan members divided by the total number of Ix opportunities.
Demographics
Employer 1 participants were 50.1% male and 49.9% female. Employer 2 participants were 66.9% female and 33.1% male. The average age of participants from both employer groups was 37 years (standard deviation [SD], ~20 years).
Ix Type
The method in which the Ix was prescribed was automatically coded by the online system as 1 of 3 options: point of service, claims initiated, or system generated. The majority (81.9%) of participants from Employer 1 received claims initiated Ix, followed by point of service (18.1%). The same was true for Employer 2; 70.7% of the Ix was claims initiated, and 29.3% was point of service. Seventy-three percent (72.8%) of Employer 1 participants and 65.7% of Employer 2 participants indicated their physician directed them to the program Website and discussed why they should view the information.
Impact
Participants were asked to rate several aspects of their experience including helpfulness of program information, their adherence to recommended treatment(s), physician’s performance, motivation to improve health literacy and health behaviors, the impact of the economy on health care service decisions, and importance of physician’s awareness of patient self-management and health objective accomplishments. Participants rated each item on a 5-point Likert-type scale, with 5 being the highest and 1 the lowest.
Participants from Employer 1 found the information more helpful, t(8) = 4.19, P < .001, and rated their physician’s performance higher, t(9) = 4.85, P < .001, than those from Employer 2 (Table 1). Employer 2 participants reported higher adherence to recommended treatment(s), t(−12) = 4.83, P < .001, and greater importance of physician’s awareness of patient self-managing health, t(−3) = 4.58, P < .003, and accomplishing health objectives, t(−3) = 4.62, P < .003 (Table 1). Overall, the majority of participants reported that their health was improving (66.9%).
Average Participant Ratings

Discussion
The majority of the Ix prescribed to participants were claims initiated, meaning once the claim was submitted by the physician to the insurance provider, an Ix was automatically prescribed to the patient based on what condition or disease was billed. This presents a large opportunity for physicians to become increasingly involved in Ix programs. Initial findings from the survey suggest that the participants were satisfied with the information prescribed and that it was helpful in self-managing their disease; however, data on rate of participation by physicians were unavailable. The level of physician participation might be limiting the quality of communication between the physician and patient. Patients indicated the importance of the physician-patient relationship and that the relationship needs to be built upon trust. 14 Increasing physician involvement in the Ix process is one method that could be used to build trust between the physician and patient as well as promote effective oral communication between the two parties, which has been identified as an important component of health literacy. 4
Initial findings suggest that physicians were supportive of the program, as approximately 70% of participants indicated that their physician directed them to the Website and discussed why they should view the information. Despite this reported support, most Ix prescriptions originated from the system, which may indicate that the actual process of prescribing Ix may be too burdensome for the participating physicians or the monetary incentive may be too small. Future research is needed to understand why physicians recommend Ix but historically have not prescribed it.
There were no biomedical measurements (eg, blood pressure, weight, etc) available to determine how (or if) health behaviors changed as a result of the program or how their health status was improving, despite patient reports of improved knowledge and health behaviors. More specific questions should be added to the online participant survey to understand what behaviors are being modified. Other measurements will also be needed to determine how patients’ health statuses are improving, such as biomedical measurements, number of encounters (eg, primary care or emergency), and pharmaceutical records.
Participants also reported the knowledge that their physician had access to their questionnaire responses motivated them to improve their health literacy. However, no health literacy tool was used to determine how (or if) their health literacy improved. Previous studies have examined the effectiveness of an online Short Test of Functional Health Literacy in Adults (S-TOFHLA) compared to the traditional paper version with favorable results. 23 Future implementations of the program should include a health literacy assessment; it is recommended that an online S-TOFHLA or comparable assessment be added to the current online participant survey to better understand the impact on participants’ health literacy.
The findings are limited by the nature of the secondary analysis. The program described in this study was implemented as a solution for the health care environment: to improve physician-patient communication, improve patient health literacy, and reduce medical costs for employers. It was not initially intended to be a research study. The limitations of the study prevent generalization of findings to a larger population; however, these data have important clinical implications and can help inform future research.
Authors’ Note- These data used in this investigation were supplied by MedEncentive, Inc. to University of Kansas School of Medicine-Wichita under a Confidentiality Agreement, to conduct an independent evaluation according to a specific proposal to analyze the data. Under this nonmonetary exchange and Business Affiliation Agreement, the KUSM-W IRB approved (dated 9/21/09) examination of identifiable records. MedEncentive, Inc. has been given an opportunity to review, comment, make suggestions, and receive from KUSM-W responses to its comments and recommendations. The interpretations and conclusions represent those of the authors.
Conclusions
As the availability of Web-based health information increases, the importance of understanding the impact of this information increases. The relationship between a physician and patient has been evolving since its inception, and technology seems to be influencing the ways this communication occurs. This secondary analysis indicated a positive relationship between prescribed Ix and self-reported health literacy. Future research is needed to scientifically evaluate the effects Ix has on health literacy and health behaviors as well as the long-term impact on physician-patient communication.
Footnotes
These data used in this investigation were supplied by MedEncentive, Inc. to University of Kansas School of Medicine-Wichita under a Confidentiality Agreement, to conduct an independent evaluation according to a specific proposal to analyze the data. Under this nonmonetary exchange and Business Affiliation Agreement, the KUSM-W IRB approved (dated 9/21/09) examination of identifiable records. MedEncentive, Inc. has been given an opportunity to review, comment, make suggestions, and receive from KUSM-W responses to its comments and recommendations. The interpretations and conclusions represent those of the authors.
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
This research was supported in part through the University of Kansas School of Medicine - Wichita through a level II grant from the Kansas Bioscience Authority (QW850004).