
Abstract
Purpose
Patients are increasingly involved in decision making by their clinicians. Yet, there are concerns that involvement in decision making may cause emotional distress in patients. Little research has examined the nature of the burden experienced by patients confronted with a life-changing treatment decision. Therefore, we explored the nature and manifestations of burden experienced by patients with early-stage breast and prostate cancer regarding their involvement in decision making. We further aimed to identify patient-perceived causes and potential solutions for their experienced burden.
Methods
We used semi-structured interviews to explore the perspectives of patients with early-stage breast and prostate cancer. Patients (N = 24) were eligible if they were diagnosed in the past 6 mo and reported some degree of burden regarding their involvement in decision making. Two researchers independently inductively coded the interviews using thematic analysis.
Results
Patients described being burdened by the decision in various ways and at various moments in the decision-making process. Patients attributed their decision-related burden mainly to uncertainty, fear of making the wrong decision, insufficient guidance by their clinician, and feeling an overwhelming sense of responsibility for their treatment decision. Patients indicated various factors that mitigated their burden or facilitated decision making, including having sufficient time, the opportunity to discuss the choice with experts and/or family, and receiving advice or confirmation from family or the clinician.
Conclusion
These findings suggest that decision-related burden could be caused by the uncertainty and anxiety patients experience and by a nonpreferred division of roles within the decision-making process.
Implications
Accordingly, acknowledging patients’ feelings by discussing the presence of uncertainty and distress might normalize the burden for patients. Moreover, clinicians could explore and adjust to patients’ role preference in decision making and discuss what would facilitate the decision process for patients.
Highlights
Patients experience emotional, cognitive, and physical burden from their involvement in decision making.
Some of the burden appears to result from the way clinicians involve patients in decision making.
In addition to information about options, benefits, and harms, patients require active support in their decision-making process.
Clinicians could aim to avoid overfocus on patient autonomy and instead establish authentic, shared decisions, with a role for some clinician control if needed.
Keywords
Introduction
Cancer patients increasingly face preference-sensitive treatment decisions, 1 that is, decisions for which there is medically no optimal strategy, because the evidence for the treatment outcomes is lacking, treatment options have similar outcomes, or patients can be expected to differ in how they weigh the benefits and harms of the options. 2 The ideal model of involving patients in such decisions is considered to be shared decision making (SDM).3–5 In SDM, patients and clinicians work together to make decisions about care that align with the best available medical evidence, the clinician’s expertise, and the values and preferences of the patient.4,6,7 A recent synthesis of SDM consultation models identified the following key components in the vast majority of models: creating choice awareness, describing treatment options, tailoring information, learning about the patient, discussing patient preferences, deliberating, and making or explicitly deferring the decision. 7 SDM is generally considered morally justified, as patients’ autonomy and right to self-determination are supported.4,8 Empirical studies conclude that SDM improves patient outcomes, including satisfaction and, more tentatively, quality of life.9–11
However, some authors have raised concerns that the focus on patient autonomy may overlook patients’ vulnerability, especially shortly after diagnosis.3,12–18 Imposing decision-making responsibility on patients when they are psychologically vulnerable in uncertain situations may lead to emotional distress and conflict.8,19–23 Few studies have specifically examined the potential burden of involving patients in decision making,24,25 nor have they examined to what extent such burden depends on the way the components of SDM are applied by clinicians. Studies show that some men with prostate cancer experience distress due to the uncertainty surrounding the decision, pointing to a lack of clinician guidance.19,26–28 Similarly, women facing decisions regarding breast cancer surgery sometimes express concern and distress about making the right choice. 29
Negative experiences around decision making may also arise when expectations or preferences regarding decisional roles are misaligned between physicians and patients. Notably, some but not all SDM models’ “determining roles in the decision making process” are included. 7 Cancer patients who prefer a limited role in their own care process may particularly experience distress when these preferences are not sufficiently taken into account in the SDM process.30,31 Also, patients who expect a more family-centered decision-making process instead of a patient-centered approach may experience distress when the family is insufficiently involved by the clinician. This misalignment may especially be the case with Western clinicians and patients with non-Western cultural backgrounds, in particular when language or cultural barriers are present. 32
Currently, we lack empirical evidence and in-depth understanding of patients’ perceived burden when involved in decision making. While existing literature offers hypotheses about its causes and solutions, little research has been purposefully initiated to investigate patients’ perspectives on their perceived burden of being faced with a treatment choice. Such research is needed to understand what kind of support could be offered to patients so that patients’ decision-related distress can be mitigated, optimizing the SDM process. To address this gap, we explored the nature and manifestations of burden experienced by patients with early-stage breast and prostate cancer regarding their involvement in decision making. We further aimed to identify patient-perceived causes and potential solutions for their experienced burden.
Methods
Design
A qualitative study using semi-structured one-on-one interviews with patients was conducted. These interviews generated in-depth personal accounts of the decision-making process. The consolidated criteria for reporting qualitative research (COREQ) were used to ensure complete methodological reporting (Appendix 1). 33
Sample and Recruitment
Participants were patients who had been diagnosed with early-stage breast cancer (tumor size <5 cm and ≤3 positive lymph nodes) or early-stage prostate cancer (no metastases outside of the prostate gland) in the past 6 mo. Patients were eligible if they were involved in a treatment choice (either recently or currently) by their clinician and self-reported some degree of burden regarding their involvement in decision making on a screening questionnaire (Appendix 2).
We chose to include early-stage breast and prostate cancer patients as these patients are relatively likely to be confronted with preference-sensitive treatment choices. 1 In the Netherlands, SDM implementation in cancer care is increasingly promoted and embedded in the care for early-stage breast and prostate cancer patients.34–36
Participants were sampled purposefully, to ensure variation regarding potentially relevant characteristics, 37 that is, their self-reported level of experienced burden, age, tumor type, type of treatment decision, and migration background. To further ensure a diverse sample, patients were recruited via 3 different ways: 1) via clinicians in 3 Dutch participating hospitals, 2) via 2 Dutch cancer patient associations (1 breast and 1 prostate), and 3) via a Dutch advocacy organization group for patients and their families with a migration background (Stichting Gezondheid Allochtonen Nederland). Interested patients completed the screening questionnaire digitally or verbally via telephone.
Eligible patients were informed about the study by the researchers, and if they provided initial oral consent, an appointment was made for an interview at the patients’ preferred location (home, hospital, or online via Microsoft Teams). At the time of the interview, patients signed formal informed consent. The total sample size was based on data saturation, meaning that recruitment continued until informational redundancy was achieved (i.e., when no new themes arose in 3 subsequent interviews).38,39
Data Collection
Interviews were conducted by 4 researchers between October 2022 and February 2024. F.L.H. (MSc, background in health sciences and management) and M.J.H (MSc, psychologist), both trained in qualitative interviewing skills, conducted interviews with Dutch-speaking patients. Two care consultants with a non-Western background conducted interviews with Turkish-, Arabic-, and Berber-speaking patients. A semi-structured interviewing guide (Appendix 3) was used, based on the research questions (Table 1). The interview guide was pilot tested with 1 former breast cancer patient. Interviewers kept a reflexive journal capturing their thoughts before, during, and after the interview, to be aware of their own possible bias/assumptions. The interview guide was adapted and discussed with the core project group throughout the data collection based on emerging findings and the reflexive journals. The main changes in the interview guide were, for instance, focusing more on experiences and feelings rather than evaluations of care and focusing more on the choice process instead of care in general. Interviews were audio-recorded with participants’ permission and lasted about 1 h.
Research Questions
Data Analysis
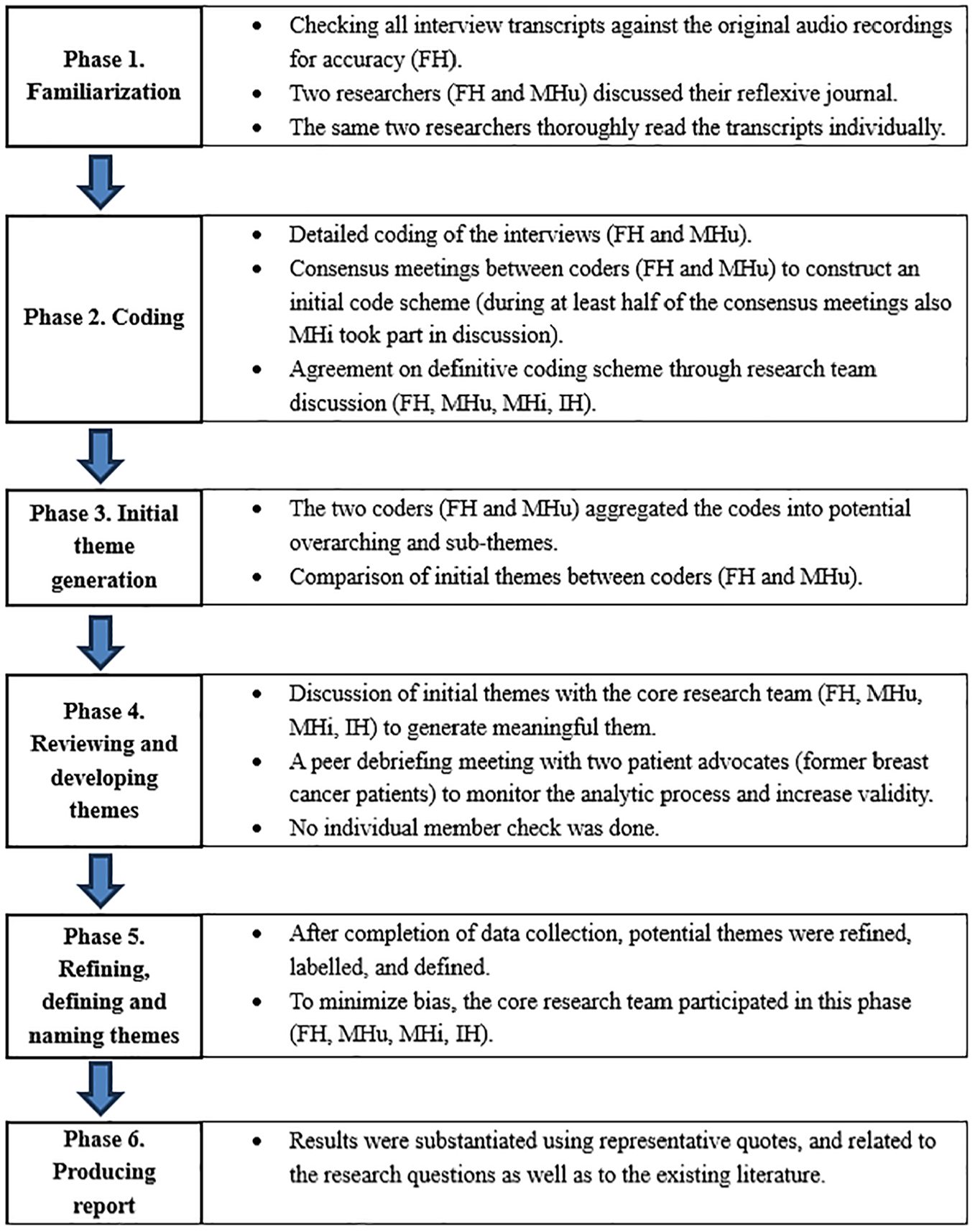
Analysis was based on the 6 phases of reflexive thematic analysis described by Braun and Clarke,40,41 as illustrated in Figure 1. Analysis was mainly inductive, that is, not originating from existing theoretical frameworks but openly mapping experiences. 42 Coding and analysis were performed with MAXQDA 2020 (Verbi software, Marburg, Germany).
Results
Sample Characteristics
In total, 50 patients completed the screening questionnaire, of whom 25 patients did not meet the inclusion criteria. Of those 25 patients, 6 were diagnosed longer than 6 mo ago, 2 patients did not experience a choice, 13 patients did not experience burden regarding their involvement, and 4 patients did not want to participate in the interview after completion of the questionnaire. Eventually, 24 patients were interviewed as 1 patient canceled the interview due to illness. Breast cancer patients (n = 13) faced choices about type of surgery (e.g., breast conserving v. mastectomy), type of breast reconstruction, radiotherapy, hormonal therapy, and/or chemotherapy. Patients with prostate cancer (n = 11) faced choices between active monitoring, surgery, radiotherapy, and hormonal therapy. See Table 2 for participant characteristics.
Participant Characteristics
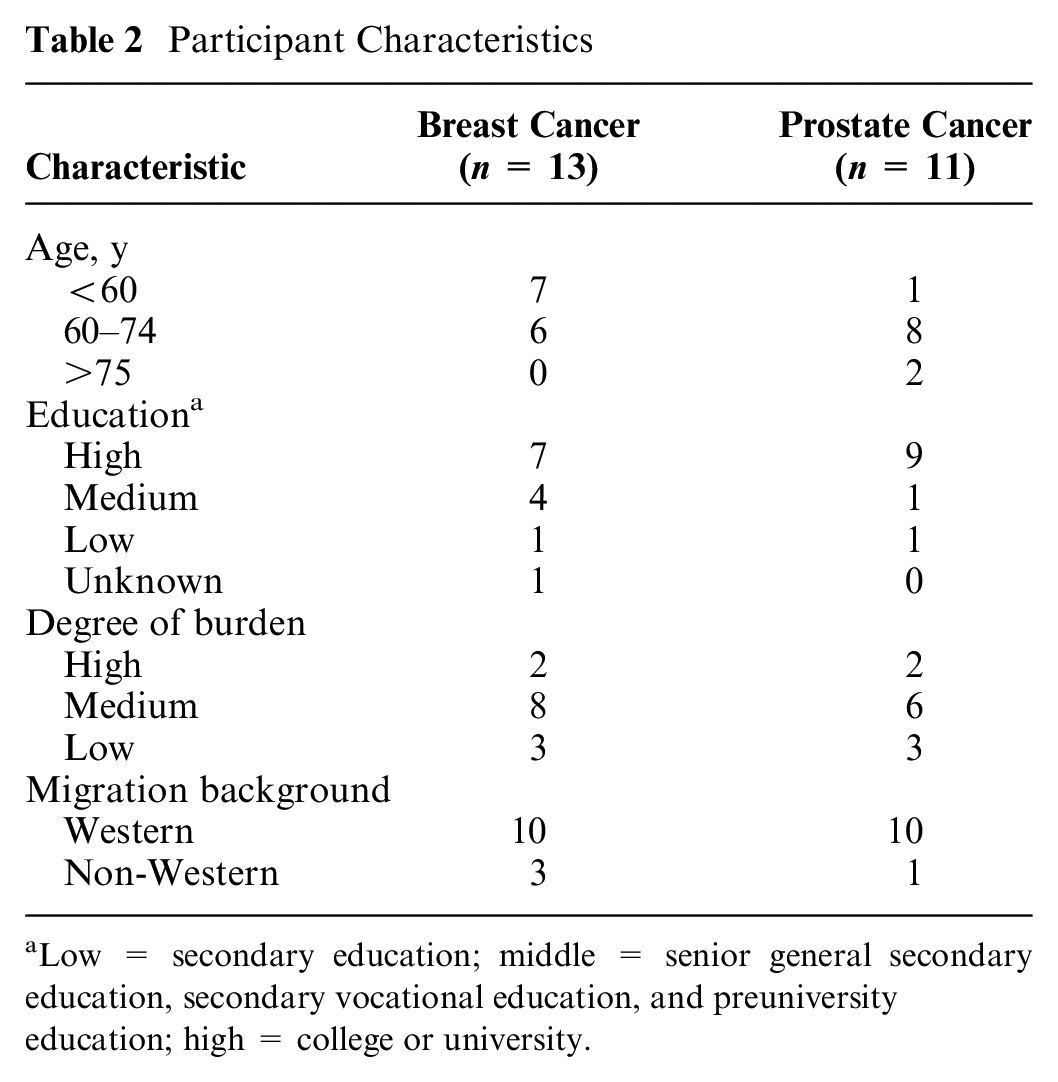
Low = secondary education; middle = senior general secondary education, secondary vocational education, and preuniversity education; high = college or university.
How Do Patients Experience Burden?
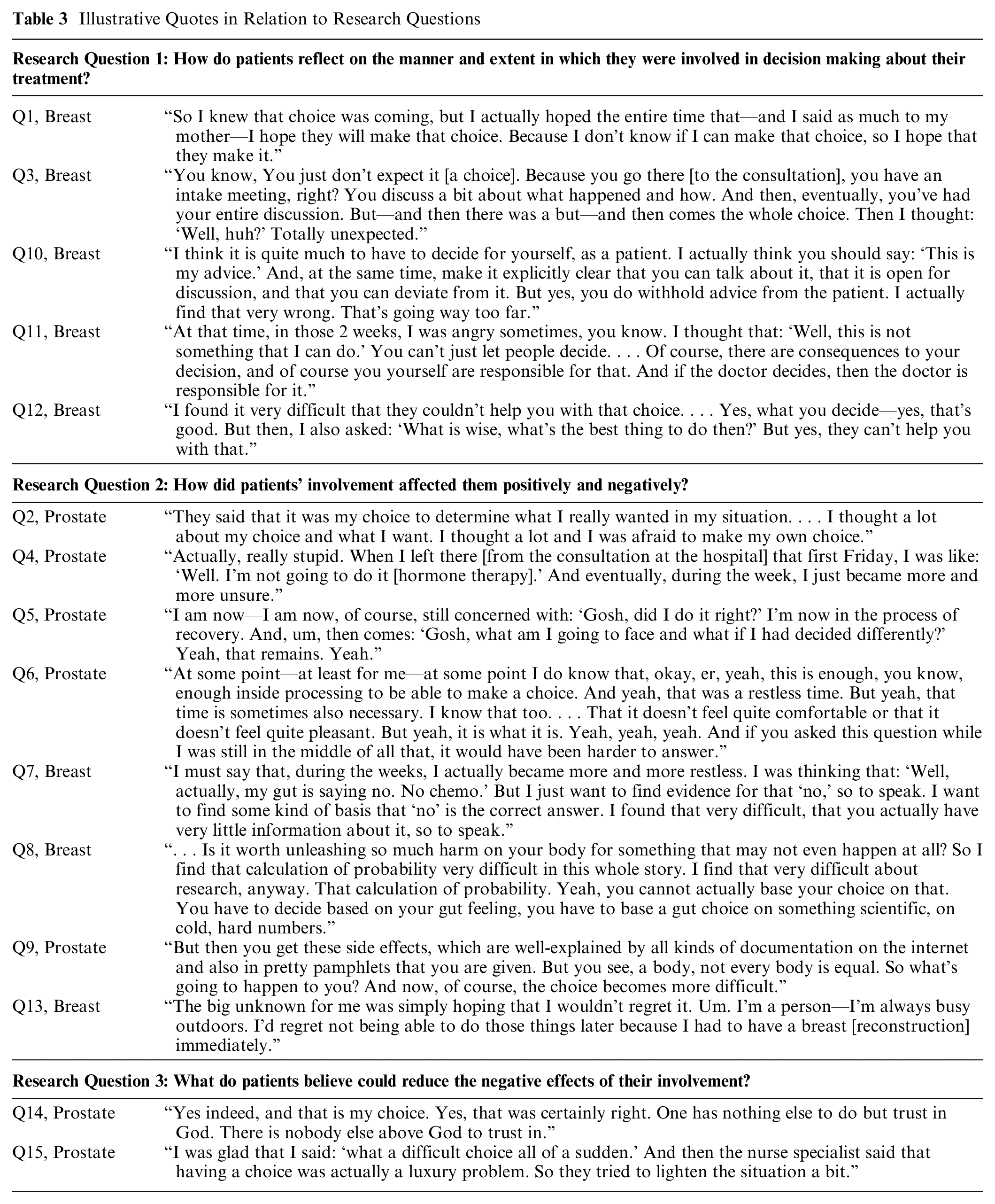
Patients reported experiencing the treatment choice they were facing as a dilemma, although they varied in how difficult the choice was for them, ranging from somewhat to very difficult. Some mentioned that it would have been easier if the clinician had decided for them or if they would not have been presented with a choice at all (Table 3, Q1).
Illustrative Quotes in Relation to Research Questions
Emotional, cognitive, and physical manifestations of burden
Patients reported different ways in which the burden of choice would manifest. Manifestations could be 1) emotional, such as crying, fear, agitation, or being angry; 2) cognitive, such as constantly changing ideas, worry, grinding over the choice, being confused, or being uncertain; or 3) physical, such as sleep problems. These manifestations could go hand in hand (Table 3, Q2).
Patients could feel burdened at different moments throughout the process. This included the moment they were faced with the choice, while being “at home” after being faced with the choice, and/or the period afterward. The burden experienced during the moment they were faced with the choice mainly consisted of confusion. They felt confused when presented with a different choice than expected (as they had searched the internet for information or heard stories from others about specific treatments) or when unexpectedly presented with a choice instead of a treatment advice/proposal (Table 3, Q3). Others experienced burden once they had returned home after the consultation in which they were presented with a choice. These patients explained that during the consultation they felt that they had come to a decision, but upon leaving the hospital or arriving at home, doubts arose about what the “right” choice would be (Table 3, Q4).
Reflections after decision making range from satisfaction to doubts
In the period after the decision-making process, patients were overall satisfied with having been offered a choice despite the experienced decisional burden. However, they varied in how they reflected on the decision-making process. These views ranged from feeling relieved at the end of the decision-making process that the choice was eventually made to experiencing lingering doubts. Also, some patients believed going through this process, with all the difficulties it entailed, was inevitable to arrive at the “right” choice. This difference is reflected in the quotes of 2 prostate cancer patients (Table 3, Q5 and Q6).
Figure 2 shows the schematic display of cancer patient–experienced burden of being involved in treatment decision making.
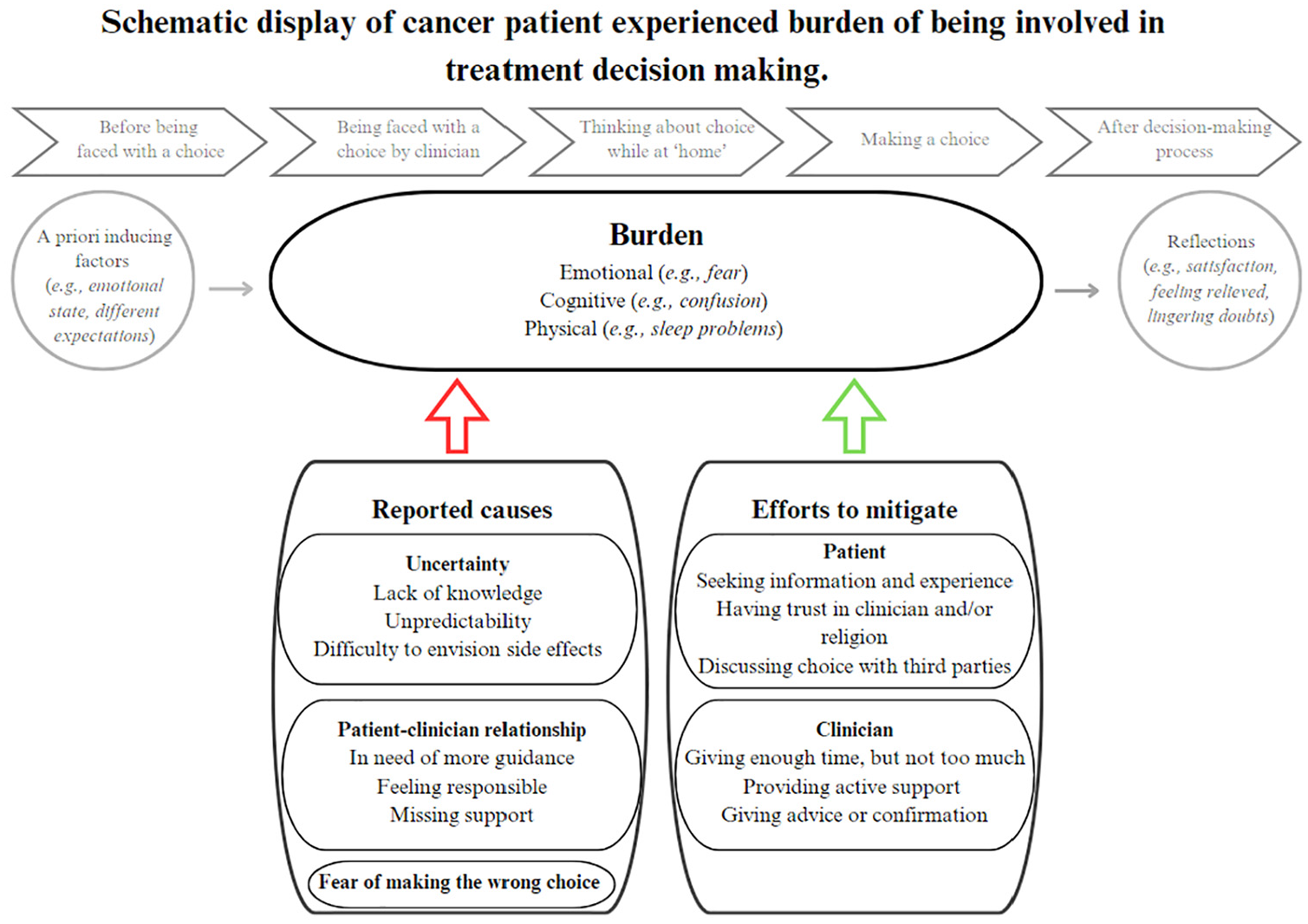
Schematic display of cancer patient–experienced burden of being involved in treatment decision making.
What Induces Patients’ Experience of Burden?
Patients mentioned several factors that induced their experienced burden of involvement in treatment choices.
Uncertainty due to lack of knowledge and unpredictability
First, they explained how various types of uncertainty caused burden. This included an awareness of their own lack of medical knowledge. Making a choice based only on feelings instead on medical information felt wrong (Table 3, Q7). Another type of uncertainty was that patients felt burdened by the unpredictability of survival benefit, treatment effects, and side effects. Patients indicated it was difficult to decide based on statistical data, without specific predictions regarding their individual situation (Table 3, Q8). Especially, when the clinician indicated that treatment efficacy was predicted to be in the “gray” area of beneficence (i.e., medically no preference). Lastly, patients felt uncertainty because they experienced difficulty envisioning side effects. Some patients found it difficult to predict how severe the impact of side effects would be on their health, daily life, and/or relationships, complicating their decisional process (Table 3, Q9). Patients’ uncertainty was influenced by other people’s experiences and opinions. Uncertainty could be exacerbated by others, as patients heard/read various stories with conflicting outcomes from different people or because people suggested a different treatment option than the patient had in mind. Uncertainty could also be alleviated by others, as patients’ treatment choice/preference would be supported by others.
Misalignment in role preferences regarding decision making
A second cause of burden identified by patients was certain aspects of the patient–clinician relationship. Experiences with the division of roles varied between patients, with some patients expressing dissatisfaction with their role within the decision-making process. For example, one experience was that clinicians could have given more guidance and been more directive on what option to choose (Table 3, Q10). Another experience was the wish to not have full responsibility during the decision-making process (Table 3, Q11). Others also would have liked support from their clinicians in the decision making but seemed to believe a clinician is unable to provide such support (Table 3, Q12).
Fear of making the wrong choice
A third cause of burden patients mentioned was fear of making the wrong choice. This fear resulted from the irreversibility of the choice, worry about cancer recurrence, and anticipated regret. Patients’ anticipated regret was reflected in their comments suggesting they would blame themselves if the future outcome was not as desired (Table 3, Q13).
How to mitigate the burden?
Patient efforts: gathering information and trusting the clinician
Ways in which patients dealt with being faced with a choice were various and included seeking information and experiences on the internet and discussing the choice with third parties, for instance, with family and friends but also with other clinicians or their general practitioner. Another way patients dealt with a choice was related to having trust. Some patients seemed to reassure themselves by trusting in the knowledge and experience of their clinician. Especially patients with a migration background mentioned reassuring themselves by trusting Allah. They felt that it was up to Allah whether they would be cured (Table 3, Q14).
Clinician efforts: offering time, support, and advice
Patients indicated 3 ways in which clinicians had helped them in making a choice and mitigated the burden they experienced. First, patients needed enough time, but not too much, to think about which choice to make. If given too much time, the choice became harder as doubts reemerged. Second, clinicians who provided active support in constructing a treatment preference also alleviated patient burden. For example, clinicians offered a new perspective by presenting the choice in a different way (Table 3, Q15), or helped to weigh the options against the patient’s preferences. Third, it helped patients when their clinician gave advice on the options or confirmed that the patient made a “good” choice. This gave the patient peace of mind and helped them put their doubts aside. Also, some patients who did not get any confirmation from their clinician expressed their desire for it to be sure they made the right choice.
Discussion
We gathered detailed accounts of cancer patients’ experienced burden during their involvement in treatment decision making and their views on its causes and solutions. While patients valued being involved in treatment choices, they reported emotional (fear, anger), cognitive (confusion, procrastination), and physical (sleep issues) burden at different stages of the process. Patients attributed their burden to uncertainty, a felt decisional responsibility, fear of making the wrong decision, and insufficient guidance from clinicians.
Burden was experienced at various moments throughout the decision-making process. First, during consultations, several patients reported being unprepared for the presentation of choice, which required a mind shift. This suggests that not all patients expect to be involved in a treatment choice, even when SDM has been advocated in public campaigns in the Netherlands, 43 and most patients nowadays indicate wanting to be involved in medical decisions. 44 Therefore, clinicians might be aware that participation in decision making is not always evident for every patient. Even when patients anticipate having a choice, they may not be fully prepared for SDM, for example, because they lack medical knowledge or have difficulty understanding the information provided.45–47 Patients in our sample indicated that a lack of medical knowledge was related to experiencing distress. Reduced health literacy could further hinder engagement in SDM. 48 Second, burden could be experienced after consultations, when patients were instructed to (re)consider their decision at home. People have different decision styles to cope with a decision, some of which are more likely to induce burden and a sense of abandonment when independently considering a choice.49–51 For example, people who rely on others or are avoidant in making decisions may feel unable to make effective decisions themselves or fear taking on responsibility.
Part of the reported burden may be inevitable, as cancer treatment decision making inherently involves uncertainty and stakes are usually high.3,4,6,8,52 Clinicians will involve patients in decision making only when, from a medical point of view, there are multiple realistic options. To make a decision that aligns with patients’ values and preferences, clinicians have no other choice than to involve the patient in the decision-making process. Uncertainty about the best course of action may create or add to the patient’s awareness of vulnerability after a cancer diagnosis. 8 In our study, such vulnerability manifested in the unease patients felt regarding responsibility and their fear of making the wrong choice.
Our findings, however, also show that part of the burden may be related to how patients are involved in decision making by their clinician. Some patients felt highly responsible, were in need of more guidance, and missed support in the decision-making process. These experiences seem misaligned with SDM as intended, instead aligning with practices of informed decision making.53,54 The informative decision-making model assumes that patient’s values are well defined and known, limiting the physician’s role to providing relevant factual information and executing the patient’s choice. 54 In other words, the conception of patient autonomy in informed decision making is patient control and patient responsibility over decision making, 53 while in SDM, clinician guidance is important. Our results show that such guidance may sometimes fall short, as patients expressed a need for more direction. Some indicated this would help them relieve decisional burden by being able to trust in their clinicians’ expertise. Similarly, previous empirical evidence reiterates that patients’ feeling of engagement and autonomy often go hand in hand with the wish to be cared for by their clinicians. 55 Thus, while clinicians may sometimes approach patients as autonomous, rational decision makers, some patients may require more guidance in the decision-making process. The challenge for clinicians is to balance providing patient autonomy with giving sufficient support.55,56
When it comes to patients’ wish to trust in clinician expertise, clinicians’ main concern might also be to strike the right balance. On one hand, our results show trust is needed to offer guidance and potentially lower patients’ decisional burden. On the other hand, excessive trust may cause dependency on the clinician8,47 and less active participation in the decision-making process. 47 This can become especially problematic when doctors are unaware how such dependency may reduce patients’ autonomous capacity. 8 Ultimately, clinicians may keep in mind that SDM prioritizes that choices align with patient’s needs and preferences, regardless of who eventually makes the final decision.
Conceptual and Practical Implications
In recent SDM models, the emphasis has shifted away from clinicians providing recommendations and/or sharing their professional preferences. 7 This movement signals a drive to enhance patients’ autonomy and right to self-determination. However, the current results highlight the potential unintended negative consequences for the patient if clinicians fully refrain from providing their input. Our findings emphasize the importance of clinicians providing guidance and support in preventing and mitigating patients’ decisional burden. Further, our results also show the importance of explicitly addressing and agreeing on roles in decision making to prevent patients from feeling the responsibility for a decision is imposed on them. Thus, the current study underscores that conceptualizations of SDM should include elements pertaining to the determination of preferred roles and leave room for some physician control in decision making. Figure 3 lists several practical recommendations for clinicians in the context of mitigating a patient’s burden regarding decision making.53,57,58
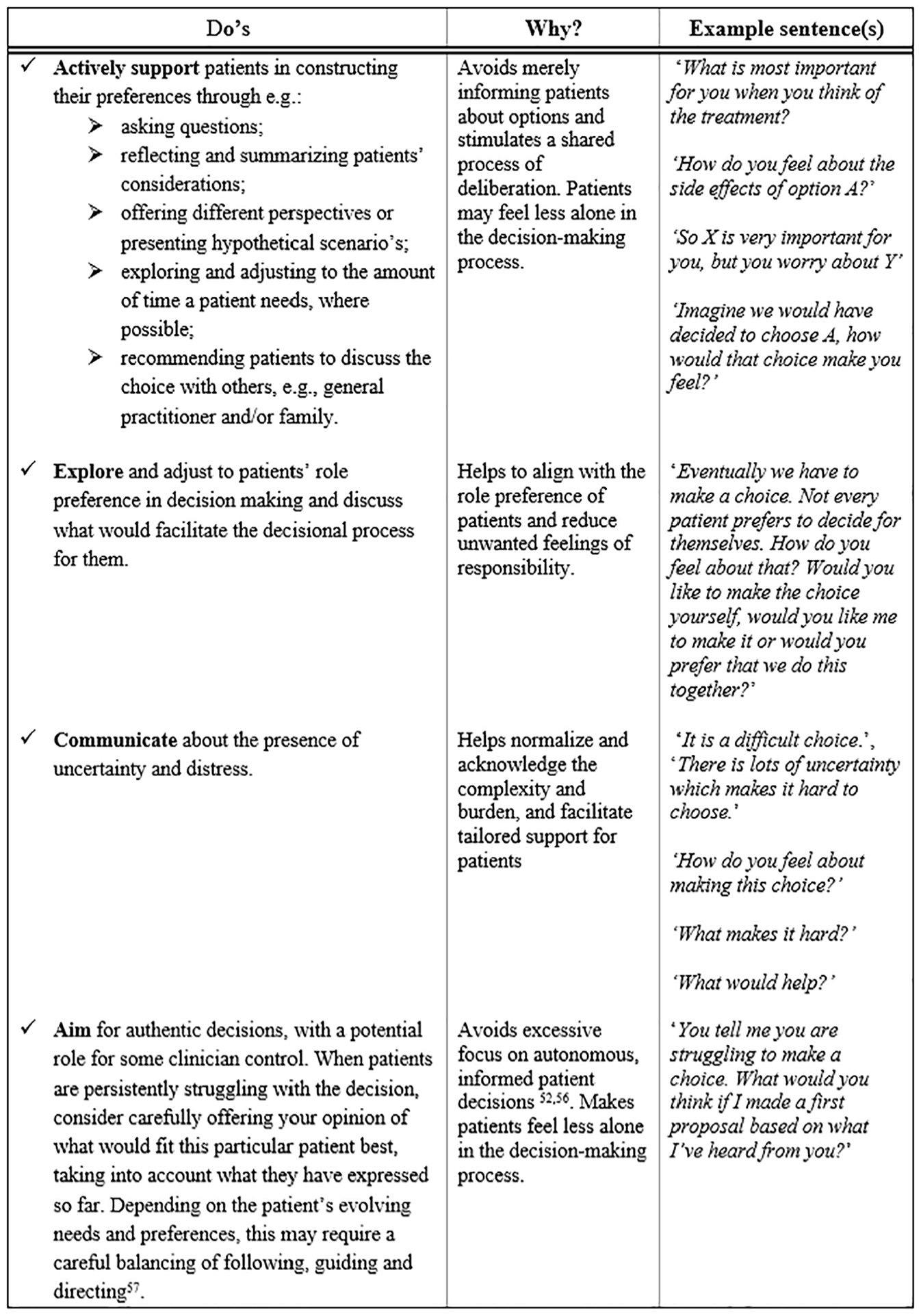
Practical implications for clinicians regarding shared decision making.
Strengths and Limitations
A strength of our approach is that we used researcher triangulation, which increased the validity of our findings and added depth to the phenomenon of interest.59,60 Limitations are, first, that most patients were interviewed after completing the decision-making process. Thus, their reflections may have been affected by the passage of time. Second, despite our inclusion of 4 patients (17% of our sample) with a non-Western migration background, our sample consisted largely of highly educated, native Dutch people. Additional perspectives of lower educated patients and patients with a non-Western background are needed, as experienced burden may be affected by language barriers and cultural differences. 32 Finally, in interpreting the results, readers should be aware that we included only patients with self-reported burden and only in the context of curative breast and prostate cancer. Therefore, these findings may not generalize to other populations. We did not focus on potential differences in patients’ experiences of burden between various settings. Future research could explore these, for example, between cancer types and different types of decisions associated with them and/or curative versus palliative setting. In addition, it would be interesting to compare differences in perspectives between patients who experienced burden and those who did not, to gain more insights into predictors of burden.
Conclusion
This study provides important insights into cancer patients’ experiences of burden when being involved in treatment decision making. Experienced burden varied in nature and manifested at various moments throughout the decision-making process. The results suggest that the burden can be partly explained by how patients are involved in treatment decision making, highlighting the importance of active support and guidance from clinicians in the decision-making process.
Supplemental Material
sj-docx-1-mdm-10.1177_0272989X251334979 – Supplemental material for Cancer Patients’ Experiences of Burden when Involved in Treatment Decision Making
Supplemental material, sj-docx-1-mdm-10.1177_0272989X251334979 for Cancer Patients’ Experiences of Burden when Involved in Treatment Decision Making by Fiorella L. Huijgens, Marij A. Hillen, Mette J. Huisinga, André N. Vis, Corinne N. Tillier, Hester S. A. Oldenburg, Gwen M. P. Diepenhorst and Inge Henselmans in Medical Decision Making
Footnotes
Acknowledgements
First, we would like to thank all participants for sharing their experiences, feelings, and thoughts with us on this delicate topic. Second, we would like to thank the patient partners for thinking along with us on setting up the study and pilot testing the interview guide. Further, we want to thank the clinicians of the 3 participating hospitals (especially the clinicians and specialized nurses), the cancer patient associations (Borstkankervereniging Nederland and Prostaatkankerstichting) who helped in the selection procedure of patients. Lastly, we would like to thank S. Laaboudi and N. Lale-Kahraman from Stichting Gezondheid Allochtonen Nederland for their help in recruiting and interviewing patients with a non-Western migration background.
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support for this study was provided by a grant from the Dutch Cancer Society (KWF Kankerbestrijding) and partly by Amsterdam Public Health, Personalized Medicine who financially supported the interviews with non-Western patients. No generative AI was used in any portion of the manuscript writing.
Authors’ Note
• Amsterdam Public Health annual meeting, Amsterdam, Netherlands, 2023, poster presentation (preliminary results)
• International Shared Decision Making conference, Lausanne, Switzerland, 2024, oral presentation
Ethical Considerations
The Medical Ethics Committee AMC approved this study (reference No. W22_260 # 22.317).
Consent to Participate
Informed consent to participate was written.
Consent for Publication
Informed consent for publication was provided by the participants.
Data Availability
Research methods are presented in Table 1, Figure 1, Appendix 2, and Appendix 3. Anonymized illustrative quotes used for the analyses are presented in ![]() . Privacy-sensitive data (interviews) will not be shared.
. Privacy-sensitive data (interviews) will not be shared.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.