
Abstract
Objective:
To explore the usefulness of multishot diffusion tensor imaging (DTI) for evaluating the neurological function of patients with spinal cord tumors
Methods:
Routine magnetic resonance imaging and multishot DTI were performed in five patients with spinal cord tumors. The values of fractional anisotropy (FA) and radial diffusivity (RD) were analyzed.
Results:
Multishot DTI of spinal cord tumors allowed for defining the margins of tumors and determining the relationship of tumors with the adjacent white matter structures of the spinal cord. Multishot DTI demonstrated significantly increased RD and decreased FA of spinal cord tumors compared with those of the normal spinal cord.
Conclusions:
Multishot DTI is a potentially useful modality for differentiating resectable tumors from nonresectable ones based on preoperative imaging alone as well as for differentiating intramedullary tumors from extramedullary ones. Further prospective studies are warranted to confirm these results.
1 Introduction
Cervical spinal cord tumors are common. Despite advances in microsurgical and neurophysiological techniques, intramedullary spinal cord tumor resection remains challenging, and histological type is the primary predictor of tumor resection. Although magnetic resonance imaging (MRI) enables the early detection of spinal cord tumors, this modality often provides inaccurate predictions of histological types. Multishot diffusion tensor imaging (DTI) is a potentially useful for differentiating resectable tumors from nonresectable ones based on preoperative imaging alone as well as for differentiating benign tumors from malignant ones. DTI can provide functional information regarding the spinal cord and contribute to the diagnosis and evaluation of spinal cord tumors. However, conventional single-shot DTI produces scans with low resolution and geometric distortion. Meanwhile, multishot DTI can effectively improve the resolution and reduce the geometric distortion. The new multishot DTI technology was first used in patients with cervical spondylotic myelopathy [1 –3]. In this study, we applied this technology in patients with spinal cord tumors. The aim of this retrospective study was to evaluate the usefulness of multishot DTI for predicting tumor resectability and differentiating intramedullary tumors from extramedullary ones. Of note, while conventional multishot DTI is mostly performed in the sagittal plane, multishot DTI in this study was performed in the axial plane as well.
2 Methods and materials
2.1 Baseline patient characteristics
The present study included five patients (three males and two females; age, 34~64 years) with spinal cord tumors; three patients presented with extramedullary tumors and two with intramedullary tumors. The diagnoses were ependymoma in two patients, ganglioneuroma in one patient, schwannoma in one patient, and cavernous hemangioma in one patient. The tumors were located in the cervical spinal cord in four patients and in the thoracic spinal cord in one patient. All patients underwent preoperative multishot DTI, and one patient underwent postoperative multishot DTI as well. Baseline patient characteristics are summarized in Table 1.
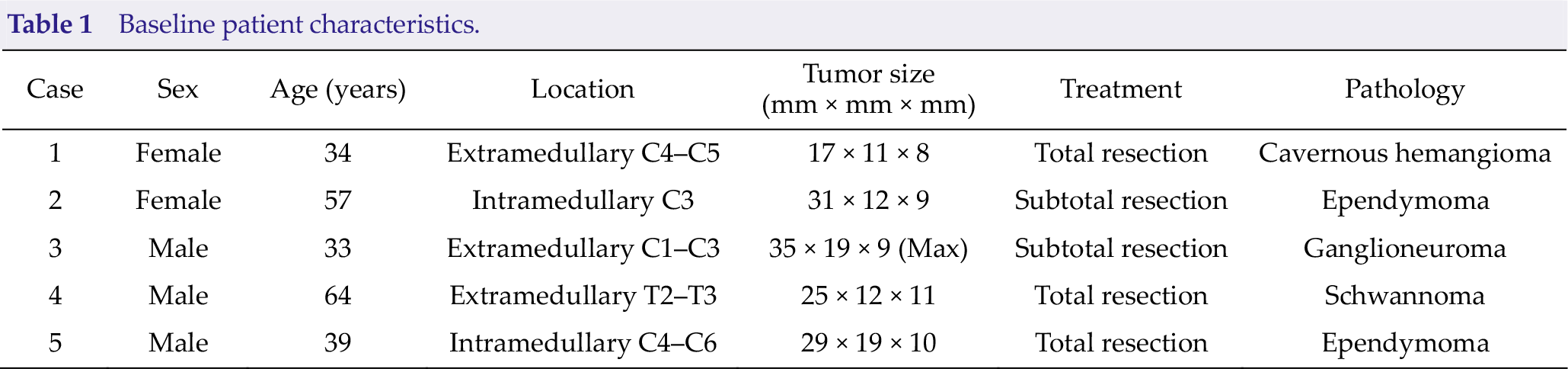
Baseline patient characteristics.
2.2 Multishot DTI parameters
The tumors showed different levels of spinal cord compression and infiltration. All patients underwent MRI using Philips 3.0T Achieva TX (Philips Healthcare, Best, The Netherlands). Detailed scanning methods were based on the multishot DTI technology used first in patients with cervical spondylotic myelopathy [1 –3]. Specifically, DTI was performed in both sagittal and axial planes, and multiple excitation iEPI sequences with navigational data were used to suppress cerebrospinal fluid (CSF) pulsation artifacts (trigger delay = l00 ms). The sagittal scanning parameters were as follows: number of excitations, 10; b, 600 s/mm2; number of diffusion directions, 10; and number of layers, 5. The axial scanning parameters were as follows: number of excitations, 8; b, 600 s/mm2; number of diffusion directions, 15; and number of layers, 9~21. Due to the limitation in imaging time, the number of acquisition layers was small; therefore, the section with the most severe tumor compression was selected as the center of scanning in transverse DTI.
After image reconstruction [1 –3], DTI Studio was used to process and analyze the images, and DTI-related parameters such as fractional anisotropy (FA) and radial diffusivity (RD) were obtained. The specific level at which the tumors compressed the spinal cord was determined on the basis of T2WI and T1WI. FA values for tumors as well as for compressed and normal spinal cords were measured on axial and sagittal images (ROI, 4 voxels). ROI was placed at the center of the tumor, and uniform signal was maintained. FA and RD values were measured three times by choosing three different ROIs, and the average value was recorded. During measurements, areas adjacent to the tumors and the surrounding CSF were avoided.
3 Results
3.1 DTI scan quality
The DTI scan quality met the requirements for FA and RD measurements in all patients.
3.2 Image analysis
Image analyses of extramedullary tumors indicated that the spinal cord exhibited compression displacement primarily at the tumor site. On FA images, the spinal cord was dominated by blue signals, whereas the tumors showed mixed red, green, and blue signals. Conversely, image analyses of intramedullary tumors revealed tumors were expansive or infiltrating growth and the spinal cord was thickened at the site of tumor growth. Additionally, the signal in the medulla was abnormal. On FA images, the spinal cord showed mixed blue and dotted red and green signals.
3.3 DTI parameters of the normal spinal cord
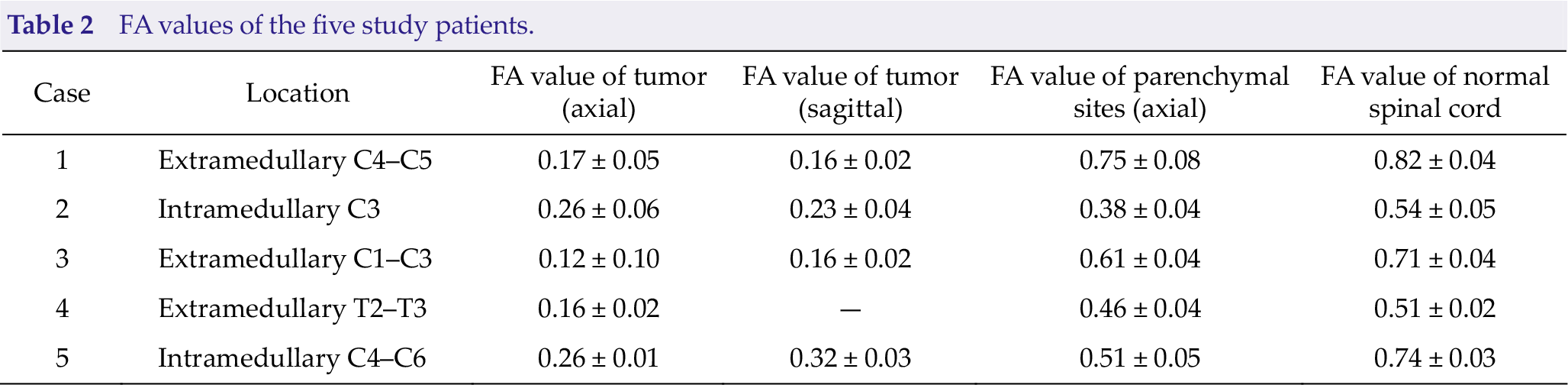
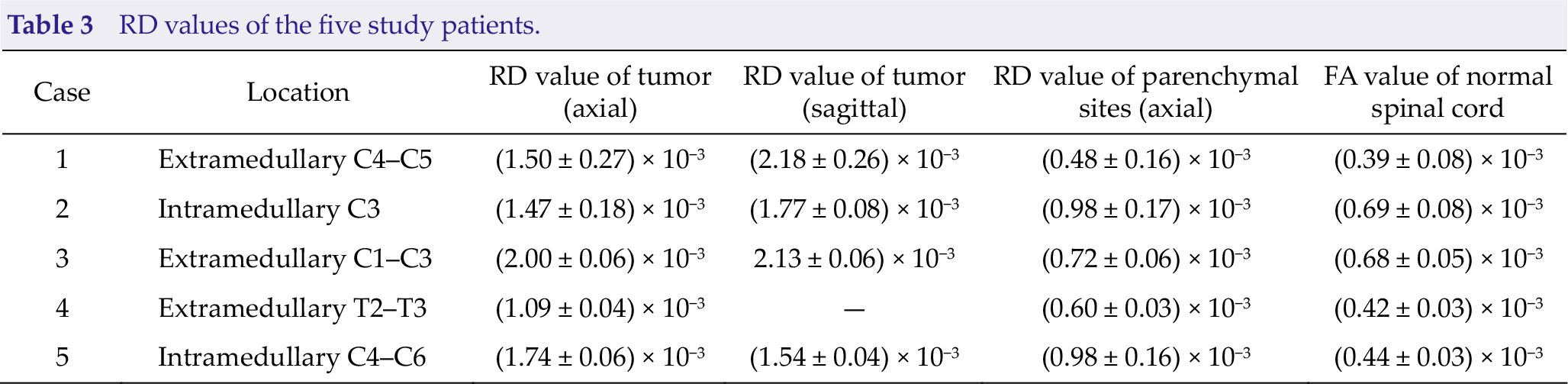
FA values of the normal spinal cord ranged from 0.51 ± 0.02 to 0.82 ± 0.04. RD values of the normal spinal cord ranged from (0.39 ± 0.08) × 10−3 to (0.69 ± 0.08) × 10−3; these values were similar to previously reported values [4–5]. Detailed data are presented in Table 2 and Table 3.
3.4 DTI parameters of the spinal cord tumors
Compared with those of the normal spinal cord, FA values of all spinal cord tumors were significantly decreased but RD values were evidently increased. Additionally, FA values were slightly decreased in the areas of the normal spinal cord close to the extramedullary tumors and significantly decreased in the areas of the normal spinal cord close to the intramedullary tumors. Detailed data are presented in Table 2. RD values were slightly increased in the areas of the normal spinal cord close to the extramedullary tumors and significantly increased in the areas of the normal spinal cord close to the intramedullary tumors. Detailed data are presented in Table 3.
FA values of the five study patients.
RD values of the five study patients.
3.5 Surgical outcomes and complications
Three patients underwent microscopic total resection, whereas the remaining two patients underwent near-total resection. Regarding complications, one patient developed persistent postoperative pain in the neck and shoulders, one patient experienced a decline in muscle strength, one patient developed sensory deficits including numbness and paresthesia.
4 Discussion
DTI can be used to evaluate spinal cord compression and destructive changes caused by spinal cord tumors. In this study, the FA value of areas of the spinal cord around the tumor was significantly decreased but the RD value was increased. DTI plays an important role in the differential diagnosis of intramedullary and extramedullary tumors. Fiber tractography (FT) can evaluate the damage to the spinal cord fiber bundles and guide surgical treatment and prognosis of patients.
Multishot DTI can effectively improve the resolution and reduce geometric distortion compared with conventional single-shot DTI. In this study, multishot axial scanning was used as well. In the study cohort of five patients, the imaging quality was good, without obvious distortion and deformation. On FA images, the spinal cord was dominated by blue signals, whereas the tumors showed mixed red, green, and blue signals. Our results demonstrate the utility of multishot DTI for evaluating the resectability of spinal cord tumors and differentiating intramedullary tumors from extramedullary ones.
In the present study, the FA values were significantly decreased in the parenchyma of intramedullary tumors and slightly decreased in the parenchyma of extramedullary tumors. Conversely, the RD values were significantly increased in the parenchyma of intramedullary tumors and slightly decreased in the parenchyma of extramedullary tumors. Accordingly, the spinal cord tumors could be roughly identified as being intramedullary or extramedullary based on the extent of changes in DTI parameters. The FA and RD values of intramedullary tumors were significantly altered and were consistent with the previously reported values [6 –8]. Ducreux [5] examined DTI results of five patients with intramedullary spinal astrocytomas (ROI, 10 voxels) and reported significantly decreased FA values at all tumor parenchymal sites, which might be attributed to extracellular edema, decreased number of fibers, or both. Liu et al. [9] examined 11 patients with spinal cord tumors (astrocytoma, ependymoma, and glioblastoma) and 10 patients with tumor-like lesions (multiple sclerosis, transverse myelopathy, and sarcoidosis) and reported significantly decreased FA values but significantly increased ADC values of tumors. The difference (FA and ADC values) between tumors and tumorlike lesions was statistically significant, indicating that the tumors caused more severe damage to the normal tissue structure. Our results suggest that DTI is of great value in the differential diagnosis of intramedullary and extramedullary tumors.
In the present study using multishot DTI, the scanning level was low; moreover, FT was not possible. However, as illustrated in the color FA value diagram (Fig. 1), the boundary between the extramedullary tumors and spinal cord fiber bundles was clear and the spinal cord fibers were completely displaced. The intramedullary tumors were not clearly separated from the spinal cord fibers; however, most of the fiber bundles were pushed out, and only a few of the fiber bundles were damaged. In the present study cohort, both intramedullary and extramedullary tumors were resectable, consistent with the literature [8, 10]. Setzer et al. [8] categorized intramedullary tumors into three types according to the fiber course: spinal cord fibers do not enter the solid tumor in type 1, some fibers enter the tumor but most of the tumor does not contain nerve fibers in type 2, and most of the tumor contains nerve fibers or tumors cause nerve fiber damage in type 3. Type 1 tumors are resectable, whereas type 3 tumors are nonresectable; however, it remains unclear whether type 2 tumors can be removed without residual neurological damage. The authors suggested that type 2 tumors are resectable only if < 50% of the tumor contains nerve fibers.
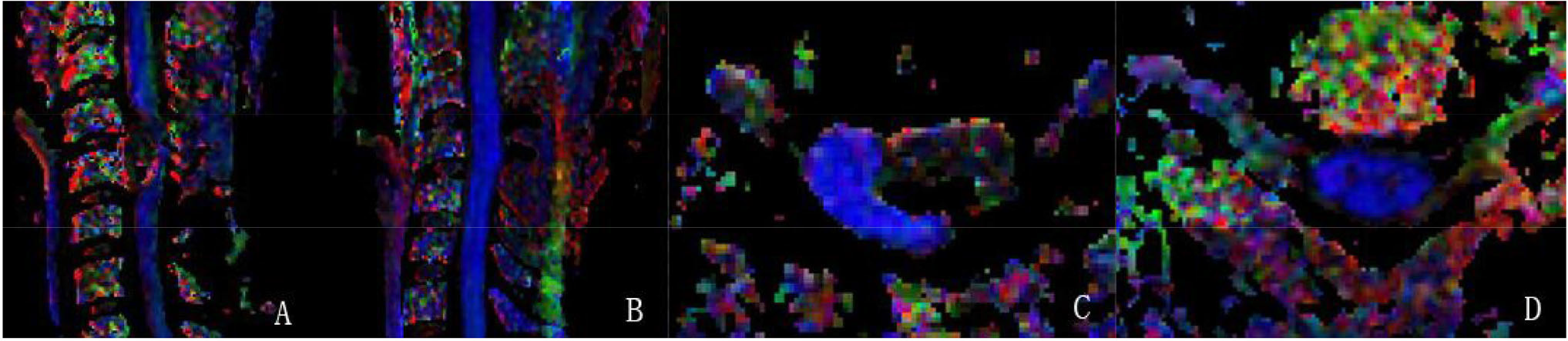
Representative images of multishot DTI in a 34-year-old female patient with C4–C5 extramedullary cavernous hemangioma. (A) Preoperative multishot DTI in the sagittal view: The compressed spinal cord is indicated in blue, and the tumor showed mixed signals. (B) At postoperative 3 months, multishot DTI in the sagittal view: The tumor was completely resected, and the spinal cord fiber imaging was intact without deformation. (C) Preoperative multishot DTI in the axial view: Spinal cord fibers were pushed posteriorly to the left by the tumor. The tumor showed a clear margin with the spinal cord fibers. (D) At postoperative 3 months, multishot DTI in the axial view:The quality of DTI is good, and the white and gray matters of the spinal cord are clearly visible.
FT is considered useful for predicting tumor resection; however, prospective studies are warranted to confirm this notion. Choudhri et al. [10] examined 10 patients with spinal cord tumors and proposed that FT can aid in determining tumor boundaries, assessing the tumor’s relationship with white matter fiber bundles, and predicting tumor resectability. A tumor with compressed and deformed white matter fiber bundles can be surgically removed. In conclusion, spinal fiber bundle imaging can aid in determining tumor resectability. If the fiber bundles are extruded or mainly pushed, complete removal of the tumor is possible. In contrast, complete tumor removal is difficult if the fiber bundles are clearly damaged.
FT cannot directly visualize fiber bundles. In the analysis of anisotropic objects, voxel value is much larger than the diameter of the axon and usually contains at least 100 axons. FT uses the FA value to indirectly display nerve fibers. In addition, the FA values of fibers in different directions in the same body element cancel one another. This is part of the volumetric effect, which makes it impossible to track the fiber bundles. If FA values in different directions do not completely cancel out, the tracked fibers may not exist. The FA threshold and angle are set based on the tracked nerve fibers; thus, FA does not always reflect the actual anatomical structures. The utility of FA is focused primarily on the cervical vertebrae. The imaging quality of the thoracolumbar segment is not good due to interference from respiration, heartbeat, and intestinal peristalsis. With the development of magnetic resonance hardware and software, DTI of the spinal cord may be useful for the examination of additional sites in and diseases of the spinal cord.
Footnotes
Conflict of interests
All contributing authors have no conflict of interests.