
Abstract
Health misinformation has long impacted public health, influencing behaviours and adherence to guidelines. Young people are one of the social groups at the centre of health communication in the digital age; they are digital ‘informavores’, meaning they actively seek out, gather, consume and share information to meet various needs. This study examines how young adults (aged 18–30) in urban locations in Nigeria navigated COVID-19 misinformation and the underlying interdependencies this implicates. Drawing on social cognitive theory, the study takes a qualitative approach, collecting data using focus groups and individual semi-structured interviews. Findings from the critical thematic analysis confirm the severity, virality and velocity with which false information about the novel coronavirus spread in parts of the country. Besides, the results reveal that the drivers of misinformation included the government, politicians, bloggers, social media influencers and citizen journalists. Young adults utilized unique verification and correction strategies, such as deliberate scepticism and curiosity, social listening and eavesdropping, personal experience and peer or citizen fact-checking. A chain of ‘interdependencies’ were fundamental to these experiences, including (inter)personal and cultural intermediaries, religion, politics, socioeconomic status, affect and emotions, among others. Young adults advocated for a proactive government, media collaboration, ethics of care and media and information literacy interventions to combat health misinformation. The findings align with the World Health Organization's public health research agenda for managing health misinformation from a sociological point of view, with the aim to foster evidence-based intervention.
Keywords
Introduction
People commonly use the internet and social media platforms when seeking medical information and engaging in health communication. Unmet medical needs, resulting largely from financial difficulties, complexity of health conditions such as chronic illnesses, and other specific reasons, have led to a rise in health information searches on the internet, driven by the diverse situations encountered by patients and their families (Oh and Cho, 2015). However, relying on digital technology for easy access to medical information results in several issues, and during the COVID-19 pandemic, it contributed to the circulation of health misinformation (or as used interchangeably in parts of this paper, health-related fake news, health-related misinformation or simply false information on health). Apuke and Omar (2021: 3) note that ‘the affordances that social media provide, along with the abundance of information on COVID-19, contributed to fake news circulation’. In a world impacted by an escalating ‘infocalypse’, defined by Schick (2020) as a critical crisis of misinformation exacerbated by the rise of advanced technologies such as deep fakes and synthetic media, health misinformation is a subset of the larger problem of information disorders affecting populations in African countries, as in other parts of the world. Spies (2020) argues that to explore the extent and effects of misinformation, attention must be paid to a number of factors, including people's media and information consumption, technological affordances, factors relating to individual and human behaviours, information cascades on social networks and media amplification.
Health-related misinformation can delay or prevent effective care, and in some cases it endangers the lives of individuals. It can also limit the effectiveness of scientific communication from medical experts and health authorities. These stakeholders face increasing challenges in the age of fake news because they do not ‘focus on simply disseminating the message but also defend the evidence from challenges to the validity and interpretation of their research, including being proactive enough to ensure that unsubstantiated messages do not compete with the correct message’ (Merchant and Asch, 2018). Further, on social media, Chou et al. (2018) argue that ‘the spread of health-related misinformation is exacerbated by information silos and echo chamber effects as social media feeds are personally curated and tailored to individual beliefs, partisan bias, and identity’.
Since the outbreak of COVID-19 as a global health pandemic, reliance on digital technologies has meant that ‘people access a wider range of sources and “alternative facts”, some of which are at odds with official advice, misleading, or simply false’ (Newman et al., 2020: 9). The COVID-19 pandemic resulted in both a ‘misinfodemic’ and a ‘disinfodemic’. The former refers to the rapid and widespread dissemination of false, inaccurate or misleading information related to a particular topic or disease, often during a pandemic or public health crisis (Apetrei et al., 2022). The latter, on the other hand, is the insidious, toxic and negative impact of the collision of false information and the infodemic, which is disempowering, life-threatening and sows polarities and uncertainties (UNESCO, 2020). Information disorders, whether scientific or medical, are hindering public health efforts (Ahmed et al., 2020; Scales et al., 2021).
Recent research has focused on the consumption and reception of false information, as well as motivations for consuming and sharing false information, but this has largely been concentrated in Western contexts. The current study adds to the body of knowledge in this area by focusing on the unique ways in which young people negotiated and challenged and/or succumbed to health misinformation. Although false information in these contexts is rife, worrying and growing, there is an insufficient number of studies on misinformation in sub-Saharan Africa in general (Madrid-Morales et al., 2021; Wasserman and Madrid-Morales, 2019), and on health misinformation in particular (Adjin-Tettey, 2022; Ncube and Mare, 2022). Given the vast amount of information and conspiracy theories about COVID-19, including its origins, dissemination, fatality rates, treatment, health and safety precautions, and vaccines, it is a critical health issue deserving of research attention from a social science perspective.
Health information disorder: The case of COVID-19
Health misinformation is a part of the broader problem of information disorder in an information ecosystem increasingly impacted by ubiquitous internet use, digital belonging and social media. The term health misinformation refers to claims about health promotion and/or disease control that are false due to contradicting expert consensus and/or the best available evidence at the time. Such claims can also be considered inaccurate because they rely on incomplete evidence or are unsubstantiated because of a lack of evidence (Nan et al., 2023; Wang et al., 2022). The COVID-19 pandemic created an environment where misinformation and conspiracy theories were easily propagated across the world (Ashley et al., 2022). Misinformation posed a problem to public health long before the pandemic, often impacting people's health behaviours, the risks to their health they are willing to take, and whether or not they follow public health guidelines (Scales et al., 2021). However, it became more pronounced during the COVID-19 pandemic. In many ways, such COVID-19-related misinformation was to be expected: there was a lot of uncertainty and ambiguity as the disease was unknown and knowledge about it was increasing by the day. The virus itself was changing, meaning that today's knowledge could be outdated tomorrow.
According to the 2022 Digital News Report (Newman, 2022), 72% of people in Nigeria reported that they encountered more false information about COVID-19 than about politics. The report confirms that COVID-19 health misinformation, including anti-vaccination misinformation, was the most widespread type of misinformation that people encountered between 2021 and 2022. It was much more prevalent than political misinformation, which is unexpected given that political news has always dominated Nigerian public discourse due to the numerous political issues in the country, including corruption, economic hardship and ethnic polarisation.
Online misinformation and conspiracy theories spread rapidly, extensively and virally from the beginning of the pandemic. Individuals in the United States who relied on social media platforms to find tailored health information often encountered inaccurate and deceptive content that promoted false beliefs and hazardous actions in relation to COVID-19 (McKinley and Lauby, 2021). In the Netherlands, Meppelink et al. (2022: 7) found that ‘overall, the use of platform media influenced the likelihood of believing in one of the COVID-19-related misperceptions’. The same applied in African countries, as supported by evidence from Ghana (Adjin-Tettey, 2022), Zimbabwe (Ncube and Mare, 2022) and Nigeria (Uzuegbunam and Ononiwu, 2023). In particular, Nigeria, the largest African country by population, has experienced numerous instances of widespread misinformation and disinformation, particularly during ‘hot health crises’ (Kilgo et al., 2018: 2), including polio, Ebola virus disease, Lassa fever and the COVID-19 virus. During these health incidents, false information spread both offline and on social media platforms. Since the Ebola outbreak in 2014, the Nigerian Centre for Democracy and Development (CDD) has been studying the patterns of false information propagated throughout the country. It has confirmed that Nigeria has experienced widespread cases of misinformation with serious implications (CDD, 2020). During the Ebola outbreak, for instance, numerous myths abounded (CDD, 2020; Oyeyemi et al., 2014), such as bathing in warm, salty and Dettol-infused water being effective in preventing the disease; chewing kola nuts being effective in preventing the disease; and utilizing homeopathic treatments made from natural plants being effective at healing the disease, among others.
Similar types of misinformation and disinformation continued to circulate in the COVID-19 era, such as the following: the coronavirus is a scientific fabrication; the coronavirus is a ‘plandemic’ (Kearney et al., 2020)—the notion that the COVID-19 pandemic was planned by world powers; wine, garlic, pepper, regular sex, chloroquine and men shaving their beards may be effective at treating the virus; the ‘African gene’ and hot temperatures in regions of Africa render African people immune to the virus; and so on. In Nigeria, according to the CDD, the majority of such false news was disseminated via gossip blogs, WhatsApp, sensational magazines and social media, particularly Twitter and Facebook. Factors such as widespread distrust in the government, weak public institutions and information sources, low social capital, inaccessible healthcare due to cost and infrastructural decay, and lack of responsiveness made citizens susceptible to alternative sources of information and remediation (Apuke and Omar, 2021; Gagliardone et al., 2021; Uwalaka et al., 2021). Furthermore, due to widespread fear, anxiety and uncertainty about local transmissions and multiple infections, a variety of actors, including opinion leaders, politicians, influencers and social commentators, disseminated propagandistic information through official sources, social media and word of mouth, which has been corroborated by research (Apuke and Omar, 2021; Uwalaka et al., 2021).
There were religious and cultural anxieties and conspiracies surrounding the COVID-19 vaccines and their efficacy. This led to scepticism and a lack of enthusiasm for vaccination, even as developing countries struggled to secure vaccines in the face of global vaccine nationalism and vaccine imperialism (Uzuegbunam, 2021). The largely unregulated online environment encouraged the dissemination of such conspiracies, rumours and hoaxes to unsuspecting audiences who were already anxious and fearful due to the COVID-19 virus (Uzuegbunam, 2021). This had an adverse impact on disease control and management, as also seen in prior outbreaks like SARS-CoV-2, polio and Ebola in the continent. It resulted in incidences of people ignoring scientific information and government advice about social distancing and other public health interventions, as well as refusing to be vaccinated (Ahmed et al., 2020). Despite a limited number of studies focusing on the Nigerian context, very scant evidence exists about how young people navigated health misinformation related to COVID-19, as well as the associated interdependent factors in their interaction with health information and false information on COVID-19. This study, therefore, explores the following specific research questions to fill this gap:
How did young adults understand, negotiate and share health-related misinformation (including whether they employed any correction practices in the process)? What were the associated interdependencies in their interaction with health misinformation? How did young adults frame the perceived or experiential impact of, and measures required to combat, health misinformation in general and COVID-19-related misinformation in particular?
Theorizing young people's negotiation of health (mis)information and its underlying interdependencies
This study uses social cognitive theory as a foundation to examine the process of negotiating health misinformation and its associated interdependencies in a pandemic. Social cognitive theory was popularized in 1986 by Albert Bandura, who focused on the complex and ever-changing relationship between individuals, their behaviours and the sociocultural contexts in which they are situated. Social cognitive theory posits that people's ideas and behaviours are inevitably influenced and strengthened by social factors. In this context, social factors encompass individuals’ backgrounds, level of exposure and past experiences. This study utilizes this idea to analyse how young adults navigated health misinformation throughout the COVID-19 pandemic. More specifically, the external factors and personal characteristics of young adults, including their existing knowledge, beliefs, and social and cultural resources, could have influenced how they received, engaged with and navigated health (mis)information, even during health crises such as the pandemic. The social cognitive theoretical framework has been successfully applied in studies examining health behaviours and health promotion (Bandura, 2004; Islam et al., 2023; Kelder et al., 2015; Luszczynska and Schwarzer, 2020).
Bandura (2009) proposed that social cognitive theory can be applied to understand how media content and information affect people's daily lives. According to this theory, humans are not depicted as lacking power when exposed to media content; instead, they possess the ability to determine how they are influenced by such content and information. This contradicts the earlier magic bullet or hypodermic needle model (Ahmad et al., 2023), which held that media content may have a powerful and instantaneous influence on users and viewers. Bandura (2009) contends that it is crucial to understand the mechanisms through which symbolic communication influences human cognition, emotion and behaviour, given the substantial influence of mass media on society. The social cognitive framework thus provides an insight into the interaction between cognitive and affective elements, behavioural patterns and environmental events in assessing how young people navigated COVID-19 misinformation in Nigeria.
Methods and protocol
Tremblay et al. (2021) contend that while efforts have been made to address the COVID-19 health crisis through clinical trials and epidemiological studies, insufficient focus has been placed on understanding the specific ethnographic (sociological) experiences and interpretations associated with COVID-19, as well as the strategies employed to reduce its transmission among affected populations. The current study explores qualitative insights provided by young adults in Nigeria, aiming to obtain a deeper understanding of their lived realities with health misinformation during the pandemic. Both focus groups and individual semi-structured interviews were employed to address the research questions. Group interviews are highly effective for studying shared life experiences, while semi-structured interviews are the predominant strategy for collecting qualitative data in health research (DeJonckheere and Vaughn, 2019). Conducting in-depth semi-structured interviews proved to be an appropriate method for further exploring the themes emerging from the focus groups on an individual level without the influence of group dynamics such as uncertainty, timidity and unease that arise while speaking in front of others. Interview participants were chosen from the group members after each group discussion was completed.
Scholars such as Bosch (2022) advocate for prioritizing qualitative approaches and methods, such as interviews and focus groups, in order to gain a deeper understanding of users’ daily activities. Since social media and messaging platforms like WhatsApp have policies that hinder effective computational social science research on information reception dynamics, researchers can find value in using qualitative-ethnographic methods such as focus groups and interviews (Bosch, 2022). Although these methods are typically time-consuming compared to quantitative methods such as surveys, they can be considered rigorous and capable of generating deep, thick qualitative data. Qualitative approaches offer the opportunity to document the dissemination of information across different social media platforms and its reciprocal effects (Spies, 2020), as well as the interdependencies that arise when examining human interaction with the physical environment.
A total of four focus groups, consisting of 33 young adults, were conducted (see Table 1). Of the 17 males and 16 females that took part in this study, 28 participants were between the ages of 26 and 30, with five between the ages of 18 and 25. In terms of level of education, 27 participants had bachelor's degrees, while six were either master's degree holders or enrolled in a master's programme. Thus, there was an equal gender distribution of participants; the majority of them were in their late 20s and 30s; and most of them could be deemed suitably educated.
Participants’ demographic information.
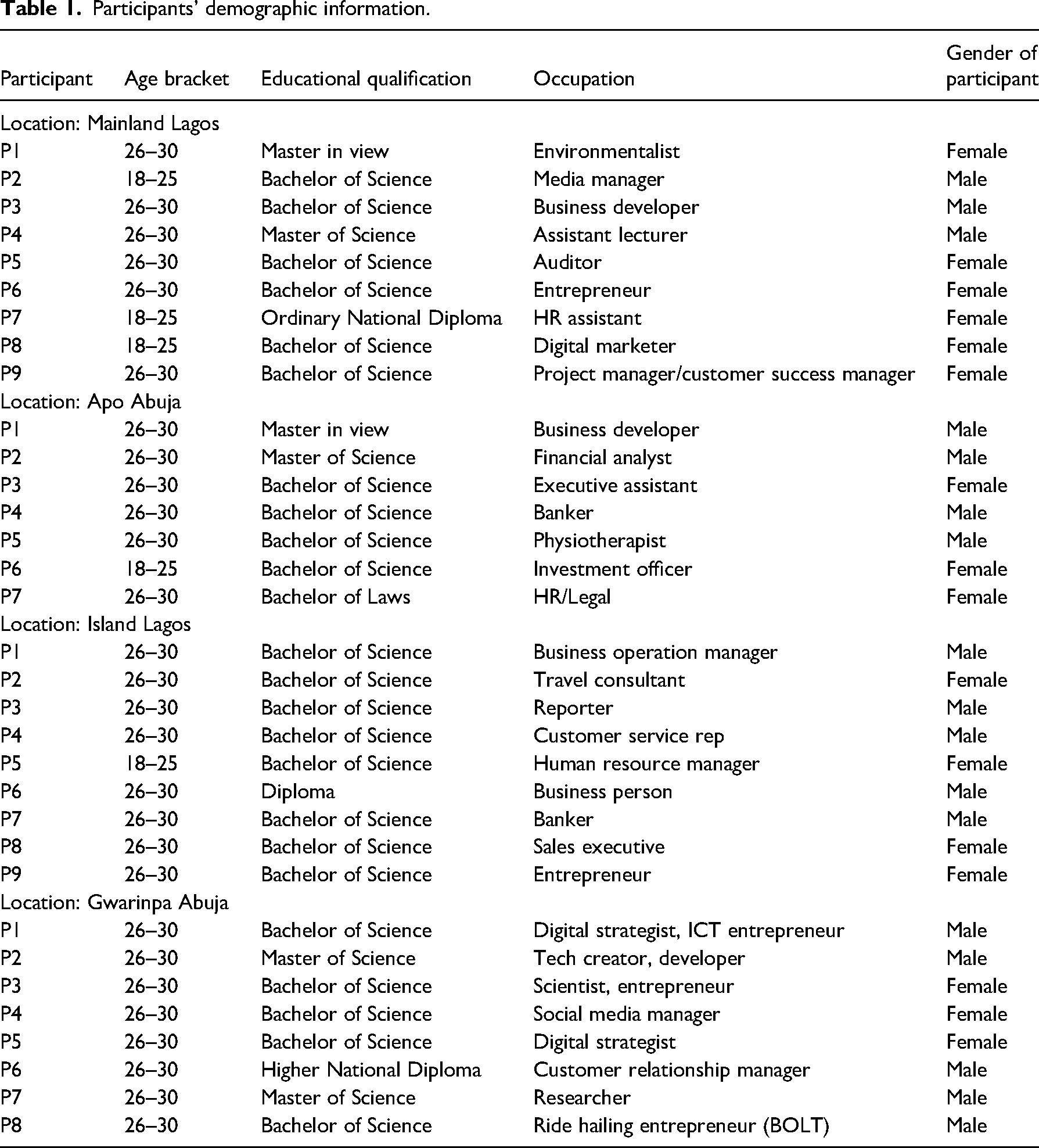
Participants’ demographic information.
Two focus groups took place in FCT-Abuja, while the other two were held in Lagos. Furthermore, an additional eight individual interviews were conducted to further explore the emergent themes that came up during the group discussions. Purposive sampling was used during the recruiting process in order to produce a loose representation (Lynch, 2013). The emphasis was placed on selecting individuals who were either enrolled in colleges or universities or were professionally employed or self-employed. The participants were selected using the snowball sampling technique. Four trained research assistants were employed to assist in recruiting potential volunteers in both cities. Despite the relatively small sample size, the conversations produced were of high quality and effectively addressed the research questions. There was a wide range of diversity among the participants regarding educational background, socioeconomic status, gender, ethnicity and geographical location. The fieldwork was conducted in person in December 2021, while adhering to the prevailing COVID-19 regulations at the time and overcoming challenges such as time constraints and physical distancing which impacted qualitative studies during the pandemic (Tremblay et al., 2021).
The study requested and received approval from the ethics review board of the Institute for Humanities in Africa at the University of Cape Town, South Africa. Ethical guidelines were followed for information sharing, informed consent, confidentiality, maleficence and material compensation (Uzuegbunam, 2022). The data for this paper were obtained from a broader study that included a range of questions posed to participants (see the Appendices). These questions covered topics such as participants’ health information-seeking practices, health-related behaviours and attitudes, health-related misinfodemics, reception of misinformation and combating health misinformation.
Critical thematic analysis was used to analyse the coded data, which is a highly flexible method that allows for the identification of themes and patterns in various types of texts, such as interviews and ethnography (Lawless and Chen, 2019). The coding technique consisted of three steps: initial data-driven inductive coding, followed by theory-driven deductive coding and a critical evaluation. We began with a data-driven approach, where we closely examined the focus group and interview transcripts to identify recurring patterns, repetitions and relevance to the topic. This step was crucial for uncovering themes that naturally emerged from the data without imposing preconceived categories. Following the inductive phase, we applied a theory-driven approach. Here, we used the social cognitive theoretical framework to further refine and categorize the themes identified in the initial coding. This step ensured that the themes were not only grounded in the data but also connected to theory. Each identified theme was then critically evaluated to understand its significance and implications within the broader social context. This involved questioning the power dynamics, social structures and other salient factors, which we have termed ‘interdependencies’ in the paper, that the themes represented.
The coding process was conducted using NVivo software, version 1.5, released in 2021. This facilitated the coding process by allowing efficient retrieval and organization of codes, concepts and causal chains. The capabilities of the software enabled a systematic and rigorous analysis, ensuring that the themes were well supported by the data.
The qualitative data, consisting of personal interviews and focus groups, were analysed collectively due to the lack of rationale for analysing the same kind of qualitative data independently, and due to word count considerations. Critical thematic analysis enabled the identification of themes and patterns in diverse qualitative texts, such as interviews and focus groups, without the need for their explicit separation. This can be attributed to parallels in the questions posed during the interviews and focus groups. The interviews aimed to ascertain whether there were any disparities between participants’ responses and behaviours in a group setting and their individual responses to similar questions. While the interviews provided a platform for more open expression, the thoughts expressed did not deviate considerably from the themes that arose during the group discussions. However, some participants included more detail about their experiences and spoke in a more relaxed manner than during the group discussions.
The following thematic analysis shows the complex and intertwined range of discourses and issues that emerged from the young adults’ experiences with various forms of health misinformation, whether familial, (inter)personal or societal, as well as the interdependent factors underlying them. Young adults’ self-efficacy in handling the pandemic and its consequent misinfodemic was evident throughout the interaction with them and their interaction with each other. Within the framework of Bandura's social cognitive theory, the experiences of young people in Nigeria during the COVID-19 pandemic can be seen as a complex and nuanced interaction of personal, interpersonal, behavioural and environmental factors. Their narratives, which are examined in the following analysis, provide insight into their cognitive processing of the pandemic.
Understanding, negotiating and sharing health misinformation (RQ1)
Viral fake news on COVID-19 in Nigeria
Young adults in Nigeria affirmed the virality and velocity with which false information around the novel coronavirus spread in parts of the country, from urban, peri-urban to rural locations. This was rife from the beginning of the pandemic to the later stages. Several viral fake news that circulated during the initial stages of the pandemic were recounted by the young adults, including those purporting that the virus was a figment of some dubious people's imagination; that alcohol could prevent one from contracting the virus; and that the hot and humid weather of most African countries will provide immunity from the virus (see Atuire et al., 2021). Bloggers and content creators who used such fake news to drive traffic to their sites or accounts in order to trend, the government and its opponents, social media influencers, so-called citizen journalists, religious influencers who promised miraculous healing, and vendors of orthodox medicines who promised cures for the disease were all mentioned by participants as specific misinformers.
One of the most widely circulated viral fake stories in Nigeria linked the COVID-19 virus and vaccines to the 5G network and ultimately to the notion of a satanic mark of ‘666’ (the Anti-Christ), which many claimed was promised in the Bible as a harbinger of the ‘end times’ (Bruns et al., 2022). Linked to this idea was the viral fake story ‘that the virus was a mass destructive, biotech weapon’ meant to depopulate the world, especially Africans (FGD, Participant 7, Gwarimpa, Abuja). There were accounts of debates around whether the US or China was responsible for the pandemic, including the fact that both countries have been at loggerheads over who has more global influence. President Trump's constant vilification of China and his accusatory tone, labelling China as the architect of the coronavirus at the time, did not help matters and deepened the impact of such hoaxes (McKinley and Lauby, 2021). The participants tended to believe a lot of information originating from America. Their accounts indicate that there were two points in time where linking the virus and vaccines with a satanic agenda by powerful world governments grew more prominent locally: first, when 5G masts were mounted in some cities; and second, when the federal government and some state governments mandated compulsory vaccination for civil servants. In defence of people's concerns, compulsory vaccination only confirmed their suspicions about a secret agenda to bring about ‘a new world order’ and take over the world (Gassner, 2022), as warned by many Christian pastors who were pushing this narrative to their followers (Obadare, 2022).
The participants confirmed the role played by churches in perpetuating the narrative of a ‘plandemic’ (Kearney et al., 2020) and the spread of fictitious information about the pandemic. One participant in FCT-Abuja recounted how, just before coming to the focus group meeting, she had been to her church for an event and the pastor showed the congregation a YouTube video ‘where the vice president of the United States was saying that people who have died had taken the vaccine from COVID-19, something like that’. This participant became suspicious of the integrity of this message when it dawned on her that the pastor ‘didn’t give us the preceding and concluding part of the video, just that part’, thus confirming her fears of possible decontextualization or repurposing of content. As the young people noted, with Nigeria being a very conservative country, religion plays a huge role in disseminating important information and assisting people in making rational important decisions in their everyday lives. People take the words of their religious leaders very seriously and will often follow their guidance without questioning it. According to Alsmadi et al. (2021), religion and political orientation, both important aspects related to misinformation, can easily make people completely disagree with a specific news item or claim, and they can unintentionally spread misinformation, believing it to be true.
A plethora of other false information circulated about the COVID-19 vaccinations. There was widespread circulation of viral videos and messages claiming that the COVID-19 vaccination would generate electric current and magnetic ions in the recipient's body. These anecdotes were recounted by numerous participants at different venues in FCT-Abuja and Lagos. Additional viral conspiracy theories regarding vaccines included the notion that they are utilized to implant persistent ailments in individuals, the belief that receiving the vaccine would lead to a quicker death compared to contracting COVID-19, or that death will occur within a few years of taking the vaccine.
Confronting, negotiating and sharing health misinformation
A significant number of the young adults encountered various types of health misinformation regarding COVID-19, primarily through popular social media, video-sharing platforms and instant messaging apps like WhatsApp, as well as through informal channels such as word of mouth from peers, associates and family members. Most fake news on COVID-19 were believed to have started online and then moved to offline spaces—‘when people consume it online, they use word of mouth to spread it to other people’ (FGD, Participant 1, Lagos Island). One participant likened the spread of such false information to a drop of water which could turn into an ocean. To the young adults, false information spreads faster and is more likely to be believed than accurate or good information because of its nature to be out of the ordinary. Many of the viral fake news were described as ridiculous, dramatic and shocking but, at the same time, sometimes believable.
While some of the participants stated that they might consider the information (note that this is different from outright believing the information and acting on it), they would not share or broadcast it. They did not see it as their job to share information that they were unsure of with people, either to warn them or for other reasons. This contrasts with the findings of the study by Uzuegbunam and Ononiwu (2023), which found that older adults’ motivations for sharing health-related COVID-19 news included a sense of concern about the pandemic and/or a desire to create awareness of the dangers of the virus. However, some of the participants did share COVID-19-related information they thought was funny and satirical, or information they were sure of, especially from sources such as the Nigerian Centre for Disease Control, the World Health Organization (WHO) and trusted international and local news media. Other reasons they would not share unverified and controversial information included fear of damaging the trust their close circles have in them; concerns about being perceived as a peddler of false information by those they care about; and worries about spreading fear. The young adults also would not share information that is circulating as a result of hearsay from other people.
Due to the contested and sensitive nature of the topic of vaccines and vaccination, a lot of virulent information was spread during the pandemic, which led to some clearly risky behaviours, even among educated people. With such varied versions of information, especially on vaccines and vaccination, ‘people were talking about it and that is the reason that made people not to have taken this vaccine’ (FGD, Participant 1, Lagos Island, Lagos). Some young adults shared a few pieces of circulating false information, mostly myths, around the vaccines. The reason for sharing this was because the information came from a prominent Nigerian Pentecostal preacher who was openly anti-vax and believed the pandemic was a ‘plandemic’. One of the participants had shared such hoaxes on WhatsApp, and although they no longer believed in the veracity of this information at the time of the interview, they insisted that ‘whether they are fake or not is yet to be seen or to be known because they are still coming’, while further asserting that ‘what you call fake news today may turn out to be real news tomorrow’.
Some individuals who had previously spread incorrect information found it challenging to retract it or warn their recipients that the content was wrong. This difficulty sometimes stemmed from feelings of guilt and shame. An instance was when a participant conveyed a piece of misinformation (unrelated to COVID-19) regarding receiving calls from unfamiliar numbers, claiming that answering such calls would result in death. The participant disseminated the information to a large number of people within her social network. Upon discovering that the information was false, she experienced a combination of anger and embarrassment yet was unable to retract her previous statement. I wasn’t the direct source, but I was now part of it. So for the fact that I was part of the people who shared it, even shared it on the major groups where there were about 300 people … I was very angry with myself. (FGD, Participant 4, Gwarimpa, Abuja)
Social listening or social eavesdropping, decontextualization, recontextualization and repurposing emerged as factors when confronting and negotiating health misinformation on COVID-19. Firstly, the young adults practised social listening as a method of dealing with health information. Social listening occurs when people communicate and deliberately listen to others via mediated, electronic and social channels (Kearney et al., 2020). This suggests that individuals were more inclined to discuss the information they received with close associates, friends or relatives. Receiving false information about COVID-19 allowed some of the participants to have open and critical conversations with their peers, associates and relatives, which either clarified the information they received or raised doubts about the authenticity of such information, helping them to determine the appropriate action to take. Secondly, information is decontextualized, recontextualized and repurposed as it moves from sources (people and platforms) to recipients and ordinary people. Decontextualization occurs when the intended meanings and details are distorted as information crosses platforms and is interpreted by individuals based on their cognition and pre-existing beliefs. On the other hand, when original information acquires new meanings and additional details are added, it is recontextualized; as a result, the information may become more complex and confusing. Repurposing is the process of (re)constructing the original information to fit a new agenda or to accomplish a completely different goal from the original source's intention. All of these contribute to the dissemination of health misinformation in a social milieu.
Verification and correction practices of young people
Some of the young adults were found to employ a range of distinct verification and correction strategies. One such strategy was an intentional practice of questioning the information they received, especially when it concerned a sensitive and trending issue such as COVID-19. The idea was to not easily believe every piece of information they came across. Such deliberate scepticism then morphed into curiosity to try to verify the authenticity of a particular message. Simple Google searches, subsequent searches on reputable local and international news platforms, or searches on the verified accounts of influencers they trusted on Twitter and Instagram are all examples of how such verification took place. They also used social listening or social eavesdropping as a method of verification and correction. This involved having conversations with knowledgeable individuals in their social support networks or acting as knowledgeable individuals themselves to spread accurate information within their close networks. The advantage of this lies in the ability of young individuals to question each other's assumptions, enlighten one another on contentious topics and debunk any erroneous knowledge they may have previously held. However, there was a prevailing perception that individuals with expertise often lack the motivation or exert minimal effort to disseminate accurate information or refute false information, both online and offline. In contrast, mis/disinformers exhibit audacity, intentionality and cruelty in their deceptive tactics.
Personal experience was another interesting way for young adults to verify information; however, only a small proportion of them reported doing so. For example, if they read that drinking hot water infused with ginger, garlic and other herbal components treated or prevented COVID-19, they tried it for themselves. If they heard that having the vaccine made you emit electric currents, they got vaccinated to find out for themselves. One participant in Apo, Abuja, described how, when it was announced that vaccination would begin in the country, her mother sent her a YouTube video of ‘two soldiers who claimed they were vaccinated’ putting a light bulb on their body and producing an electric current or light. The video went on to say that such a current would emerge when people get vaccinated. Because of this, the participant's mother angrily urged her not to be vaccinated. This participant, adamant in believing the story, tried to carefully study the video to pick up anything unusual or tricky. She found nothing. Still unsatisfied, she ‘visited a friend whose cousin is a doctor’. She further narrated: So I brought up the video. The doctor brought a bulb and put it on his hand, and it brought out a light, and he wasn’t vaccinated. I now asked, how come? He explained the science behind it and that it was normal, not an issue of vaccine. So I had to tell my mum, even though she still insisted it was still real. (FGD, Participant 6, Apo, Abuja)
A similar account was shared by another participant in Abuja, who, when encountered the spurious story of people emitting an electric current from their bodies on YouTube, ‘felt that something was off, especially how they cut the video off’ and then took steps to verify this information and found from online searches that the information was a hoax. I just went on YouTube and searched for the video and put on the subtitle and I noticed that the video said vaccinated, but the subtitle said unvaccinated. So, I went on Google again and searched again. (FGD, Participant 5, Apo, Abuja).
Familial misinformation was therefore not uncommon. Many of the young people shared stories of how their relatives—parents, grandparents and siblings—were conduits through which they interacted with a lot of viral fake news on COVID-19, including varying attempts to influence their behaviour and attitudes towards the virus, its spread, vaccines and other aspects of the pandemic (this is corroborated by the findings from Duque and Peres-Neto, 2022). Beyond employing personal verification and correction strategies, the young people showed minimal awareness or utilization of formalized fact-checking methods such as using fact-checking sites. A significant number of the participants were unfamiliar with existing fact-checking sites and organizations.
Interdependencies: Understanding factors underlying youths’ engagement with health misinformation (RQ2)
The intricate dynamic of the spread of (mis)information is reinforced and activated by the notion of ‘interdependencies’, which helps to explain young individuals’ engagement with misinformation. The analysis uncovered a series of interconnected relationships in the young adults’ engagement with misinformation in general, and specifically with health misinformation. There was an interdependence between the offline and online imaginaries and practices of young adults. The notion of interdependence is used loosely here to explain the impact of sociocultural-religious-political and human intermediaries, affect and interpellated ideologies, among others. Interdependencies underlie the various kinds of material, affective, social and political conditions that result in a range of behaviours, risk perceptions and dissemination of alternative truths and misinformation in a social setting. For example, if certain young people are exposed to misinformation about the 5G network and its alleged links to the ‘Mark of the Beast 666’ and COVID-19, they may proceed to discuss it with others with whom they share partisan, cultural or religious views. As a result, these individuals may engage in offline actions such as vandalizing 5G masts built by the government or telecommunications corporations.
Interdependence can be understood as directional communication, which can help to explain how false information moves from platforms such as WhatsApp and YouTube and trickles down to other places. This kind of reciprocity in the transfer of information from one source to another is crucial to understanding the ways in which contextual factors impact information reception, diffusion and transfer. Interdependence can also be seen as the co-creation of information and meaning by different groups; and in this study, we see how the young adults could co-create meaning out of information that they received, alongside relatives, close friends, associates and social media influencers.
From the data, one such interdependent factor is interpersonal or cultural intermediaries. This includes, as one participant put it, ‘those smaller groups where people come together’. Falade (2022) notes the influence of culture, social groups and social representations during health crises such as COVID-19. This highlights the importance of the social listening dynamic observed earlier in the data—a situation where the young adults relied on others for the diffusion of information, and, at the same time, could play the role of information diffusers themselves. Such engagement fostered trust and built a sense of community, providing opportunities to engage in honest, practical, peer-to-peer discussions that clarified, legitimized or challenged the messages they received, and enabled them to work with others to find accurate information about an issue relating to the COVID-19 pandemic. I believe word of mouth is even more powerful than social media. If you see someone trying to convince another person of what they themself have little or no idea of, you see how powerful it is. They will say a lot of catchy words, a lot of lies to just make it more powerful. (Personal interview, Participant 2, Lagos Island, Lagos)
Religion plays quite an important role in a conservative and deeply faith-based country like Nigeria (Uzuegbunam, 2021). Religious leaders are often seen as persuasive opinion leaders whose words are respected and taken as sacrosanct by congregants and followers. In the case of COVID-19 pandemic, these religious influencers shaped the kinds of imaginaries and narratives spreading about the pandemic, eventually affecting the kind of risky or safe behaviours people adopted. They did this by disputing the reality of the virus, influencing citizens’ adherence to science-based health guidelines and whipping up sentiments around vaccines and vaccination, thereby increasing the number of people with vaccine hesitancy (see Falade, 2022; Obadare, 2022).
Politics is a crucial aspect to consider when examining how individuals are affected by false information in general (Dhawan et al., 2021; Neyazi and Muhtadi, 2021), as it is interconnected with other factors. The data revealed a conspicuous lack of faith in the government and its agencies, to the extent that the pandemic was widely believed to have been politicized. For example, there were numerous allegations from the participants that the pandemic was a political hoax. According to their assertions, the government and its agencies (referred to as a ‘community of liars’ by one participant) allegedly gained benefits from the pandemic and received foreign assistance. However, they allegedly manipulated the data to exaggerate the severity of the crisis, with the intention of prolonging the pandemic hysteria. The young individuals criticized the government and its agencies for hoarding and withholding social palliatives, primarily food items, supplied by benefactors and NGOs. Similar to religious scepticism, individuals who harboured doubts about the government and its authorities were more prone to disregarding health advice and actively disseminating misinformation. This encompassed marginalized demographics. Conversely, a study conducted in the Western countries of the USA, UK, France and Canada did not find evidence to support the belief that being exposed to false information weakens faith in the government or the media (Boulianne and Humprecht, 2023). They have politicized everything, that way, we have lost trust in them. Even when something is good for us, we don’t trust that they are telling us the truth because, over time, they have lied to us … I just feel our politicians have given us the room not to trust them; even when they are telling us the truth, we just don’t believe it or we think it is politics. (Personal interview, Participant 6, Apo, Abuja)
The data also indicated widespread acceptance of the effectiveness of traditional (herbal) medicine. This further reinforces the notion that various sociocultural, religious and political factors can impact the dissemination, reception, cognition and adherence to information during a critical period such as a health crisis. The participants acknowledged that these conventional remedies are highly favoured by specific demographics, especially in rural and peri-urban regions. Consequently, individuals may develop the misconception that consuming these remedies gives them immunity against the virus. During the pandemic, numerous traditional healers emerged, asserting the effectiveness of their herbal mixtures for preventing or treating the virus (Atuire et al., 2021). Some individuals considered science-based medical knowledge to be equally credible and followed it as closely as they did traditional medicinal practices. The participant narratives showed that during the pandemic it was possible for individuals to use masks, sanitize and adhere to social distancing rules, but at the same time, prioritize their routine of consuming hot water infused with herbal blends such as ginger, garlic, honey or other traditional herbs.
The social hierarchy in which young people were positioned also influenced their receptiveness or scepticism towards misinformation in general. Individuals from middle-income backgrounds, accustomed to accessing reliable and high-quality information, were less prone to accepting and spreading false information. In addition, the data revealed the impact of affect and emotions, as seen in the way the young adults vividly and affectively discussed their experiences of the pandemic and behaviours around health (mis)information. Assessing the significance of affective fluxes and emotional elements is crucial in understanding the interconnectedness of individuals’ experiences and behaviours (Lünenborg and Maier, 2018). In scholarly questioning of social phenomena, affective and emotional elements are sometimes overlooked; and in the case of fake news, a related social and democratic issue is that it is frequently deliberately affective (Bakir and McStay, 2018). According to Shafak (2022) in her TED Talk ‘The revolutionary power of diverse thought’, ‘analysts and experts are so busy with data and metrics that they seem to forget those things in life that are difficult to measure and perhaps impossible to cluster on the statistical models’. Humans are intrinsically emotional beings, and emotional factors often manifest in many human decisions, behaviours and practices. People may become misinformers or disinformers based on affective factors such as anger, fun, frustration, anxiety and fear; these may be ever shifting and can often block people's sense of reasoning or realizing the consequences of spreading false, incomplete or unverified information.
Combating health misinformation (RQ3)
How, then, do young people imagine the solutions for combating and dealing with health misinformation? First, there was widespread acknowledgement that ‘you just cannot control these things’ (FGD, Participant 5, Apo, Abuja) and that there is a long way to go in doing so, implying the sheer challenge of combating the impact of false information and the difficulty of controlling its spread. The participants recommended that the government prioritize becoming more responsive, proactive and transparent in order to rebuild trust with the people, which has been repeatedly undermined. Research findings indicate that stakeholders should prioritize persons with low levels of trust, since they are more inclined to actively seek information, increasing their susceptibility to encountering unverified and unofficial information (Kim et al., 2024). Likewise, the local traditional media were perceived to be just as unreliable as the government and politicians. In order to effectively disseminate important information to citizens in rural areas, it is imperative for the government and relevant agencies to work together and establish specialized awareness and information centres.
Additionally, utilizing mainstream media platforms to convey these crucial messages and translating health information into local languages, rather than solely relying on English, was considered to be beneficial. The participants’ suggestions corroborate the findings of existing studies (see Adekunle and Mohammed, 2022; Adjin-Tettey, 2022). In addition, the participants viewed it as imperative for government officials and health organizations to actively utilize both traditional and online media platforms to combat and debunk misinformation as soon as it emerges; research shows that social media platforms provide an important boost to government communication during a health crisis (Adikpo, 2022). Meanwhile, participants noted that mainstream media outlets have a duty to verify and thoroughly investigate news related to sensitive topics, rather than prioritizing being the first to report news stories, which could lead to important details being overlooked.
The analysis also demonstrated the importance, from the young people's perspective, of the role of social media platforms in flagging and debunking misinformation in general. Popular platforms such as Facebook, Twitter and Instagram were considered to be crucial to enforcing social media censorship, content moderation and other punitive measures recommended by the participants as potential solutions to be achieved in partnership with agencies such as the United Nations and the WHO. The participants also believed that influential opinion leaders from faith-based and cultural groups, public figures, social influencers, experts and researchers could act as intermediaries, collaborating with the government and appropriate agencies to disseminate accurate, verified information to citizens. This aligns with the principle of social listening by the government and critical stakeholders. The WHO endorsed social listening as a beneficial kind of infoveillance that can help infodemic managers sift through the ‘noise’ and locate specific relevant content to help in infodemic management efforts by different parties involved. This would involve observing and examining discussions to guide strategic actions, both on the internet and in person—an increasingly vital element of risk communication and involvement initiatives, especially in African countries (Sommariva et al., 2021).
Citizens themselves can also play a role in practising ethics of care in sharing information, especially information that they are not sure of or have not verified and, in turn, educating other people. However, a significant issue arises: it is difficult to control what people put out in the public domain as access to the internet and social media has meant that everyone and anyone can use the internet for any disingenuous agenda or intent. Additionally, peer-to-peer correction (Bode and Vraga, 2021) and citizen fact-checking could be useful in combating the spread of health misinformation by leveraging the collective vigilance of the community. This can also contribute to a more informed public discourse and foster a culture of critical thinking and media literacy. At times, people send this information without even knowing. Like my mum sent me some very weird messages. I was like ‘where did you get this information from?’ She told me that is from church WhatsApp group. So you really have to educate her. (FGD, Participant 8, Lagos Island, Lagos)
Media and information literacy was also acknowledged as one way of combating misinformation. The COVID-19 pandemic has prompted global interest in activating or enhancing people's competencies in cultivating critical thinking skills, as well as understanding, evaluating and using media for combating the impact of misinformation (Frau-Meigs, 2022; Singh and Banga, 2022). Media literacy was defined by one participant as ‘the ability to take what you see in the media and analyse it and know that this is what I should do or if I should believe it or not. That means you have power over the media and not the media having power over you’ (Personal interview, Participant 1, Lagos Island, Lagos). However, one participant noted what they thought of as ‘the death of media literacy’ in a media world constantly undergoing rapid changes. By this, they meant that many people, especially the aged population, do not have the capacity ‘to filter what they get from the Internet’ (FGD, Participant 6, Apo, Abuja). However, there is research evidence pointing to the importance of moving beyond a general idea of media literacy to news literacy, since ‘news literacy is generally oriented around critical thinking skills required for engaged citizenship’ (Ashley et al., 2022).
It is evident that age and level of education could play a role in information-sharing behaviours. A significant number of the young adults recounted instances where their older relatives, including their parents and grandparents, disseminated misinformation via WhatsApp and anticipated their unquestioning acceptance and subsequent action based on such information. When they attempted to rectify the situation or educate the older individuals, the latter perceived the young individuals as irrational for dissuading them from sharing specific types of information. Duque and Peres-Neto (2022) found that among the aged, sharing of (mis)information is motivated by active ageing and reinforced by the local cultural context, where sharing is seen as a form of participation. A participant argued that formal education does not guarantee immunity to erroneous information, despite some studies (Martínez-Costa et al., 2022; Uzuegbunam and Ononiwu, 2023) finding that individuals with a higher educational level were more confident in their own immunity.
Fact-checking was not a popular practice among the young people, as many of them were unaware of the existence of fact-checking sites and platforms in Nigeria, and they did not make use of them in their verification strategies. Some mistook social Q&A sites like Quora and health information sites like Mayo Clinic as fact-checking platforms. A growing number of fact-checking organizations have emerged in parts of the African continent (Cunliffe-Jones, 2021). Several fact-checking organizations operate within the Nigerian context, with the main ones including Africa Check Nigeria, which is a subsidiary of Africa Check; Viral Facts Africa, a network of public health institutions and fact checkers providing fact-based medical information; CDD Fact Check, the fact-checking arm of the CDD; Fact Matter Nigeria, aimed at promoting information integrity with the support of the International Centre for Journalists; Dubawa, Nigeria's independent verification and fact-checking platform; and Fact Check Hub, the verification platform of the International Centre for Investigative Reporting. Studies have shown that expert factcheckers can play a role in verifying, validating or debunking information (Alsmadi et al., 2021; Burel et al., 2021); however, despite the proliferation of these fact-checking and verification platforms in the Nigerian context, their impact in combating information disorders in this context appears to be minimal, as also demonstrated elsewhere (Burel et al., 2021).
Conclusion
This study has explored the consumption, dissemination and combating of health misinformation related to COVID-19 by young adults in Nigeria, as well as the interdependencies underlying these practices in the local context. By focusing on the youth demographic and taking a sociological approach, this study provides a useful insight into how this specific social grouping makes sense of health misinformation and how health information targeting young people could potentially be packaged and disseminated. The notion of interdependencies is explored here in relation to how sociocultural intermediaries, religious and political actors, and socioeconomic conditions significantly influence perceptions and behaviours, thus emphasizing the need to consider these factors when designing health interventions. As in many parts of the world, Nigerian young adults encountered a large amount of COVID-19 misinformation. While previous studies suggest that susceptibility to health misinformation appears to be driven by different psychological processes, and interventions need to be developed based on an understanding of these factors, the present study argues that sociocultural, political and religious interdependencies, especially in African contexts, need to be seriously considered and studied.
Young Nigerian adults’ experiences of health misinformation and its impact cross familial, interpersonal, societal and personal boundaries. Practices of social listening, decontextualization, recontextualization and repurposing underscore the complexity of information flow in a digital age. These processes not only facilitate the spread of misinformation but also offer opportunities for critical engagement and dialogue on how to better equip individuals to navigate and combat the impact of false information, resulting in a more informed and resilient society. The findings align with aspects of the WHO's (2021) public health research agenda for managing infodemics (misinfodemics and disinfodemics), notably those in relation to the pandemic, with the aim of fostering evidence-based intervention, albeit from a sociological dimension.
Given the findings of this study, we see that it is crucial for governments to treat health misinformation seriously, rather than dismissing it as the negative consequences of a growing digital environment, enacted by unscrupulous, partisan citizens. By doing so, it would be possible for governments to formulate responses that go beyond simply sharing accurate facts and take into consideration the underlying feelings of distrust, which may vary greatly among different communities and demographics (Gagliardone et al., 2021). According to Inyabri et al. (2021), Nigerian youth as a key social grouping are filled with mistrust and harbour profound disillusionment with political elites and the state. This is largely due to a failing educational system, a weak and corrupt judiciary, an inadequate healthcare system, moribund infrastructure and lack of social security.
From a theoretical perspective, the social cognitive framework has been valuable in examining how urban youth in two major Nigerian cities navigated health misinformation that circulated during the COVID-19 pandemic. Young people's experiences in Nigeria during the COVID-19 pandemic provide insight into their cognitive processing of the health crisis; they appear to be a cognitively independent, self-regulating and contemplative demographic. Rather than being passive recipients of external or internal influences, they were proactive architects of their own health behaviours and outcomes. This study shows that media consumers, especially young adults, possess the ability to make reasoned decisions about the information they receive, even if it is inaccurate. This is influenced by several interdependent elements in their everyday lives. The theory could be used to explore the perceptions and behaviours of young people in Nigeria and other parts of sub-Saharan Africa in response to other common disease outbreaks such as monkey pox, Lassa fever and others, as well as those of other significant demographic groups. These will also need to be assessed with consideration of the sociocultural, political and religious interdependencies.
Footnotes
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by a grant from the Carnegie Corporation of New York (DEAL2 Fellowship) at the Institute for Humanities in Africa, University of Cape Town.
Author biography
Chikezie E Uzuegbunam is a Senior Lecturer, MA Programme Coordinator, Deputy Head of School, and Chair of Research Forum at Rhodes University's School of Journalism and Media Studies. He is a rated researcher by the National Research Foundation of South Africa. Dr Uzuegbunam holds a PhD in Media Studies from the University of Cape Town and multiple degrees in Mass Communication from Nnamdi Azikiwe University in Nigeria. He was an inaugural Carnegie Fellow at the Institute for Humanities in Africa and holds similar other fellowships such as ASA/Carnegie Fellow for two consecutive years (2023 and 2024). He is also a Global Fellow at Northwestern University's Institute for Advanced Study in the Global South in Qatar (2024–2025). He has published dozens of peer-reviewed works on topics like digital culture, children and youth, cultural studies, generative AI and misinformation. His first book, Children and Young People's Digital Lifeworlds: Domestication, Mediation and Agency, was published in 2024 by Palgrave Macmillan.