
Abstract
Deep brain stimulation (DBS) is considered as a treatment option for many neurological diseases. Many patients with movement disorders exhibit remarkable improvement after DBS. Owing to its minimally invasive nature, reversibility, and adjustability, DBS has been increasingly used over the past several decades. Dystonia is one of the most common movement disorders among children, and there is no effective treatment. Recently, some surgeon groups have performed DBS surgery for children. However, the outcomes of DBS in children are not well characterized. Here we mainly discuss the efficacy of DBS against childhood-onset dystonia and introduce the main procedure of pediatric DBS based on our own experience.
1 Introduction
The first documented deep brain stimulation (DBS) procedure was performed by Benabid et al in 1987 to treat a patient with Parkinson’s disease (PD) [1]. Subsequently, DBS has been used to treat numerous neurological disorders. To date, the US Food and Drug Administration (FDA) has approved the use of DBS for treating PD, essential tremor, obsessive-compulsive disorder, and dystonia. In addition, the use of DBS for the treatment of refractory epilepsy was approved in Europe in 2010 [2]. An increasing number of researchers are investigating the use of DBS for the treatment of other diseases, such as chronic pain, Alzheimer’s disease, depression, and Tourette syndrome. The therapeutic efficacy of DBS is comparable with that of traditional surgeries; in addition, DBS offers the advantage of adjustability of stimulation and reversibility of any adverse effects. Although DBS has been widely used, the mechanisms underlying its therapeutic efficacy remain poorly understood. Several hypotheses have been proposed in this respect [3], such as the “classic rate model” “jamming theory” and “bursting”.
The technological innovations and scientific advances in the past several decades have led to a rapid increase in the applications and studies of DBS. However, despite the great advantages of DBS in the treatment of movement disorders, its use in children remains relatively rare. The Peking University First Hospital (PKUFH) is one of the organizations that pioneered the use of DBS in children with dystonia in China. To date, more than a dozen children with dystonia have been treated using DBS by the surgical group for pediatric movement disorders at the PKUFH.
Dystonia is a neurological disorder characterized by sustained or intermittent muscle contractions that results in abnormal, involuntary twisting movements or postures [4, 5]. Dystonia is one of the most common movement disorders among children; the disorder has negative impacts on growth and development, daily activities, and school performance. There are many causes of dystonia, including genetic mutations, cerebral palsy (CP), and inherited metabolic diseases. Currently, there is no cure for dystonia; the results of pharmacological management appear to be unsatisfactory. Owing to the rapid development and widespread application of DBS, surgeons have used this minimally invasive surgery to treat patients with dystonia and have been successful to some extent. Ever since Coubes et al. first used DBS for the treatment of dystonia [6], it has been gradually accepted as an optional treatment for childhood dystonia. Interestingly, children with DYT1 dystonia respond particularly well to DBS, with greater improvement than non-DYT1 patients [7]. However, owing to the limited documented experience on DBS for childhood dystonia, the role of DBS in other types of dystonia remains unclear.
In this review, we discuss the role of DBS in the treatment of dystonia and describe our experience with DBS for the management of childhood dystonia.
2 DBS for dystonia
Clinically, dystonia is mainly classified according to three criteria, i.e., etiology, age at onset, and body distribution [8]. The most widely accepted classification in the literature categorizes dystonia into two main types [9]: primary dystonia (dystonia is the only clinical sign and includes idiopathic or genetic disorders with no neuropathological abnormalities) and secondary dystonia [dystonia arising from neurodegeneration, acquired causes (such as lesions within the brain), or genetic conditions with a progressive course]. Although the recently published consensus classification provides a more detailed approach to distinguish dystonia [10], few published articles have used this classification.
2.1 Primary dystonia
There is a consensus that DBS is safe and effective for the treatment of primary dystonia in children [5, 11]. To date, 29 types of dystonia caused by monogenic mutations are recognized (DYT1– DYT29) [9, 12]; of these, the initial symptoms of DYT1–6, 11, 12, and 25–29 are noticeable during childhood or early adulthood. DBS has been used as an alternative treatment for several types of DYTs (Table 1).
Effect of DBS in patients with early-onset primary dystonia.
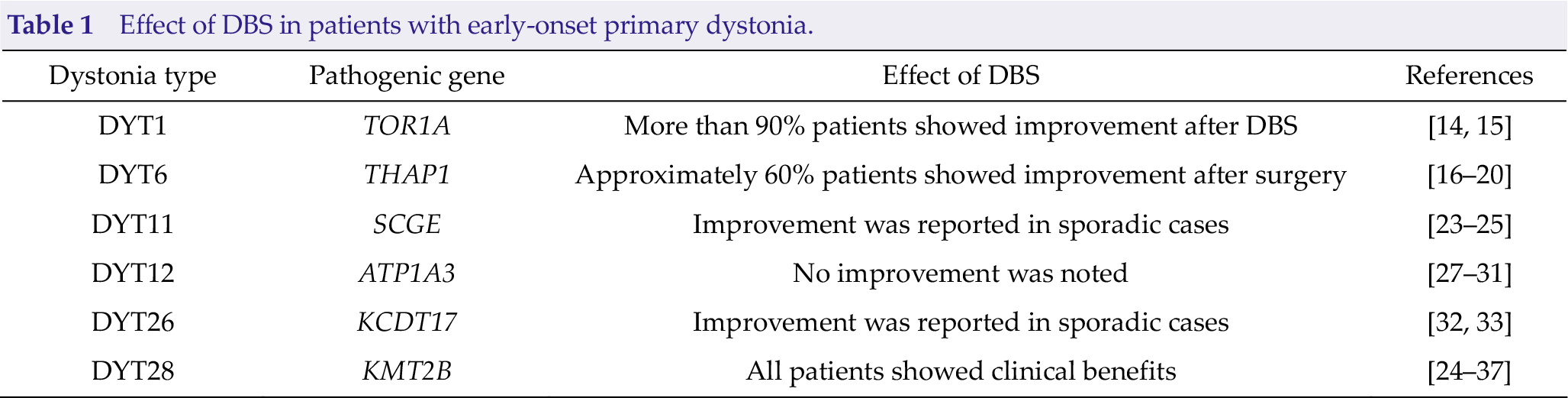
DYT1 was the first discovered primary dystonia and is caused by the torsin-1A (TOR1A) gene, and it is the most commonly reported primary dystonia treated using DBS [13, 14]. Patients with DYT1 typically present with dystonia since childhood or adolescence; the condition initially affects a single limb and often progresses to general dystonia within 1~3 years. According to some reports, DYT1 appears to show the best response to DBS among all dystonia types. Approximately 90% patients with DYT1 who underwent DBS experienced an average improvement of 60% in the 1st year after surgery, as assessed using the Burke–Fahn–Marsden Dystonia Rating Scale (BFMDRS) [14, 15].
DYT6 usually presents with dysphonia or writer’s cramp during late childhood or adolescence, and approximately 25% patients gradually develop craniocervical involvement. THAP domaincontaining protein 1 (THAP1) gene is the pathogenic gene of DYT6. Numerous cases of patients with DYT6 who underwent DBS surgery have been reported [16 –20]; the therapeutic efficacy was not as good as that observed in patients with DYT1 [14, 15]. Only 60% of patients with DYT6 experienced an average improvement of 30% in the first year following DBS, as assessed using BFMDRS.
DYT11, also known as myoclonus-dystonia, is characterized by the involvement of the neck or arms/hands during childhood or early adulthood. The condition has an autosomal dominant inheritance with pathogenic mutations in the sarcoglycan epsilon (SCGE) gene. Alcohol tends to relieve myoclonus to a large extent [21], and some drugs, such as zonisamide, may ameliorate the symptoms [22]. In addition, several research groups have reported that patients with DYT11 also respond to DBS [23 –25]. DBS could be an optional treatment for some refractory cases because it may result in 50% improvement.
DYT12 is characterized by sudden-onset dystonia–parkinsonism during adolescence or early adulthood; ATPase Na+/K+ transporting subunit alpha 3 (ATP1A3) is the causative gene for this disorder [26]. Several reports have described trials of DBS in patients with DYT12; however, none of the patients showed satisfactory clinical effects [27 –31].
DYT26 is characterized by motor delay, onset of myoclonic jerks mainly affecting the neck and upper limbs, and progression to dystonia [32–33]. In 2015, the gene encoding potassium channel tetramerization domain-containing 17 (KCDT17) was shown to be associated with this type of dystonia [32]. An excellent response to DBS was reported [33].
DYT28 is caused by pathogenic mutations of the lysine specific methyltransferase 2B (KMT2B) gene. The characteristic feature of this disorder is childhood-onset generalized dystonia. More than a dozen patients with DYT28 reportedly showed clinical response to DBS [34 –37]. Younger patients with DYT28 showed improved responses to DBS, and some of them regained the ability to walk without support after surgery.
DYT3 and DYT25 typically present during late adulthood; however, some cases may present earlier [14]. Several reports have demonstrated that patients with DYT3 and DYT25 respond to DBS [38 –41]. However, DYT2, DYT4, DYT27, and DYT29 seem to be extremely rare entities, and we were unable to find any definitive evidence of their responses to DBS.
2.2 Secondary dystonia
The most common causes of secondary dystonia include CP, pantothenate kinase-associated neurodegeneration (PKAN), and inherited metabolic diseases. In this section, we mainly discuss the efficacy of DBS for the treatment of patients with CP, PKAN, and glutaric aciduria type 1 (GA1).
Patients with CP exhibit four major types of motor dysfunction, including spastic, dyskinetic, ataxic, and mixed [42]; among these, dyskinetic CP is one of the most common causes of earlyonset dystonia. Multiple research groups have performed DBS in patients with dyskinetic CP; however, the clinical results were inconsistent. In a recent meta-analysis of data of 59 patients with CP, the median postoperative improvement in BFMDRS motor and disability subscale scores was 11.1% and 3.5%, respectively [11]. However, Romito et al. reported good long-term (up to 6 years after DBS) effects of DBS in patients with dyskinetic CP (approximately 50% improvement at the last follow-up) [43].
PKAN is a rare autosomal recessive disorder caused by pathogenic mutations of the pantothenate kinase 2 (PANK2) gene. The main clinical manifestations of PKAN are childhood dystonia, dysarthria, rigidity, and an “eye-of-tiger” sign on MRI. Only a few reports have described the use of DBS in patients with PKAN, with some degree of improvement [44, 45].
GA1 is an inherited metabolic disease caused by the Glutaryl-CoA dehydrogenase (GCDH) gene. Several reports have focused on the efficacy of DBS against GA1. To date, approximately 10 patients with GA1 have undergone DBS [46 –50], and no obvious improvement was achieved after surgery.
In addition, disorders such as kernicterus and Lesch–Nyhan disease (LND) may also present with acquired dystonia. A few case reports have documented unsatisfactory results of DBS in patients with such types of acquired dystonia [5].
3 DBS management for childhood dystonia
DBS surgery in children is very different from that in adults. Herein, we discuss the procedure for DBS in children and introduce some of our own experiences (Fig. 1).
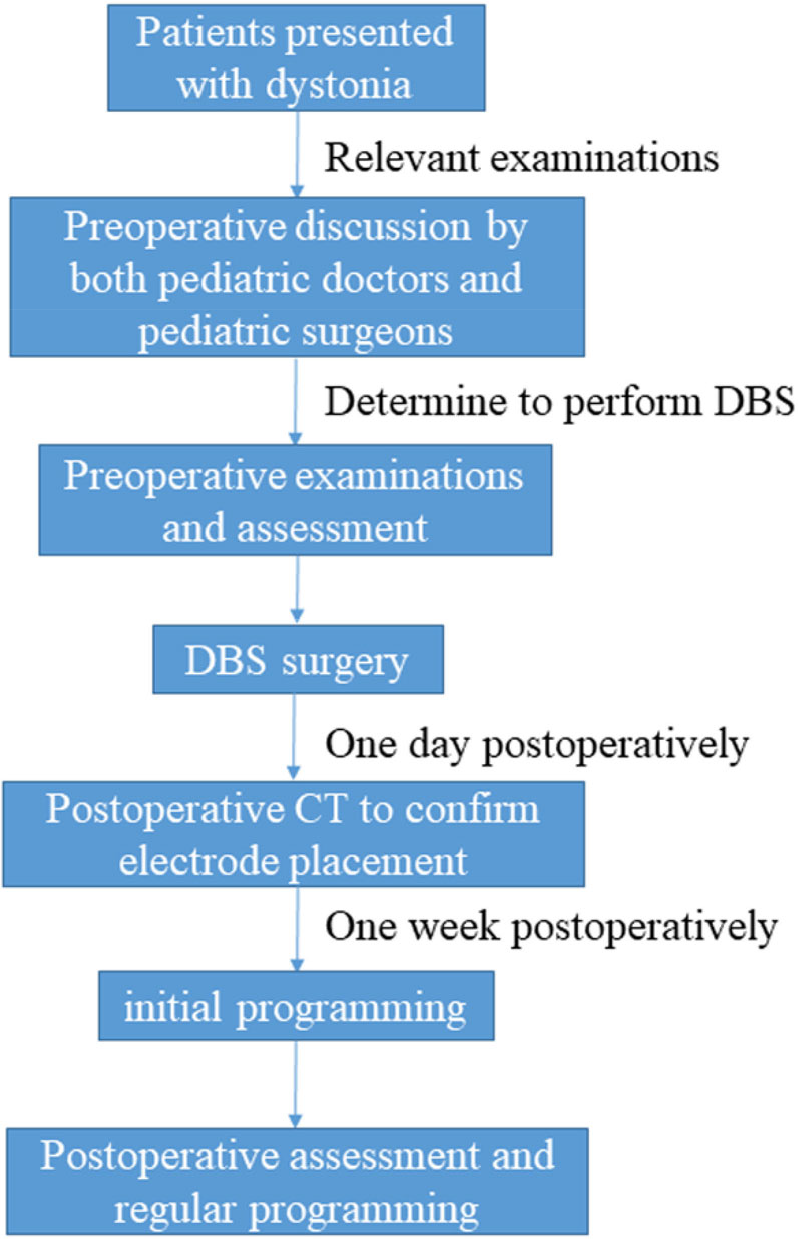
The procedure of pediatric DBS at our center.
3.1 Preoperative preparation
First, we seek to determine the etiology of dystonia as a collaborative effort involving the departments of pediatrics and pediatric surgery. For patients with no clear cause of dystonia, we recommend whole-exome sequencing or panel sequencing to identify the underlying diseases and help predict the efficacy of DBS. Subsequently, pediatric doctors and pediatric surgeons collaboratively discuss whether DBS should be performed in that patient. If surgery is decided upon, preoperative evaluation of dystonia severity is performed using BFMDRS; in addition, a video recording of the patient’s status is saved. Unlike adults, children are unable to accurately express the postoperative changes; therefore, a more detailed assessment should be performed.
3.2 Surgical procedure
Preoperative MR images are required for target localization, and a professional workstation is used for image infusion and surgical planning. Unlike in adults, in children, DBS is always performed under general anesthesia with endotracheal intubation [50]. The leads and pulse generator are placed at the appropriate sites, as described previously [48]. The US FDA has approved globus pallidus internus (GPi) as a target for pediatric DBS [14]. However, a recent study has shown that the subthalamic nucleus (STN) could also be an effective target for DBS for patients with dystonia [51]. CT is performed after surgery to verify the precise location of the lead.
3.3 Programming and postoperative evaluation
DBS programming at our institution typically starts 1 week postoperatively, after confirmation of the lead position by CT. Patients are instructed to stay at the hospital for approximately 7 days after the surgery to facilitate regular monitoring of wound healing and any adverse events. Routine follow-up, comprising neurological examination, dystonia severity evaluation, and programming, is performed at 1, 3, and 6 months after surgery. Subsequently, all patients are reassessed every 6 months. Based on the feedback from patients or their parents, the stimulation parameters are adjusted to achieve better clinical outcomes or to reduce the adverse events. Furthermore, the patients have access to a remote control system for adjustment via the internet. Moreover, because pediatric DBS is often performed in patients with general dystonia, postoperative rehabilitation training is also recommended for these patients.
4 Conclusion
In this review, we discussed the efficacy of DBS against various types of early-onset dystonia. The majority of patients with primary dystonia show good response to DBS; however, additional evidence is required to confirm the efficacy of DBS in patients with secondary dystonia. To the best of our knowledge, most patients with secondary dystonia show poor response to DBS. However, several reports have indicated that the clinical effects tend to be unstable in the early postoperative period; therefore, there is a need to monitor the long-term effects of DBS in these patients. Additionally, based on our own experiences, we briefly introduced the main procedure for DBS performed in children, which is slightly different from that performed in adults.
Footnotes
Conflict of interests
All contributing authors have no conflict of interests.